

A Survey on the Perception of Utstein Model and the Success of Resuscitation among the Chinese Medical Staffs
-
摘要:
目的 调查我国医护人员对乌斯坦因模式(Utstein model)的知晓情况及对复苏成功的评判标准。 方法 采用问卷调查的方式,对中国大陆医护人员进行随机抽样调查。 结果 仅有58.8%的参与者知晓乌斯坦因模式,知晓率与所在科室是否登记复苏结果关系最大,护士、男性、年轻人(< 40岁)、高级职称和高学历者、在心脏急症相关科室工作者知晓率更高,但是高级别医院组的知晓率低于低级别医院组,近期(< 6月)接受CPR培训组知晓率低于长时间(> 2 a)未接受CPR培训组。84.5%的参与者认为除颤后存活是复苏成功的标准。认为判断指标持续时间大于30 s、大于20 min和大于24 h才可判定为复苏成功的参与者分别有24.9%、33.4%和18.4%。 结论 我国医护人员对乌斯坦因模式知晓率低,对“复苏成功”概念的理解混乱,需加强乌斯坦因登记模式的普及和推广。 Abstract:Objective To investigate the knowledge of the Utstein model and the criteria for evaluating the success of resuscitation among Chinese medical staffs. Method A random sampling survey was conducted among the medical staffs in Mainland of China. Results Only 58.8% of the participants had heard of the Utstein model. The awareness rate of the Utstein model was mostly related to whether the participant works in a department where registered the results of resuscitation, nurses, males, young people, senior professional titles and highly educated individuals, staff works in cardiac emergency-related department had a higher awareness rate of Utstein model. However, the awareness rate of high level hospital group was lower than that of the low level hospital group, the group who received a training within 6 months did not have a higher awareness rate than the group who had no training more than 2 years. 84.5% of participants considered that post-defibrillation survival was a standard for successful resuscitation. Additionally, 24.9%, 33.4%, and 18.4% of participants believed that judgment indicators lasted more than 30 seconds, more than 20 minutes, or more than 24 hours indicated successful resuscitation, respectively. Conclusions The awareness rate of Utsteinmodel among the medical staff is low, and the understanding of the term “success of resuscitation” is very confusing in China. It is urgent to strengthen the popularization and application of the Utstein registration model. -
Key words:
- Utstein model /
- Medical staff /
- Cardio-pulmonary resuscitation /
- Successful resuscitation
-
近年来,随着心脏骤停(cardiac arrest,CA)发生率不断上升,提高CA患者的救治成功率是急救领域亟待解决的重要问题。提高CA患者的存活率,首先必须确立一个科学统一的复苏结果评价标准。长期以来,我国的医护人员用“复苏成功率”来评价心肺复苏结果,但是这一概念的评价标准不统一,不利于对CA患者救治率和存活率做出科学客观的统计。1991年,国际上提出了院外复苏结果汇报和登记指南,即乌斯坦因模式(Utstein model),并于2004年和2005年进行两次升级简化,乌斯坦因模式的提出使全球范围内和我国部分地区的复苏登记汇报有了显著增加[1-6]。然而,国内对Utstein模式的认知更多停留在学术研究层面,实际工作中应用并不广泛。KylieDyson等[7]的研究显示,应用Utstein模式的中心之间报道的存活率差异率达到50%,说明Utstein模式的应用仍存在许多问题。中国每年约有54.4万人死于心脏骤停(cardiac arrest,CA),存活率低于1%[8]。Sasson C等[9]报道,院外心脏骤停(out-of-hospital cardiac arrest,OHCA)存活率低于10%,且不同国家报道的存活率差异很大[10-11],笔者推测,CA患者存活率报道差异大的原因,可能与由各救治中心评判标准不统一有关系。基于以上背景,为了解我国医护人员对Utstein模式的知晓情况,以及对复苏成功(Successful resuscitation)的评判标准,从而促进医务工作者使用标准的心肺复苏登记模式,特对中国大陆医护人员进行随机抽样调查,旨在为规范我国复苏结果登记和统一评价标准提供参考。
1. 资料与方法
1.1 研究对象
中国大陆31个省、市、区医护人员。
1.2 研究方法
采用抽样调查的方式,由2名院内和3名院外复苏专家、1名统计专家参照Utstein模式共同设计问卷,问卷通过“问卷星”发放,于2017年5月在进行预调查,样本量为136名,内部一致性Cronbash's α系数为0.817,重测信度为0.855。经过商议修订,于2017年11月5日至12月23日正式发布。
问卷包括两部分,第一部分为参与者的基本信息,包括8个条目,第二部分为参与者对复苏结果的认知情况,共7个条目。
1.3 质量控制
问卷匿名自愿填写,有显著提示仅供医护人员填写。系统默认参与者将所有问题填写完毕才可提交问卷,默认同一IP地址只能填写一次,避免重复答题。调查结束后对数据进行整理和逻辑检错,剔除显著逻辑错误的样本。
1.4 统计学处理
使用Excel表格对数据进行录入整理,使用SPSS23.0软件对数据进行统计分析;计数资料采用均数± 标准差(χ±SD)表示,描述性统计采用百分比[n(%)]表示,单因素分析采用χ2检验,多因素分析采用Logistic回归分析,以 P < 0.05为差异有统计学意义。
2. 结果
共收集到10 393份问卷,排除不合格问卷169份,有效样本量为10 224份,有效问卷回收率为98.37%。
2.1 调查对象基本情况
在中国大陆31个省、市、区医护人员中,参与者人数排名前五的省份为云南省(1704人)、广东省(1089人)、河北省(822人)、山东省(893人)及山西省(793人),其余省份参与调查人数在100~500人之间。调查参与者中男性占40.4%,医生占57%,20~50岁年龄段占95.3%,参与者对Utstein模式的知晓情况见表1。
表 1 参与者对Utstein模式的知晓情况[n(%)]Table 1. Participants' knowledge of Utstein model[n(%)]项目 总数 Utstein模式的知晓情况 知晓 不知晓 Z P 性别 男 4126(40.4) 2554(61.9) 1572(38.1) 5.316 < 0.001 * 女 6098(59.6) 3453(56.6) 2645(43.4) 职业 医生 5829(57.0) 3255(55.8) 2574(44.2) 6.889 < 0.001 * 护士 4395(43.0) 2752(62.6) 1643(37.4) 年龄 < 29岁 5147(50.3) 3269(63.5) 1878(36.5) < 0.001 * 30-39岁 3778(37.0) 2188(57.9) 1590(42.1) 5.417 > 40岁 1299(12.7) 550(42.3) 749(57.7) 职称 初级职称 4116(40.3) 1898(46.1) 2218(53.9) 6.897 < 0.001 * 中级职称 4033(39.4) 2624(65.0) 1412(35.0) 高级职称 2075(20.3) 1488(71.7) 587(28.3) 学历 专科及以下 2299(22.5) 1256(54.6) 1043(45.4) < 0.001 * 本科 5891(57.6) 3406(57.8) 2485(42.2) 5.972 硕士及以上 2034(19.9) 1345(66.1) 689(33.9) 医院级别 急救中心# 1046(10.2) 813(77.7) 233(22.3) < 0.001 * 一级医院 3125(30.6) 2156(69.0) 969(31.0) 6.089 二级医院 3043(29.8) 1708(56.1) 1335(43.9) 三级医院 3010(29.4) 1330(44.2) 1680(55.8) 科室 院前急救# 1052(10.3) 825(78.4) 227(21.6) < 0.001 * 急诊科 2217(21.7) 1459(65.8) 758(34.2) ICU 881(8.6) 555(63.0) 326(37.0) 麻醉科 507(5.0) 311(61.3) 196(38.7) 7.785 心脏内外科 735(7.2) 471(64.1) 264(35.9) 妇产儿科 1265(12.4) 817(64.6) 448(35.4) 其他科室 3567(34.9) 1569(44) 1998(56) 培训时间 < 6 月 4366(42.7) 2215(50.7) 2151(49.3) 6.962 < 0.001 * 6月~2a 3368(32.9) 2174(64.5) 1194(35.5) > 2a 2111(20.6) 1491(70.6) 620(29.4) 从未培训过 379(3.7) 127(33.5) 252(66.5) 科室登记复苏结果 是 7380(72.2) 5417(73.4) 1963(26.6) 7.097 < 0.001 * 否 2844(27.8) 590(20.7) 2254(79.3) *P < 0.05. #有的急救中心有住院病床,而有的急救医生为院内各科室医生轮班,导致医院和科室的数据有差别。 2.2 Utstein模式知晓率
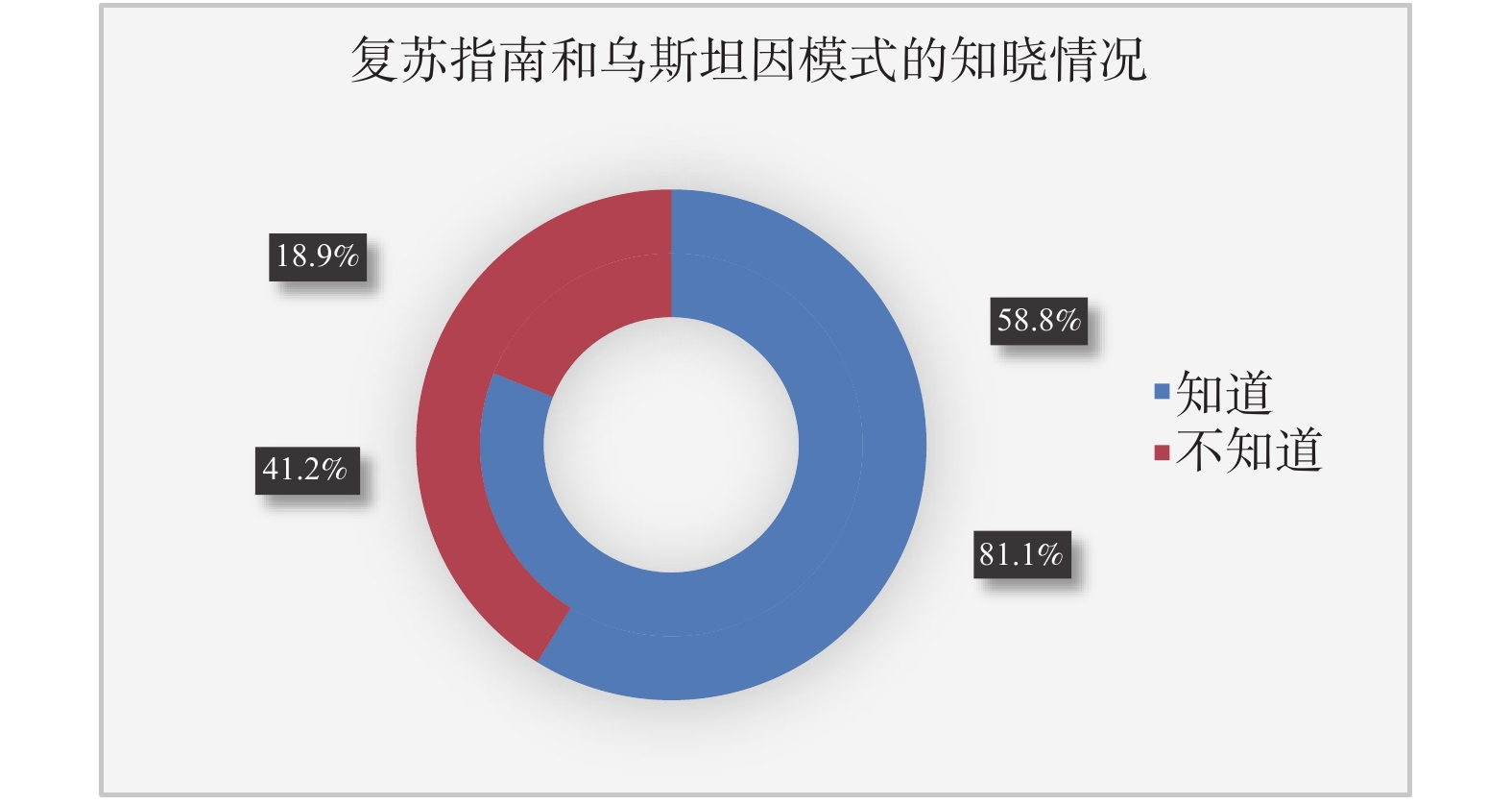
在10 224位参与者中,有6 007(58.8%)位知晓Utstein模式,8293(81.1%)位参与者听说过美国心脏协会(american heart association,AHA)的《心肺复苏和心血管急救指南》,见图1。
Logistic回归分析发现,Utstein模式知晓率医生低于护士(OR = 0.616,95% CI:0.545~0.696),男性高于女性(OR = 1.443,95% CI:1.282~1.624),年长者低于年轻者( ≥ 40岁vs < 29岁OR = 0.313,95% CI:0.265~0.369),高级职称者高于初级职称者(高级职称 vs初级职称 OR = 3.475,95% CI:2.973~4.063),高学历者高于低学历者(硕士及以上vs专科及以下 OR = 1.473,95% CI:1.242~1.747),高级别医院组低于低级别医院组(三级医院vs一级医院 OR = 0.366,95% CI:0.321~0.417),心脏急症相关科室医护人员知晓率高于其他科室医护人员(如院前急救vs其他科室 OR = 2.113,95% CI:1.717~2.601),近期接受CPR培训组低于长时间未接受CPR培训组(< 6月vs > 2a OR:0.512,95% CI:0.445~0.588),所在科室登记复苏结果组显著高于未登记复苏结果组(OR = 8.611,95% CI:7.684~9.650),见 表2。
表 2 Utstein模式知晓率的多因素Logistic回归分析Table 2. Multivariate Logistic regression analysis of Utstein model awareness rate项目 P OR 95%CI 职业 护士 1 医生 < 0.001 0.616 0.545~0.696 性别 女性 1 男性 < 0.001 1.443 1.282~1.624 年龄 < 29岁 1 30-39岁 < 0.001 0.652 0.582~0.732 > 40岁 < 0.001 0.313 0.265~0.369 职称 初级职称 1 中级职称 < 0.001 2.361 2.095~2.661 高级职称 < 0.001 3.475 2.973~4.063 学历 专科及以下 1 本科 0.429 1.052 0.927~1.194 硕士及以上 < 0.001 1.473 1.242~1.747 医院级别 一级医院 1 二级医院 < 0.001 0.539 0.473~0.613 三级医院 < 0.001 0.366 0.321~0.417 急救中心 0.802 1.027 0.834~1.264 科室 其他科室 1 院前急救 < 0.001 2.113 1.717~2.601 急诊科 < 0.001 1.424 1.244~1.630 ICU 0.015 1.258 1.045~1.515 麻醉科 0.040 1.272 1.011~1.600 心内科 < 0.001 1.498 1.229~1.827 妇产儿科 < 0.001 1.869 1.589~2.198 近期培训 > 2a 1 6月-2 a 0.108 0.889 0.769~1.026 < 6月 < 0.001 0.512 0.445~0.588 从未培训 < 0.001 0.376 0.283~0.499 科室登记复苏结果 否 1 是 < 0.001 8.611 7.684~9.650 2.3 复苏成功的标准
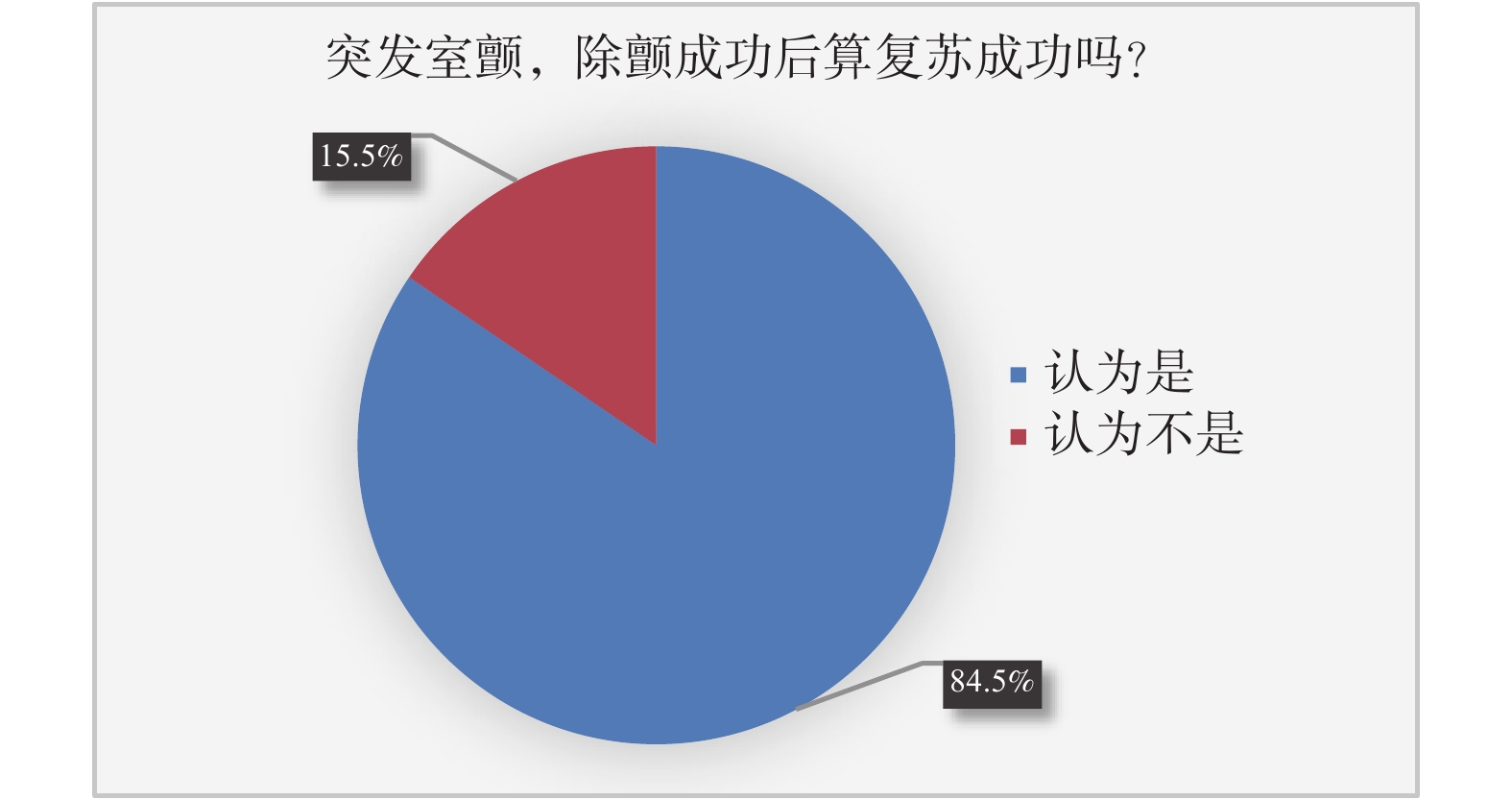
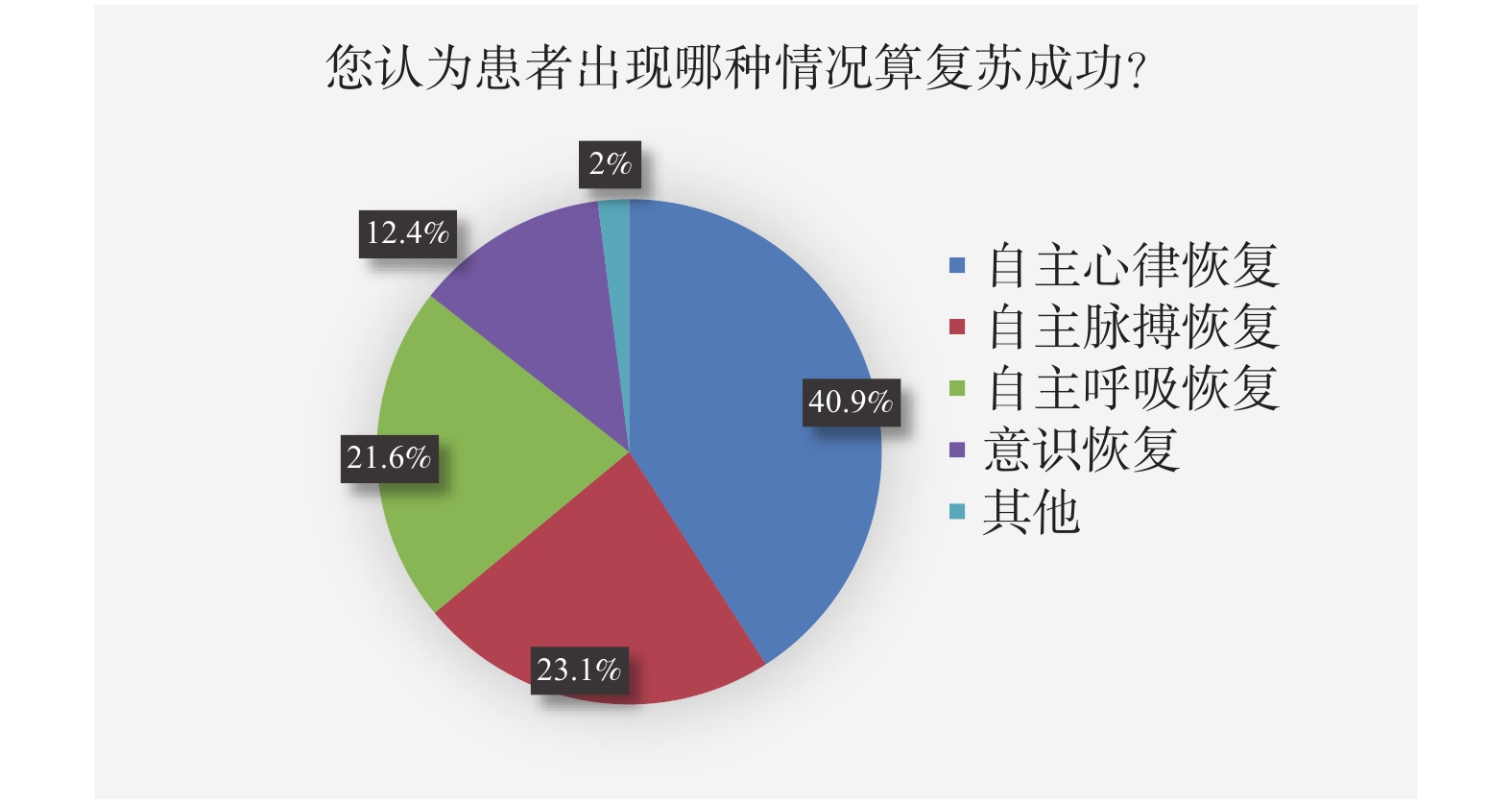
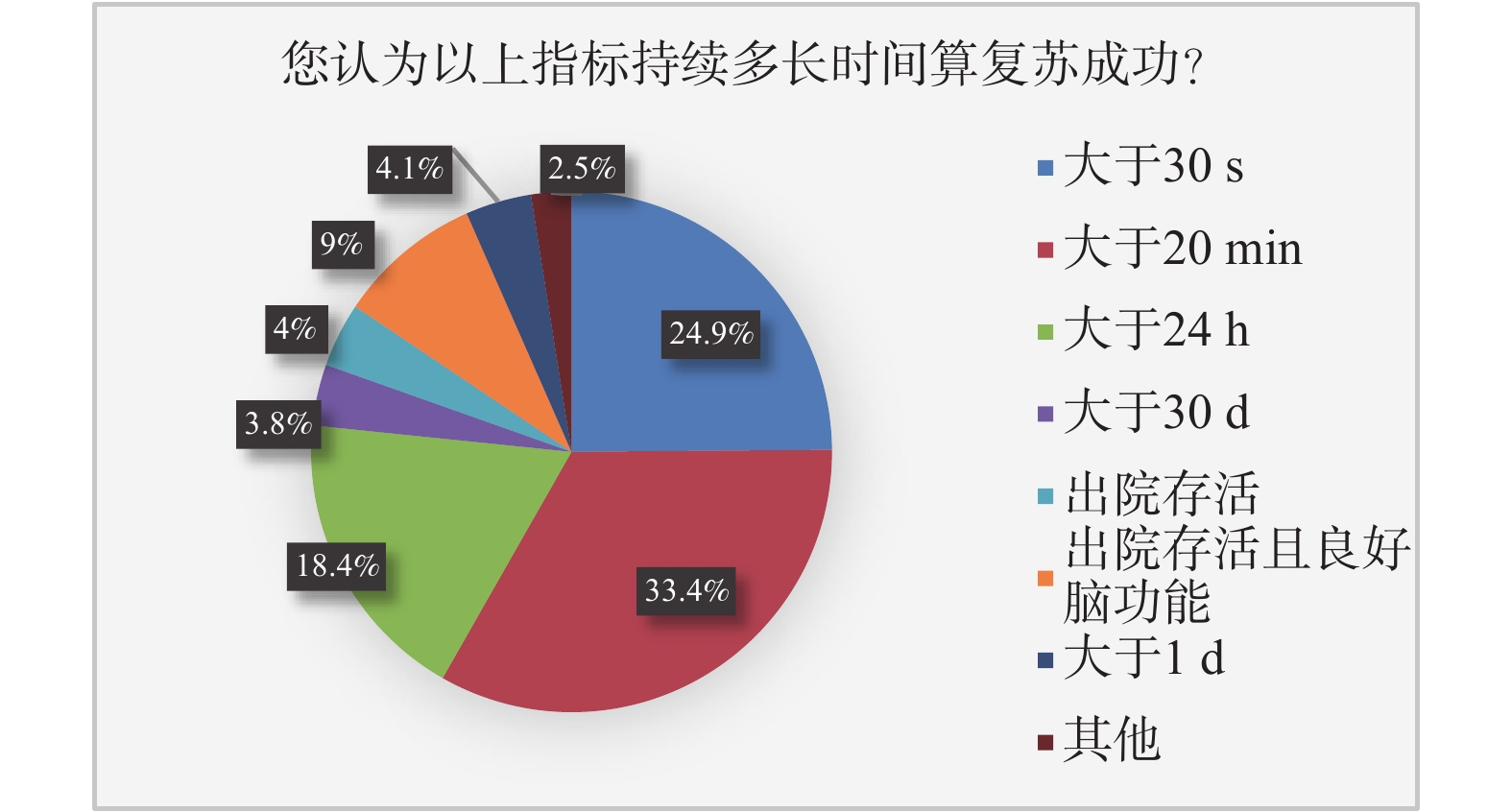
关于复苏成功判断标准调查的结果显示,突发室颤的患者除颤成功后存活,有9 638(84.5%)位参与者认为属于复苏成功,586(14.5%)位参与者认为不属于复苏成功(图2),关于复苏成功的判断标准,选择自主心律恢复、自主脉搏恢复、自主呼吸恢复和意识恢复的患者分别占40.9%(4181位)、23.1%(2357位)、21.6%(2 210位)位和12.4%(1269位)(图3)。关于持续时间,认为应当维持超过30 s、20 min、24 h和30 d的参与者依次为24.9%(2545位)、33.4%(3419位)、18.4%(1 878位)和3.8%(386位),408(4%)位参与者认为存活到出院可判断复苏成功,917(9%)位参与者认为存活到出院而且要有良好神经功能方可判断复苏成功,419(4.1%)位参与者认为存活大于1a方可判断复苏成功(图4)。
3. 讨论
Utstein模式和AHA的复苏指南被公认为两大复苏理论体系[12-13],关于医务工作者对这两大体系的知晓和践行情况鲜见研究报道,而笔者在工作中发现,部分医务工作者对这两大体系不熟悉,尤其是Utstein模式,很多年轻医务工作者更是闻所未闻。然而CA的发病率逐年提升,提高其救治率迫在眉睫,因此,笔者展开了这项调查研究,旨在了解我国医护人员对Utstein模式的知晓情况,以及对复苏成功(Successful resuscitation)的评判标准,为规范我国复苏结果登记和统一评价标准提供参考。本研究显示,虽然有超过80%的参与者听说过复苏指南,仅有约60%的参与者听说过Utstein模式,说明Utstein模式对于我国医护人员来说非常陌生。Logistic回归分析发现,Utstein模式的知晓率与所在科室是否登记复苏结果关系最大,说明大部分登记复苏结果的科室可能参考了Utstein模式[14]。年轻人和高学历者对Utstein模式的知晓率更高,可能是因为年轻人和高学历者更容易接受新知识。与心脏急症相关科室工作的医护人员对Utstein模式的知晓率更高,说明Utstein模式知晓率与CPR经验可能相关。然而,与笔者预期结果不一致的是,三级医院医护人员对Utstein模式的知晓率却低于一级医院,6个月内接受过CPR培训的人群知晓率低于大于2a没有接受过CPR培训的医护人员,可能的原因为目前大部分CPR培训的课程内容均不会纳入Utstein模式。
研究还调查了我国医护人员关于复苏结果登记的一些具体问题,包括病例纳入、判断指标和判断的时间标准。结果显示,只有84.5%的医护人员认为除颤后存活的病人属于复苏成功,事实上,室颤是CA三种类型中最常见的一种[15]。此外,CPR在Utstein模式里的定义为尝试恢复患者自主循环的方法,包括胸外按压、人工通气、除颤和药物复苏等,因此接受了电除颤,无论是否接受胸外按压,都必须纳入CPR结果登记。CPR生存链的第一环强调CA的早期识别,包括早期症状和早期心律的识别。早期症状包括抽搐和濒死样喘息,早期心律包括室颤和无脉性室速。早期识别是早期CPR和早期除颤的前提,也是CA病人存活的关键,也是决定患者能否远期存活并有良好神经功能的关键,是如今国际复苏界推崇旁观者使用体外自动除颤仪(automated external defibrillator,AED)的原因[16-18]。如果复苏结果登记时的纳入标准不包括最容易存活的室颤患者,势必会影响复苏结果的客观性。2004版Utstein模式提示自主脉搏恢复30 s即可认为复苏成功,我国医务工作者对复苏成功的判断标准高于国际标准,这可能也是我国报道的心肺复苏成功率不高的原因之一。
笔者通常用“复苏成功”来评价复苏结果,该术语在Utstein模式里对应的为“Successful resuscitation”,该名词在1991版Utstein模式中出现过两次[19],2004版出现一次,2015版则没有出现。从上世纪90年代开始,国际复苏界很少使用“复苏成功”这个术语,而将复苏结果分等级描述。1991版Utstein模式将复苏结果分为自主循环恢复(restoration of spontaneous circulation,ROSC)维持5 min以上、存活入院和存活出院三个等级[19];2004版Utstein模式推荐的核心复苏结果包括任何ROSC、存活事件、存活出院三个等级,任何ROSC的判断指标只有一个,即自主脉搏恢复[20],时间至少3 s;存活事件在院前定义为存活到医院,院内定义为存活超过20 min;存活出院是指患者从急症医院出院,无论神经功能好坏和送达地点。2015版院外Utstein模式将核心复苏结果分为近期结果和远期结果,近期结果为任何ROSC和存活事件,远期结果为出院存活或存活超过30 d[21]。
本调查研究了医护人员对“复苏成功”定义判断指标和持续时间的理解,结果显示我国医护人员对复苏成功判断指标和持续时间的理解存在很大差异,综合说来,调查结果显示的判断要求高于Utstein模式的解释,如果严格按照指南登记,真实的复苏成功率可能会高于医护人员的主观判断。当然,根据知信行理论[22],听说过调查复苏结果的浅表认知,离具体实践行为还有很大差距,我国复苏结果是否被低估还需要进一步研究证实。可以肯定的是,如果不能统一复苏结果评价的术语和标准,就很难找到心肺复苏中存在的薄弱环节,很难提高CA患者的存活率[23-24]。因此,加强对我国医护人员Utstein模式相关培训非常有必要。
综上所述,我国医护人员对Utstein模式的知晓率较低,对复苏结果的判断标准不统一,急需加强Utstein模式知识的普及和应用的推广。
-
表 1 参与者对Utstein模式的知晓情况[n(%)]
Table 1. Participants' knowledge of Utstein model[n(%)]
项目 总数 Utstein模式的知晓情况 知晓 不知晓 Z P 性别 男 4126(40.4) 2554(61.9) 1572(38.1) 5.316 < 0.001 * 女 6098(59.6) 3453(56.6) 2645(43.4) 职业 医生 5829(57.0) 3255(55.8) 2574(44.2) 6.889 < 0.001 * 护士 4395(43.0) 2752(62.6) 1643(37.4) 年龄 < 29岁 5147(50.3) 3269(63.5) 1878(36.5) < 0.001 * 30-39岁 3778(37.0) 2188(57.9) 1590(42.1) 5.417 > 40岁 1299(12.7) 550(42.3) 749(57.7) 职称 初级职称 4116(40.3) 1898(46.1) 2218(53.9) 6.897 < 0.001 * 中级职称 4033(39.4) 2624(65.0) 1412(35.0) 高级职称 2075(20.3) 1488(71.7) 587(28.3) 学历 专科及以下 2299(22.5) 1256(54.6) 1043(45.4) < 0.001 * 本科 5891(57.6) 3406(57.8) 2485(42.2) 5.972 硕士及以上 2034(19.9) 1345(66.1) 689(33.9) 医院级别 急救中心# 1046(10.2) 813(77.7) 233(22.3) < 0.001 * 一级医院 3125(30.6) 2156(69.0) 969(31.0) 6.089 二级医院 3043(29.8) 1708(56.1) 1335(43.9) 三级医院 3010(29.4) 1330(44.2) 1680(55.8) 科室 院前急救# 1052(10.3) 825(78.4) 227(21.6) < 0.001 * 急诊科 2217(21.7) 1459(65.8) 758(34.2) ICU 881(8.6) 555(63.0) 326(37.0) 麻醉科 507(5.0) 311(61.3) 196(38.7) 7.785 心脏内外科 735(7.2) 471(64.1) 264(35.9) 妇产儿科 1265(12.4) 817(64.6) 448(35.4) 其他科室 3567(34.9) 1569(44) 1998(56) 培训时间 < 6 月 4366(42.7) 2215(50.7) 2151(49.3) 6.962 < 0.001 * 6月~2a 3368(32.9) 2174(64.5) 1194(35.5) > 2a 2111(20.6) 1491(70.6) 620(29.4) 从未培训过 379(3.7) 127(33.5) 252(66.5) 科室登记复苏结果 是 7380(72.2) 5417(73.4) 1963(26.6) 7.097 < 0.001 * 否 2844(27.8) 590(20.7) 2254(79.3) *P < 0.05. #有的急救中心有住院病床,而有的急救医生为院内各科室医生轮班,导致医院和科室的数据有差别。  下载: 导出CSV
下载: 导出CSV
表 2 Utstein模式知晓率的多因素Logistic回归分析
Table 2. Multivariate Logistic regression analysis of Utstein model awareness rate
项目 P OR 95%CI 职业 护士 1 医生 < 0.001 0.616 0.545~0.696 性别 女性 1 男性 < 0.001 1.443 1.282~1.624 年龄 < 29岁 1 30-39岁 < 0.001 0.652 0.582~0.732 > 40岁 < 0.001 0.313 0.265~0.369 职称 初级职称 1 中级职称 < 0.001 2.361 2.095~2.661 高级职称 < 0.001 3.475 2.973~4.063 学历 专科及以下 1 本科 0.429 1.052 0.927~1.194 硕士及以上 < 0.001 1.473 1.242~1.747 医院级别 一级医院 1 二级医院 < 0.001 0.539 0.473~0.613 三级医院 < 0.001 0.366 0.321~0.417 急救中心 0.802 1.027 0.834~1.264 科室 其他科室 1 院前急救 < 0.001 2.113 1.717~2.601 急诊科 < 0.001 1.424 1.244~1.630 ICU 0.015 1.258 1.045~1.515 麻醉科 0.040 1.272 1.011~1.600 心内科 < 0.001 1.498 1.229~1.827 妇产儿科 < 0.001 1.869 1.589~2.198 近期培训 > 2a 1 6月-2 a 0.108 0.889 0.769~1.026 < 6月 < 0.001 0.512 0.445~0.588 从未培训 < 0.001 0.376 0.283~0.499 科室登记复苏结果 否 1 是 < 0.001 8.611 7.684~9.650
下载: 导出CSV
-
[1] Nehme Z, Andrew E, Bernard S, et al. The impact of partial resuscitation attempts on the reported outcomes of out-of-hospital cardiac arrest in Victoria, Australia: Implications for Utstein-style outcome reports[J]. Resuscitation, 2014, 85(9): 1185-1191. doi: 10.1016/j.resuscitation.2014.05.032 [2] Iwamura T, Sakamoto Y, Kutsukata N, et al. An Utstein-style Examination of Out-of-hospital Cardiac Arrest Patients in Saga Prefecture, Japan[J]. Journal of Nippon Medical School, 2013, 80(3): 184-191. doi: 10.1272/jnms.80.184 [3] Poppe M, Weiser C, Holzer M, et al. The incidence of “load&go” out-of-hospital cardiacarrest candidates for emergency department utilization of emergency extracorporeal life support: A one-year review[J]. Resuscitation, 2015, 91(8): 131-136. [4] Shao F, Li CS, Liang LR, et al. Incidence and outcome of adult in-hospital cardiac arrest in Beijing, China[J]. Resuscitation, 2016, 102(1): 51-56. [5] Shao F, Li CS, Liang LR, et al.Outcome of out-of-hospital cardiac arrests in Beijing, China[J]. Resuscitation, 2014, 85(11): 1411-1417. doi: 10.1016/j.resuscitation.2014.08.008 [6] Song W, Chen S, Liu YS, et al. A prospective investigation into the epidemiology of in-hospital cardiopulmonary resuscitation using the international Utstein reporting style[J]. HONG KONG JOURNAL OF EMERGENCY MEDICINE, 2011, 18(6): 391-396. doi: 10.1177/102490791101800604 [7] Dyson Kylie, Brown Siobhan P, May Susanne, et al. International variation in survival after out-of-hospital cardiac arrest: A validation study of the Utstein template[J].Resuscitation, 2019, 138(1): 168-181. [8] 王立祥, 孟庆义, 余涛. 2016中国心肺复苏专家共识[J]. 中华灾害救援医学, 2017, 5(01): 8-30. [9] Sasson Comilla, Rogers Mary A M, Dahl Jason, et al. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis[J].Circ Cardiovasc Qual Outcomes, 2010, 3(1): 63-81. doi: 10.1161/CIRCOUTCOMES.109.889576 [10] Okubo Masashi, Gibo Koichiro, Wallace David J, et al. Regional variation in functional outcome after out-of-hospital cardiac arrest across 47 prefectures in Japan[J].Resuscitation, 2018, 124(1): 21-28. [11] Berdowski Jocelyn, Berg Robert A, Tijssen Jan G, P et al. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies[J].Resuscitation, 2010, 81(11): 1479-87. doi: 10.1016/j.resuscitation.2010.08.006 [12] 王微, 宋维, 陈文腾, 等.基于Utstein模式下的院内心脏骤停原因评价[J].中国急救医学. 2015, 35(1): 24-28. doi: 10.3969/j.issn.1002-1949.2015.01.006 [13] 宋维, 陈实, 刘元税, 等.基于乌斯坦因模式的心肺复苏研究报告[J].中华急诊医学杂志, 2012, 21(9): 1003-1006. doi: 10.3760/cma.j.issn.1671-0282.2012.09.020 [14] 朱虹, 刘俊鹏, 许波, 等. 深圳市院外心脏骤停发生地点特征分析[J]. 岭南急诊医学杂志, 2019, 24(6): 521-523. doi: 10.3969/j.issn.1671-301X.2019.06.003 [15] Hazinski MF, Nolan JP, Aickin R, et al. Part 1: Executive Summary: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations[J].Circulation, 2015; 132(16): S2-39. [16] Weiser C, Poppe M, Sterz F, et al. Initial electrical frequency predicts survival and neurological outcome in out of hospital cardiac arrest patients with pulseless electrical activity[J]. Resuscitation, 2018, 125(1): 34-38. [17] Salam I, Thomsen JH, Kjaergaard J, et al. Importance of comorbidities in comatose survivors of shockable and non-shockable out-of-hospital cardiac arrest treated with target temperature management[J]. Scand Cardiovasc J, 2018, 52(3): 133-140. doi: 10.1080/14017431.2018.1450991 [18] Zijlstra JA, Bekkers LE, Hulleman M, et al. Automated external defibrillator and operator performance in out-of-hospital cardiac arrest[J]. Resuscitation, 2017, 118(1): 140-146. [19] Cummins RO, Chamberlain DA, Abramson NS, et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: the Utstein Style: A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council[J]. Circulation, 1991, 84(2): 960-975. doi: 10.1161/01.CIR.84.2.960 [20] Jacobs I, Nadkarni V, Bahr J, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation [J]. Circulation. 2004, 110(21): 3385-3397. doi: 10.1161/01.CIR.0000147236.85306.15 [21] Perkins, Gavin D, Jacobs, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein resuscitation registry templates for out-of-hospital cardiac arrest, a statement for healthcare professionals from a task force of the international liaison committee on resuscitation; and the American heart association emergency cardiovascular care committee and the council on cardiopulmonary, critical care, perioperative and resuscitation[J]. Resuscitation, 2015, 96(1): 328-340. [22] 费素定, 胡苏珍, 金晓霞, 等. 宁波市农村居民院前急救知识、态度与行为现状的研究[J].中华护理杂志, 2014, 49(3): 275-279. doi: 10.3761/j.issn.0254-1769.2014.03.004 [23] Maurer H, Masterson S, Tjelmeland IB, et al. When is a bystander not a bystander any more? An European Survey[J]. Resuscitation, 2019, 136(1): 78-84. [24] Sunde GA, Kottmann A, Heltne JK, et al.Standardized data reporting from pre-hospital advanced airway management—a nominal group technique update of the Utstein-style airway template[J].Scand J Trauma Resusc Emerg Med, 2018, 26(1): 46-72. doi: 10.1186/s13049-018-0509-y 期刊类型引用(1)
1. 王新锋. 去甲肾上腺素联合碳酸氢钠治疗心脏骤停复苏后低血压的效果. 中国当代医药. 2022(34): 80-83 .  百度学术
百度学术其他类型引用(0)
-

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 2097
- HTML全文浏览量: 1683
- PDF下载量: 8
- 被引次数: 1
