

Expressions of ROR1 in Lung Adenocarcinoma and Its Relationship with Spread Through Air Apace
-
摘要:
目的 研究受体酪氨酸激酶样孤儿受体1(receptor tyrosine kinase-like orphan rectetpor 1,ROR1)在不同病理亚型肺腺癌组织中的表达与气腔播散(spread through air space,STAS)发生的关系。 方法 收集昆明医科大学第一附属医院病理科2017年6月至2022年1月,肺腺癌组织蜡块标本618例,采用HE染色切片判断病理亚型与病理特征,记数STAS数量并分级,免疫组化染色,半定量判读ROR1表达水平,统计分析ROR1表达与STAS数量及与病理亚型的关系。 结果 ROR1在微乳头型与实体型肺腺癌(低分化)中的表达高于其它亚型肺腺癌,差异有统计学意义(P < 0.001);ROR1在低STAS、高STAS组中表达率分别为88.0%、94.1%,高于无STAS组且差异有统计学意义(P < 0.001)。 结论 ROR1高表达于低分化肺腺癌并提示更高的STAS发生率。ROR1有望成为新的肺腺癌诊断生物标志物用于指导临床治疗及辅助预后判断,并可能成为STAS阳性肺腺癌的潜在治疗靶点。 Abstract:Objective To study the relationship between the expression of receptor tyrosine kinase-like orphan receptor 1 (ROR1) and spread through air space (STAS) in lung adenocarcinoma tissues. Methods We collected 618 cases of lung adenocarcinoma from June 2017 to January 2, 2022, HE staining section was used to determine pathological subtypes and pathological characteristics, count STAS number and grade. The expression of ROR1 was detected by immunohistochemistry staining in different pathological subtypes of lung adenocarcinoma and the relationship with STAS quantity was analyzed. Results ROR1 expressions were higher in micropapillary and solid lung adenocarcinoma (poorly differentiated) (P < 0.001); ROR1 expression rates were 88.0%, 94.1% in low STAS and high STAS groups, significantly higher than no STAS group (P < 0.001). Conclusions ROR1 is highly expressed in poorly differentiated lung adenocarcinoma and suggests a higher incidence of STAS. ROR1 is expected to be a new diagnostic biomarker of lung adenocarcinoma for guiding clinical treatment and assisting prognostic judgment, and may be a potential therapeutic target for STAS-positive lung adenocarcinoma. -
Key words:
- Lung adenocarcinoma /
- ROR1 /
- Spread through air space /
- Pathological subtypes /
- Immunohistochemistry
-
肺腺癌是世界范围最常见的恶性肿瘤之一,近年来在我国发病率有上升趋势,虽然靶向治疗等新型治疗模式取得长足发展,肺腺癌的疗效得到了显著提高,但肺腺癌仍是病死率最高的恶性肿瘤之一[1]。肺腺癌的侵袭、转移是导致患者生存率低的最主要因素[2],传统肺腺癌的侵袭转移途径包括:血管、淋巴管侵犯及胸膜侵犯[3]。在《WHO(2015)肺肿瘤病理诊断指南》中正式提出并命名了一种新的肺癌侵袭模式:气腔播散或气道播散(spread through air space,STAS),定义为呈微乳头状、簇状、实性的肿瘤巢或单个散在肿瘤细胞脱离主瘤体进入周围肺泡腔中播散,最终形成癌岛及卫星癌灶,导致肿瘤进展[4]。到目前为止,还没有任何被广泛接受的理论来解释STAS的发生、发展机制,但现有研究已经证实STAS是导致肺腺癌患者术后复发、进展的独立高危因素[5]。
受体酪氨酸激酶样孤儿受体(receptor tyrosine kinase-like orphan rectetpor 1,ROR1)是一类膜受体,属于Ⅰ型受体酪氨酸激酶(receptor tyrosine kinase,RTK)家族,主要包括ROR1和ROR2,其中ROR1主要通过参与细胞内与细胞间信号传导,实现调节细胞代谢、增殖、凋亡、分化、迁移、转移等功能[6-8]。近年来国内外研究发现,ROR1在正常、分化成熟的组织中几乎不表达,但在包括乳腺癌、结直肠癌、卵巢癌、恶性黑色素瘤、淋巴造血系统肿瘤等多种肿瘤中高表达[9-13],而且表达水平与肿瘤恶性程度、侵袭性及转移等生物学行为存在密切关系[6]。
目前针对STAS的研究主要集中在肺腺癌的临床病理特征及预后影响等方面,研究对象主要为肺叶或亚肺叶(肺段)切除术后的肿瘤标本。由于STAS仅能在术后才能确诊,术前或术中冰冻判断STAS较为困难[14]。本文结合肺腺癌的病理组织亚型,通过检测ROR1蛋白在肺腺癌中的表达水平,探讨ROR1作为STAS发生预测指标的价值,初步探讨其潜在机制,为临床在术前辅助判断肺腺癌STAS状态,进一步制定针对性治疗方案提供参考。
1. 材料与方法
1.1 临床资料
收集昆明医科大学第一附属医院病理科2017年6月至2022年1月手术切除肺腺癌蜡块标本618例,其中男性242例(39.2%),女性376例(60.8%),年龄29~81岁,中位年龄59岁。原位癌、微浸润性腺癌及术前接受放、化疗者均排除。本研究通过昆明医科大学第一附属医院医学伦理审核委员会审核。通过复习病理切片,按WHO肺肿瘤病理诊断指南[4]标准以主要肿瘤病理亚型,将肺腺癌分为高分化(贴壁型),中分化(腺泡型、乳头型),低分化(微乳头型、实体型),同时观察肿瘤神经侵犯、脉管侵犯、胸膜侵犯情况,由2位经验丰富的病理医生观察是否存在STAS,记录STAS肿瘤细胞数目、形态、分布,见图1。
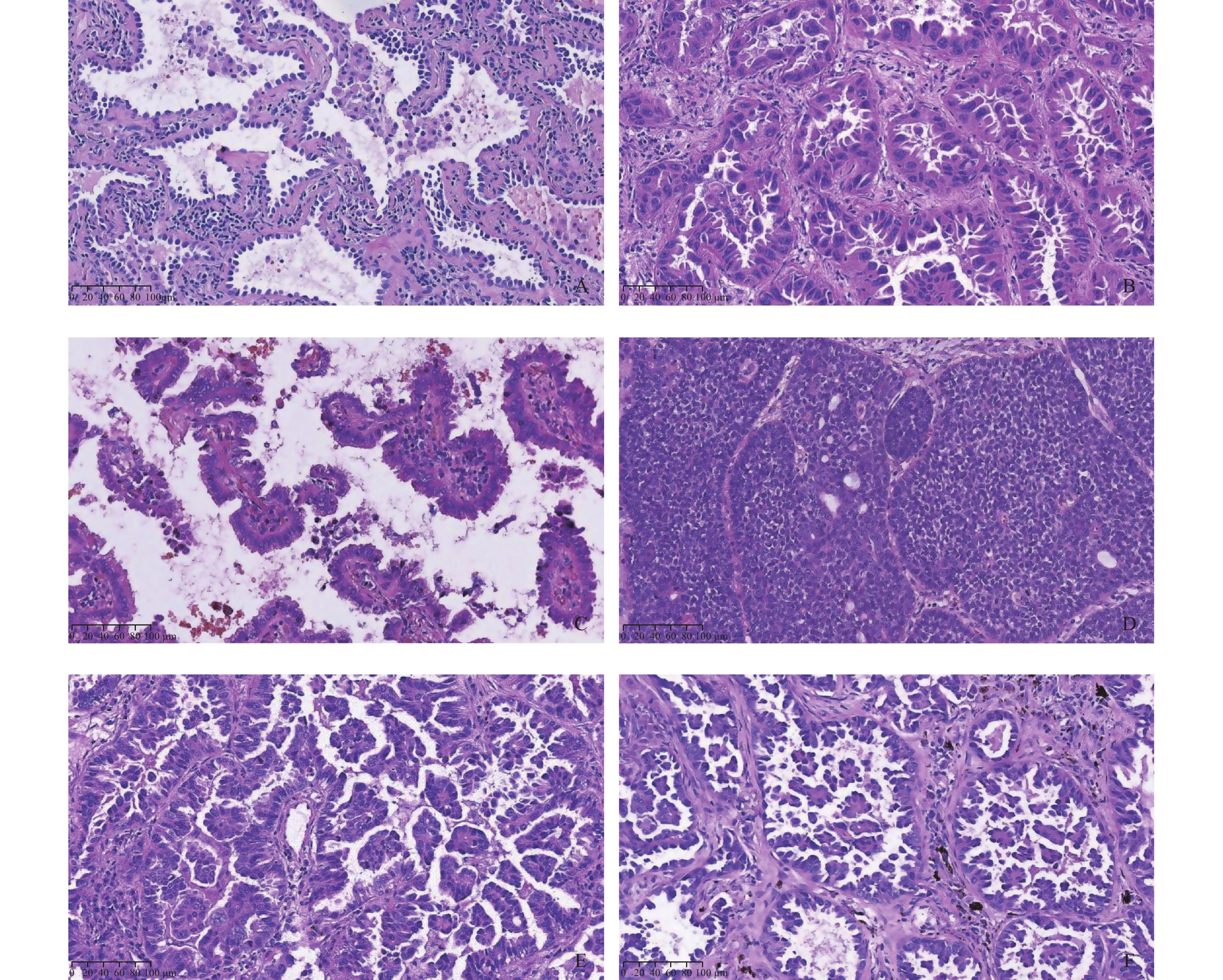 图 1 肺腺癌病理学亚型A:附壁型(高分化,HE×100);B:腺泡型(中分化,HE×200);C:乳头型(中分化,HE×200); D:实体型(低分化,HE×100);E:微乳头型(低分化,HE×200);F:腺泡型伴有微乳头结构(低分化,HE×200)。Figure 1. Subtypes of lung adenocarcinoma
图 1 肺腺癌病理学亚型A:附壁型(高分化,HE×100);B:腺泡型(中分化,HE×200);C:乳头型(中分化,HE×200); D:实体型(低分化,HE×100);E:微乳头型(低分化,HE×200);F:腺泡型伴有微乳头结构(低分化,HE×200)。Figure 1. Subtypes of lung adenocarcinoma1.2 实验方法
实验标本均经中性福尔马林固定,采用石蜡包埋,切片后,行HE及EnVision两步法免疫组化染色(IHC)。ROR1蛋白抗体购自美国Thermo Fisher公司;二抗购自迈新生物技术公司;阴性对照采用PBS代替一抗。
1.3 结果判断
1.3.1 STAS判断与分组
依据WHO定义判断是否发生STAS,记录STAS类型及细胞数量,按照病理学形态分为3类[4, 15]:(1)肿瘤周围肺泡腔内见呈微乳头或簇状肿瘤细胞巢;(2)肿瘤周围肺泡腔内见实性小巢状肿瘤细胞或肿瘤岛;(3)肿瘤周围肺泡腔内见散在单个肿瘤细胞;根据STAS肿瘤细胞数量进一步分组[16-17]为:无STAS组(未观察到STAS)、低STAS组(STAS肿瘤细胞数量为1~4个)、高STAS组(STAS肿瘤细胞数量≥5个),见图2。
 图 2 STAS病理形态与分组A:低倍镜下显示单个或散在小巢肿瘤细胞脱离肿瘤主体播散进入邻近肺泡腔内(HE×40);B:STAS肿瘤细胞呈单个、簇状、微乳头状结构(HE×200);C:低STAS组(单个、散在肿瘤细胞,HE×400);D:高STAS组(HE×200)。Figure 2. Pathological morphology and grouping of STAS
图 2 STAS病理形态与分组A:低倍镜下显示单个或散在小巢肿瘤细胞脱离肿瘤主体播散进入邻近肺泡腔内(HE×40);B:STAS肿瘤细胞呈单个、簇状、微乳头状结构(HE×200);C:低STAS组(单个、散在肿瘤细胞,HE×400);D:高STAS组(HE×200)。Figure 2. Pathological morphology and grouping of STAS1.3.2 免疫组化结果判断
ROR1蛋白免疫组化染色着色定位于肿瘤细胞质与细胞膜(染色强度判断需对比背景非特异着色),根据阳性染色强度与阳性细胞比例采用半定量积分法[11]判定结果:(1)染色强度以多数细胞呈现的染色特性计分:无着色为0分,光镜可识别的黄色(弱阳性)为1分,棕黄色(中阳性)为2分,棕褐色(强阳性)为3分;(2)计算阳性肿瘤细胞百分率并评分:0~5%为0分,6%~25%为1分,26%~50%为2分,51%~75%为3分,75%为4分。两项得分相乘,得分≥4分,判断为阳性; < 4分判断为阴性,见图3。
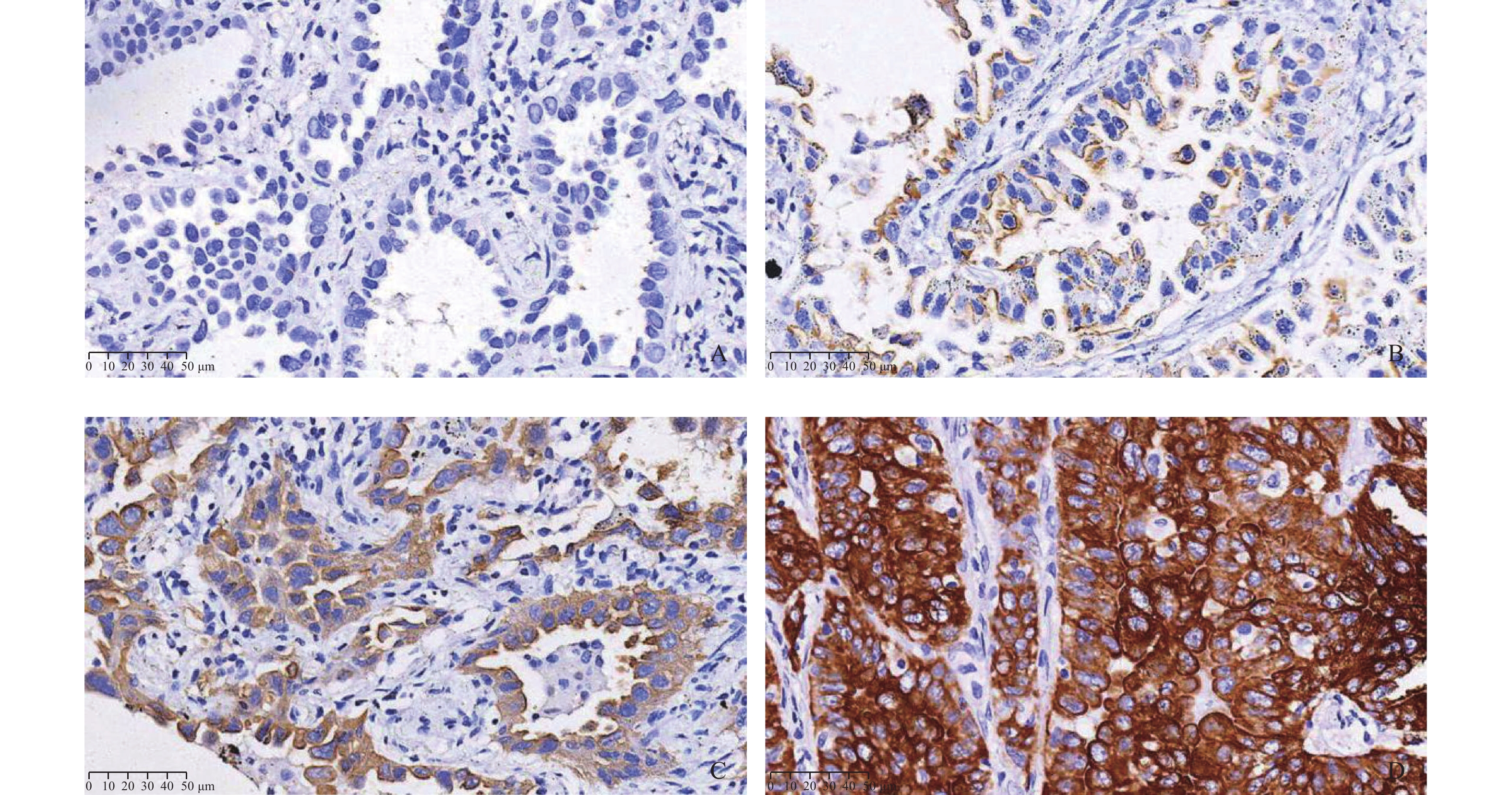 图 3 ROR1在肺腺癌中的表达 (IHC ×400)A:阴性;B:弱阳性 ;C:中阳性 ;D:强阳性。Figure 3. Expression of ROR1 in lung adenocarcinoma(IHC ×400)
图 3 ROR1在肺腺癌中的表达 (IHC ×400)A:阴性;B:弱阳性 ;C:中阳性 ;D:强阳性。Figure 3. Expression of ROR1 in lung adenocarcinoma(IHC ×400)1.4 统计学处理
应用SPSS21.0统计软件,采用χ2检验分析,表1中组织学形态与STAS关系 、表2、表3均采用列联表分析,计算Pearson卡方值。表1中除上述表格外的其他表均采用一般四格表卡方检验计算Pearson卡方值,再比较P值。采用χ2检验分析比较ROR1在不同肺腺癌病理亚型的表达水平,并分析ROR1在不同STAS分组中表达的差异。以P < 0.05为差异有统计学意义。
表 1 STAS与肺腺癌临床病理学特征的关系 [n(%)]Table 1. Relationship between STAS and clinicopathological features of lung adenocarcinoma[n(%)]临床病理学参数 n STAS χ2 P + − 性别 1.305 0.253 男 242 82(33.9) 160(66.1) 女 376 111(29.5) 265(70.5) 年龄(岁) 3.388 0.066 < 65 280 98(35.0) 182(65.0) ≥65 338 95(28.1) 243(71.9) 吸烟史 25.262 < 0.001* 无 431 108(25.1) 323(74.9) 有 187 85(45.5) 102(54.5) 肿瘤直径(cm) 191.946 < 0.001* ≤2.5 442 66(14.9) 376(85.1) > 2.5 176 127(72.2) 49(27.8) 组织学形态 123.404 < 0.001* 贴壁型 95 0(0.0) 95(100.0) 腺泡型 255 68(26.7) 187(73.3) 乳头型 148 43(29.1) 105(70.9) 微乳头型 69 49(71.0) 20(29.0) 实体型 51 33(64.7) 18(35.3) 淋巴结转移 139.614 < 0.001* 无 529 108(20.4) 421(79.6) 有 89 73(82.0) 16(18.0) 神经侵犯 30.739 < 0.001* 无 595 169(28.4) 426(71.6) 有 23 19(82.6) 4(17.4) 脉管侵犯 145.165 < 0.001* 无 517 124(24.0) 393(76.0) 有 101 87(86.1) 14(13.9) 胸膜侵犯 225.090 < 0.001* 无 443 83(18.7) 360(81.3) 有 175 146(83.4) 29(16.6) *P < 0.05。 表 2 ROR1在不同亚型肺腺癌中的表达 [n(%)]Table 2. Expression of ROR1 in different subtypes of lung adenocarcinoma[n(%)]肺腺癌病理亚型 n ROR1 χ2 P + − 贴壁型(高分化) 95 9(9.5) 86(90.5) 腺泡型(中分化) 255 73(28.6) 182(71.4) 乳头型(中分化) 148 49(33.1) 99(66.9) 135.093 < 0.001* 微乳头型(低分化) 69 55(79.7) 14(20.3) 实体型(低分化) 51 41(80.4) 10(19.6) *P < 0.05。 表 3 ROR1在不同STAS分组中的表达 [n(%)]Table 3. ROR1 expression in different STAS groups[n(%)]STAS分组 n ROR1 χ2 P + − 无STAS组 425 45(10.6) 380(89.4) 低STAS组 109 96(88.0) 13(12.0) 372.047 < 0.001* 高STAS组 84 79(94.1) 5(5.9) *P < 0.05。 2. 结果
2.1 STAS与肺腺癌亚型及临床病理特征的关系
肺腺癌618例,STAS阳性率为31.2%(193/618),通过分析发现STAS的发生与患者性别、年龄无关(P > 0.05);有吸烟史的患者具有更高的STAS发生率(P < 0.001);肿瘤直径 > 2.5 cm组肺腺癌STAS发生率为72.2%高于直径≤2.5 cm组(P < 0.001);进一步分析各亚型肺腺癌的STAS阳性率发现:低分化肺腺癌(微乳头型、实体型肺腺癌,STAS阳性率分别为71.0%、64.7%),高于中分化肺腺癌(腺泡型、乳头型,STAS阳性率分别为26.7%、29.1%),高分化的贴壁型肺腺癌中未发现STAS现象(P < 0.001)。通过分析临床病理特征与STAS发生的相关性发现,STAS的发生与其它肺腺癌侵袭性生物学行为如:淋巴结转移、神经侵犯、脉管侵犯及胸膜侵犯相关(P < 0.001),见表1。
2.2 ROR1在不同亚型肺腺癌中的表达
采用免疫组化法检测618例肺腺癌ROR1表达情况,通过观察阳性率发现:贴壁型(9.5%)低于腺泡型与乳头型(分别为28.6%、33.1%),而微乳头型与实体型肺腺癌(分别为79.7%、80.4%)ROR1表达率高于其余各亚型肺腺癌,见表2、图4。
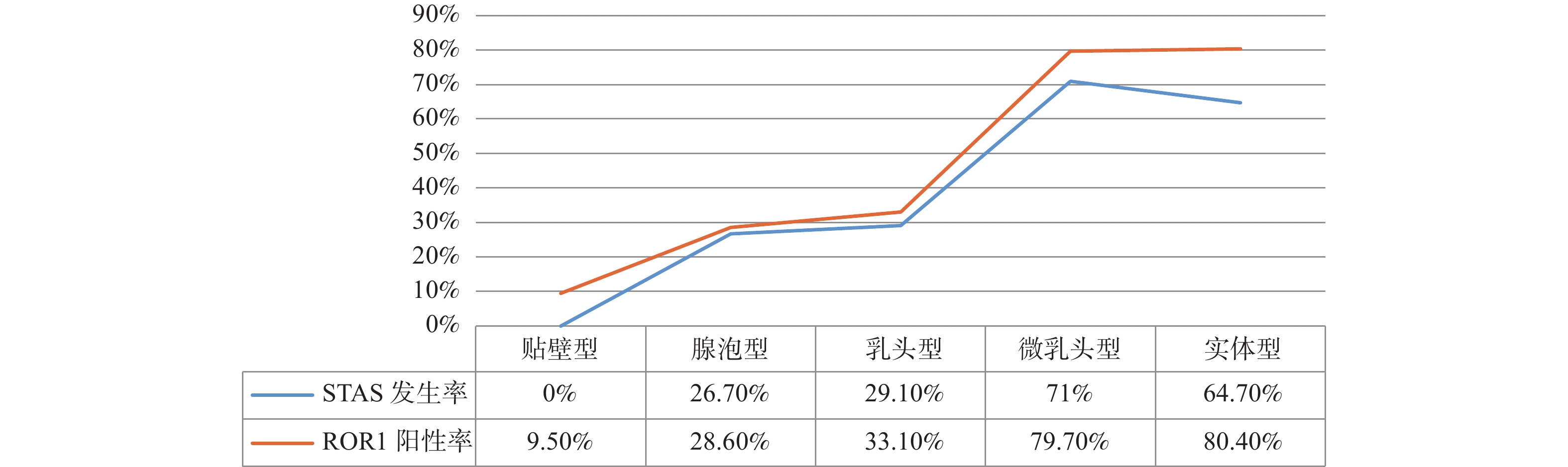 图 4 不同病理亚型肺腺癌STAS发生率与ROR1表达率的关系Figure 4. The relationship between the incidence of STAS and ROR1 expression in different pathological subtypes of lung adenocarcinoma
图 4 不同病理亚型肺腺癌STAS发生率与ROR1表达率的关系Figure 4. The relationship between the incidence of STAS and ROR1 expression in different pathological subtypes of lung adenocarcinoma2.3 ROR1在不同STAS分组中的表达
通过比较无STAS组(未观察到STAS,425例,68.8%),低STAS组(STAS数量为1~4个,109例,17.6%),高STAS组(STAS数量≥5个, 84例,13.6%),3组ROR1表达率分别为10.6%、88.0%、94.1%,见表3、图5;且低、高STAS组中STAS肿瘤细胞与主瘤体ROR1表达强度基本一致,见图6。
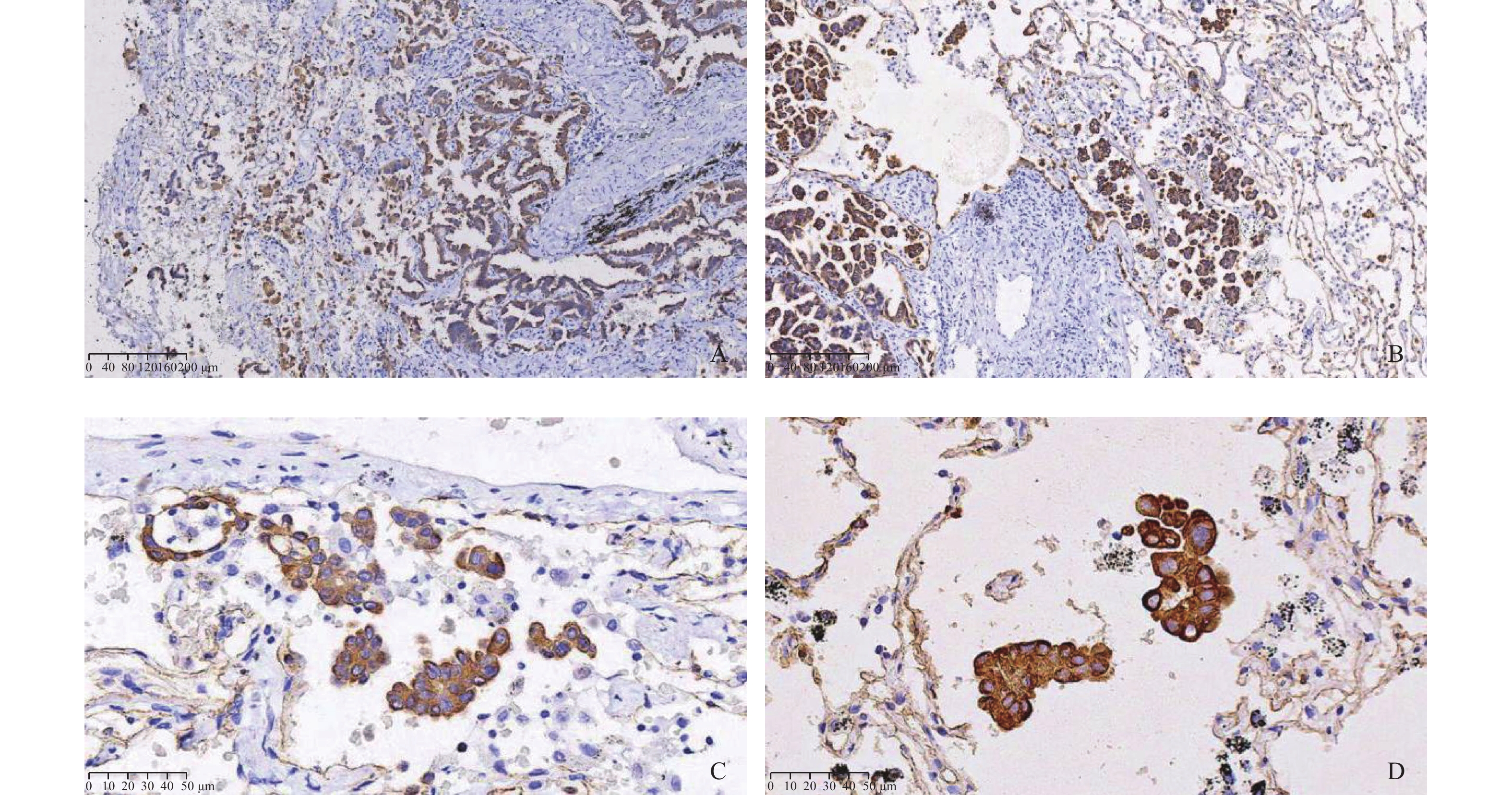 图 6 ROR1在STAS阳性肺腺癌中的表达A、B:ROR1在高STAS组肿瘤中过表达(IHC×100);C、D: STAS肿瘤细胞ROR1呈强阳性表达(IHC×400)。Figure 6. ROR1 expression in STAS positive lung adenocarcinoma
图 6 ROR1在STAS阳性肺腺癌中的表达A、B:ROR1在高STAS组肿瘤中过表达(IHC×100);C、D: STAS肿瘤细胞ROR1呈强阳性表达(IHC×400)。Figure 6. ROR1 expression in STAS positive lung adenocarcinoma3. 讨论
本研究结果显示在618例肺腺癌中STAS阳性率为31.2%,有吸烟史、肿瘤直径 > 2.5 cm的肺腺癌具有更高的STAS阳性率,与国内外文献报道接近[18],其中低分化的微乳头型与实体型肺腺癌STAS阳性率分别为71.0%、64.7%,高于中分化肺腺癌(腺泡型、乳头型,STAS阳性率分别为26.7%、29.1%);而在贴壁型肺腺癌中未发现STAS。这一结果提示,STAS的发生主要取决于肿瘤的分化程度,并且与神经侵犯、脉管侵犯、胸膜侵犯一样提示肿瘤具有更高的侵袭性生物学行为。
通过比较不同亚型肺腺癌ROR1的表达水平后发现,ROR1在微乳头型与实体型肺腺癌(分别为79.7%、80.4%)中的表达高于其余各组织学类型组,这一结果显示,ROR1高表达于低分化肺腺癌;依据STAS状态进一步分组后发现低STAS组、高STAS组的ROR1表达率分别为88.0%、94.1%,高于无STAS组(10.6%),说明ROR1高表达于STAS阳性肺腺癌。
总结本研究结果,ROR1高表达于低分化、高侵袭性的肺腺癌,并提示高STAS发生率。因此推测ROR1在肺腺癌组织中的高表达可能与肺腺癌的发生发展以及STAS的发生存在密切关系,但病理生理学过程尚不明确。依据现有相关文献报道,其潜在机制可能主要有以下几方面:(1)ROR1过表达诱导肺腺癌细胞EMT,从而促进STAS发生[19-20]。EMT(上皮-间质转化)是指上皮细胞通过程序转化为表现出间质细胞特征的病理生理学过程。通过EMT,肿瘤细胞极性丧失,粘附性下降,同时具有促进肿瘤细胞的迁移、侵袭、抗凋亡和降解细胞外基质的能力[21]。虽然STAS是肺癌特有的一种浸润生长模式,但在本研究中发现STAS的发生与淋巴结转移、神经侵犯、脉管侵犯及胸膜侵犯肿瘤侵袭性生物学行为相关,这些侵袭性生长现象均是在肿瘤粘附性下降、迁移能力增强的前提下发生的。目前,在结肠癌、乳腺癌的研究中已经发现ROR1高表达具有促进肿瘤细胞EMT作用[13, 22],因此推测,ROR1高表达的肺腺癌发生EMT导致肿瘤细胞粘附性下降,脱离主瘤体播散进入到周围肺泡腔内,这可能是发生STAS的直接原因与关键启动步骤;(2)ROR1高表达促进肺腺癌细胞高增殖、高侵袭性,导致STAS发生。本研究发现ROR1高表达于分化程度低,侵袭、转移能力强的肺腺癌亚型中,在国内外研究中也发现ROR1高表达于分化差的结肠癌、宫颈癌、乳腺癌等肿瘤中并具有促肿瘤增殖、侵袭的作用[23-24],在一项结肠癌研究中发现通过下调ROR1表达能够降低肿瘤细胞增殖与迁移能力[22]。因此,ROR1过表达可能促进肺腺癌细胞的高增殖、高侵袭性,这也是导致STAS发生的重要因素。
自从2015年STAS被WHO列为肺癌浸润标准以来,引起临床病理学的高度关注[25-27]。但到目前为止,还没有被广泛接受的理论来解释STAS发生、发展机制。通过本研究发现,ROR1高表达的肺腺癌具有较高的STAS阳性率,提示肿瘤差分化及高侵袭性。因此ROR1有望成为临床肺腺癌诊断的重要生物学标志物,特别是通过在肺癌术前检测ROR1表达水平,可以辅助判断肿瘤恶性程度,并预测肺腺癌STAS发生概率,为临床针对患者制定个体化的手术方式与术后治疗方案提供参考依据,从而改善患者预后。ROR1在STAS阳性肺腺癌过表达现象,其病理生理学机制还有待进一步深入研究;但这一发现,也为将来以ROR1为靶点治疗STAS阳性肺癌提供了新的研究方向。
-
图 1 肺腺癌病理学亚型
A:附壁型(高分化,HE×100);B:腺泡型(中分化,HE×200);C:乳头型(中分化,HE×200); D:实体型(低分化,HE×100);E:微乳头型(低分化,HE×200);F:腺泡型伴有微乳头结构(低分化,HE×200)。
Figure 1. Subtypes of lung adenocarcinoma
图 2 STAS病理形态与分组
A:低倍镜下显示单个或散在小巢肿瘤细胞脱离肿瘤主体播散进入邻近肺泡腔内(HE×40);B:STAS肿瘤细胞呈单个、簇状、微乳头状结构(HE×200);C:低STAS组(单个、散在肿瘤细胞,HE×400);D:高STAS组(HE×200)。
Figure 2. Pathological morphology and grouping of STAS
图 3 ROR1在肺腺癌中的表达 (IHC ×400)
A:阴性;B:弱阳性 ;C:中阳性 ;D:强阳性。
Figure 3. Expression of ROR1 in lung adenocarcinoma(IHC ×400)
图 4 不同病理亚型肺腺癌STAS发生率与ROR1表达率的关系
Figure 4. The relationship between the incidence of STAS and ROR1 expression in different pathological subtypes of lung adenocarcinoma
图 6 ROR1在STAS阳性肺腺癌中的表达
A、B:ROR1在高STAS组肿瘤中过表达(IHC×100);C、D: STAS肿瘤细胞ROR1呈强阳性表达(IHC×400)。
Figure 6. ROR1 expression in STAS positive lung adenocarcinoma
表 1 STAS与肺腺癌临床病理学特征的关系 [n(%)]
Table 1. Relationship between STAS and clinicopathological features of lung adenocarcinoma[n(%)]
临床病理学参数 n STAS χ2 P + − 性别 1.305 0.253 男 242 82(33.9) 160(66.1) 女 376 111(29.5) 265(70.5) 年龄(岁) 3.388 0.066 < 65 280 98(35.0) 182(65.0) ≥65 338 95(28.1) 243(71.9) 吸烟史 25.262 < 0.001* 无 431 108(25.1) 323(74.9) 有 187 85(45.5) 102(54.5) 肿瘤直径(cm) 191.946 < 0.001* ≤2.5 442 66(14.9) 376(85.1) > 2.5 176 127(72.2) 49(27.8) 组织学形态 123.404 < 0.001* 贴壁型 95 0(0.0) 95(100.0) 腺泡型 255 68(26.7) 187(73.3) 乳头型 148 43(29.1) 105(70.9) 微乳头型 69 49(71.0) 20(29.0) 实体型 51 33(64.7) 18(35.3) 淋巴结转移 139.614 < 0.001* 无 529 108(20.4) 421(79.6) 有 89 73(82.0) 16(18.0) 神经侵犯 30.739 < 0.001* 无 595 169(28.4) 426(71.6) 有 23 19(82.6) 4(17.4) 脉管侵犯 145.165 < 0.001* 无 517 124(24.0) 393(76.0) 有 101 87(86.1) 14(13.9) 胸膜侵犯 225.090 < 0.001* 无 443 83(18.7) 360(81.3) 有 175 146(83.4) 29(16.6) *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 ROR1在不同亚型肺腺癌中的表达 [n(%)]
Table 2. Expression of ROR1 in different subtypes of lung adenocarcinoma[n(%)]
肺腺癌病理亚型 n ROR1 χ2 P + − 贴壁型(高分化) 95 9(9.5) 86(90.5) 腺泡型(中分化) 255 73(28.6) 182(71.4) 乳头型(中分化) 148 49(33.1) 99(66.9) 135.093 < 0.001* 微乳头型(低分化) 69 55(79.7) 14(20.3) 实体型(低分化) 51 41(80.4) 10(19.6) *P < 0.05。
下载: 导出CSV
表 3 ROR1在不同STAS分组中的表达 [n(%)]
Table 3. ROR1 expression in different STAS groups[n(%)]
STAS分组 n ROR1 χ2 P + − 无STAS组 425 45(10.6) 380(89.4) 低STAS组 109 96(88.0) 13(12.0) 372.047 < 0.001* 高STAS组 84 79(94.1) 5(5.9) *P < 0.05。
下载: 导出CSV
-
[1] Sung H,Ferlay J,Siegel R L,et al. Global cancer statistics 2020:GLOBOCAN estimatesof incidence and mortality world wide for 36 cancers in 185 countries[J]. CA Cancer J Clin,2021,71(3):209-249. doi: 10.3322/caac.21660 [2] Siegel R L,Miller K D,Jemal A. Cancer statistics,2020[J]. CA Cancer J Clin,2020,70(1):7-30. doi: 10.3322/caac.21590 [3] Travis W D,Brambilla E,Noguchi M,et al. Interna-tional association for the study of lung cancer/American Thoracic Society/European Respiratory Society international multidiscipli-nary classification of lung adenocarcinoma[J]. J Thorac Oncol,2011,6(2):244-285. doi: 10.1097/JTO.0b013e318206a221 [4] Travis W D,Brambilla E,Nicholson A G,et al. The 2015 World Health Organization classification of lung tumors:impact of genetic,clinical and radiologic advancessince the 2004 classification[J]. J Thorac Oncol,2015,10(9):1243-1260. doi: 10.1097/JTO.0000000000000630 [5] Vaghjiani R G,Takahashi Y,Eguchi T,et al. Tumor spread through air spaces (STAS)is predictor of occult lymphnodeme-tastasis in clinical stage IA lung adenocarcinoma[J]. J Thorac Oncol,2020,15(5):792-802. doi: 10.1016/j.jtho.2020.01.008 [6] Masiakowski P,Carroll R D. A novel family of cell surface receptors with tyrosine kinase-like domain[J]. J Biol Chem,1992,267(36):26181-26190. doi: 10.1016/S0021-9258(18)35733-8 [7] Borcherding N,Kusner D,Liu G H,et al. ROR1,an embryonic protein with an emerg-ing role in cancer biology[J]. Protein Cell,2014,5(7):496-502. doi: 10.1007/s13238-014-0059-7 [8] Kipps T J. ROR1:An orphan becomes apparent[J]. Blood,2022,140(14):1583-1591. doi: 10.1182/blood.2021014760 [9] Green J L, Kuntz S G, Sternberg P W. Ror receptor tyrosine kinases: orphans no more[J]. Trends Cell Biol, 2008, 18(11): 536-544. [10] Chiang C L,Goswami S,Frissora F,et al. ROR1-targeted delivery of miR-29b induces cell cycle arrest and therapeutic benefit in vivo in CLL mouse model[J]. Blood,2019,134(5):432-444. doi: 10.1182/blood.2018882290 [11] Zhang S,Cui B,Lai H,et al. Ovarian cancer stem cells express ROR1,which can be targeted for anti-cancer-stem-cell therapy[J]. Proc Natl Acad Sci USA,2014,111(48):17266-17271. doi: 10.1073/pnas.1419599111 [12] Rich B E,Hojjat-Farsangi M,Ghaemimanesh F,et al. Inhibition of the receptor tyrosine kinase ROR1 by anti-ROR1 monoclonal antibodies and siRNA induced apoptosis of melanoma cells[J]. PLoS One,2013,8(4):e61167. doi: 10.1371/journal.pone.0061167 [13] Zhang S P,Chen L G,Cui B,et al. ROR1 is expressed in human breast cancer and associated with enhanced tumor-cell growth[J]. PLoS One,2012,7(3):e31127. doi: 10.1371/journal.pone.0031127 [14] Villalbalj A,Shih A R,Sayo T M S,et al. Accuracy andreproducibility of intraop-erative assessment on tumor spread through air spaces(STAS)in stage l lung adenocarcinomas[J]. J Thorac Oncol,2021,16(4):619-629. doi: 10.1016/j.jtho.2020.12.005 [15] Kadota K,Nitadori J I,Sima C S,et al. Tumor spread through air spaces is an important pattern of invasion and impacts the frequency and location of recurrences after limited resection for small stage I lung adenocarcinomas[J]. J Thorac Oncol,2015,10(5):806-814. [16] Uruga H,Fujii T,Fujimori S,et al. Semiquantitative assessment of tumor spread through air spaces (STAS) in early-stage lung adenocarcinomas[J]. Journal of Thoracic Oncology,2017,12(7):1046-1051. doi: 10.1016/j.jtho.2017.03.019 [17] Toyokawa G,Yamada Y,Tagawa T,et al. Significance of spread through air spaces in resected pathological stage I lung adenocarcinoma[J]. Ann Thorac Surg,2018,105(6):1655-1663. doi: 10.1016/j.athoracsur.2018.01.037 [18] Alvarez Moreno J C,Aljamal A A,Bahmad H F,et al. Correlation between spread through air spaces (STAS) and other clinicopathological parameters in lung cancer[J]. Pathol Res Pract,2021,220(4):153376. doi: 10.1016/j.prp.2021.153376.Epub2021Feb16 [19] 王作刚,冯彦,于亮,等. ROR1对人肺癌A549细胞上皮-间质转化的影响[J]. 肿瘤防治研究,2018,45(7):458-462. [20] Gentile A,Lazzari L,Benvenuti S,et al. The ROR1 pseudokinase diversifies signaling outputs in MET-addicted cancer cells[J]. Int J Cancer,2014,135(10):2305-2316. doi: 10.1002/ijc.28879 [21] Cui B,Zhang S,Chen L,et al. Targeting RORI inhibits epithelial-mesenchymal transition and metastasis[J]. Cancer Res,2013,73(12):3649-3660. doi: 10.1158/0008-5472.CAN-12-3832 [22] 马文琦,何鑫,张红丽,等. 下调结直肠癌细胞受体酪氨酸激酶样孤儿受体抑制细胞生长并促进其凋亡[J]. 细胞与分子免疫学杂志,2016,32(5):655-659,665. doi: 10.13423/j.cnki.cjcmi.007760 [23] Tomoya,Yamaguchi,Can Lu,et al. ROR1 sustains caveolae and survival signalling as a scaffold of cavin-1 and caveolin-1[J]. Nature Communications,2016,7(4):10060. doi: 10.1038/ncomms10060 [24] Zheng Y Z,Ma R,Zhou J,et al. ROR1 is a novel prognostic biomarker in patients with lung adenocarcinoma[J]. Scientific Reports,2016,6(10):36447. [25] Onozato Y,Nakajima T,Yokota H,et al. Radiomics is feasible for prediction of spread through air spaces in patients with nonsmall cell lung cancer[J]. Scientific Reports,2021,11(1):13526. doi: 10.1038/s41598-021-93002-4 [26] Han Y B,Kim H,Mino-Kenudson M,et al. Tumor spread through air spaces (STAS):prognostic significance of grading in non-small cell lung cancer[J]. Mod Pathol,2021,34(3):549-561. doi: 10.1038/s41379-020-00709-2 [27] Chae M,Jeon J H,Chung J H,et al. Prognostic significance of tumor spread through air spaces in patients with stage IA part-solid lung adenocarcinoma after sublobar resection[J]. Lung Cancer,2021,152(2):21-26. 期刊类型引用(0)
其他类型引用(1)
-

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 3662
- HTML全文浏览量: 2349
- PDF下载量: 150
- 被引次数: 1
