

Accuracy of Sub-axial Cervical Pedicle Screw Placement:A Systematic Review with the Meta-analysis Comparing Free-hand and Assistant Techniques
-
摘要:
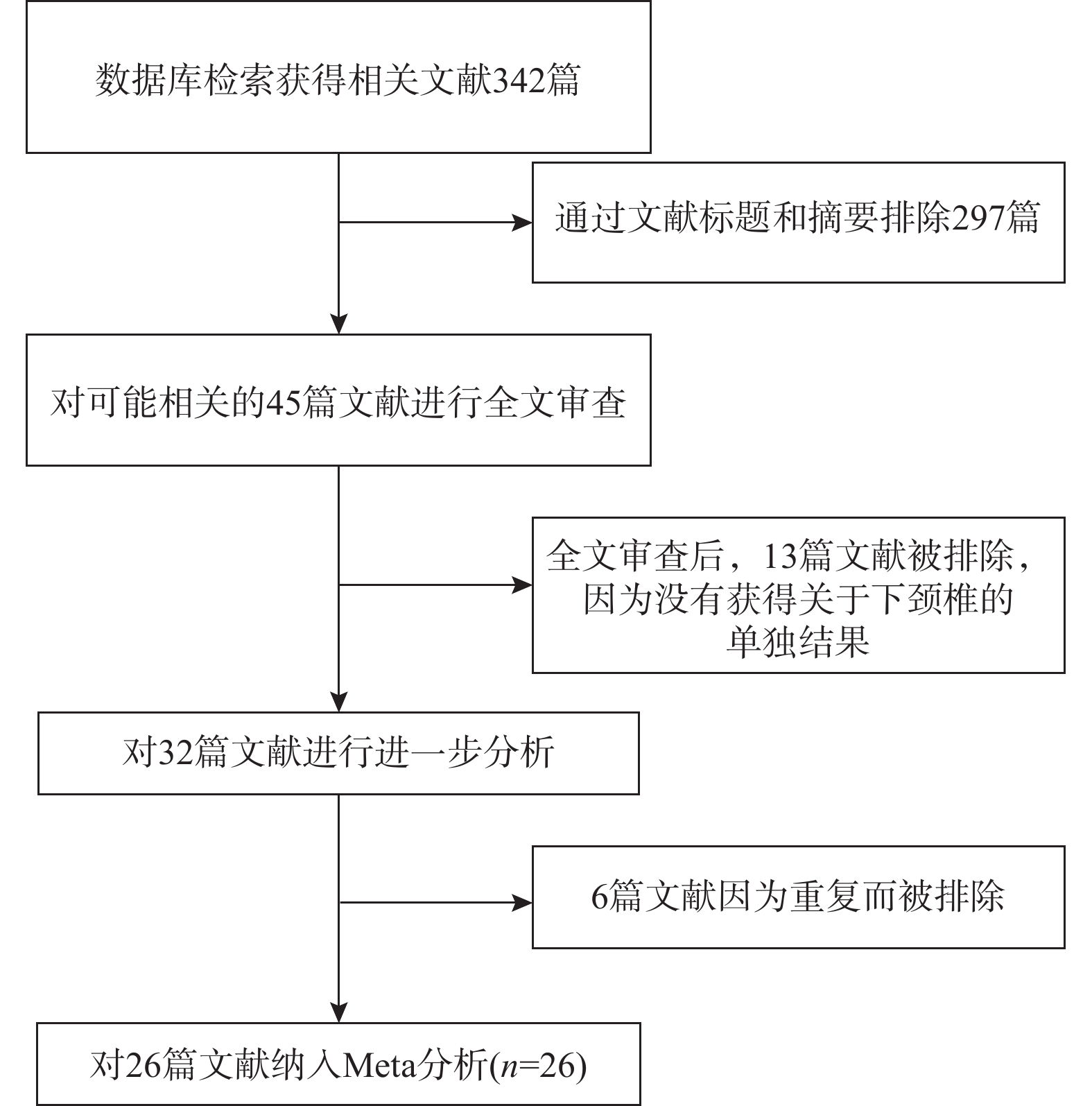
目的 系统比较徒手与辅助技术下颈椎椎弓根螺钉(sub-axial cervical pedicle screw sCPS)置入的准确性、螺钉穿破椎弓根方向以及螺钉相关并发症。 方法 检索Medline、Embase以及Cochrane数据库,收集2010年1月至2022年12月研究不同置钉技术下颈椎椎弓根螺钉置入准确性的高质量英文文献,根据纳入标准筛选文献、数据提取,使用RevMan 5.4进行Meta分析。 结果 共纳入26项研究,1697名患者,6654颗螺钉。Meta分析示:辅助技术置入sCPS有更高的准确率。穿破椎弓根外壁比内壁更常见,徒手技术置钉穿破上壁比下壁更常见,辅助技术置钉上壁和下壁穿破率,差异暂无统计学意义。 结论 (1)辅助技术较徒手技术对于置入sCPS有更高的准确性;(2)穿破椎弓根外壁和下壁比穿破内壁和上壁更常见;(3)sCPS置入的准确性评估需要统一的评估标准;(4)不同的辅助置钉技术各有优劣,应根据实际情况选择。 Abstract:Objective To systematically compare the accuracy, direction of pedicle screw perforation, and screw-related complications of sub-axial cervical pedicle screw (sCPS) placement with and without assistant techniques. Methods A total of 26 studies involving 1697 patients and 6654 screws were included. Medline, Embase, and Cochrane databases were searched to collect the high-quality English literature on the accuracy of cervical pedicle screw (CPS) placement using different screw placement techniques from 2010.1 to 2022.12. Literature was screened according to the inclusion criteria, data was extracted, and a meta-analysis was performed using RevMan 5.4. Results The meta-analysis showed that assistant techniques had a higher accuracy rate for sCPS placement. Perforation of the lateral wall of the pedicle was more common than the medial wall, and free-hand screw placement was more common in the superior wall than the inferior wall. There was no statistically significant difference in the perforation rate between the superior and inferior walls with assistant techniques. Conclusion 1. Assistant techniques has a higher accuracy rate for sCPS placement than free-hand techniques. 2. Perforation of the lateral and inferior walls of the pedicle is more common than perforation of the medial and superior walls. 3. A unified evaluation standard is needed for assessing the accuracy of sCPS placement. 4. Different assistant screw placement techniques have their own advantages and disadvantages, and should be selected according to the actual conditions. -
Key words:
- Systematic review /
- Pediclescrew /
- Sub-axial cervical
-
子宫内膜容受性是指子宫内膜对受精卵着床的能力,对于辅助生殖技术的成功率具有重要影响[1]。传统对子宫内膜容受性评估方法主要包括宫腔镜检查、活体组织学检查,但传统方法往往存在一定局限性和入侵性,而且在准确性与可靠性方面也存在一定的挑战[2−3]。超声检查评估作为1种无创、无痛、无辐射的检查方式,其具有实时、动态、可以重复观察的优点,可以清晰地显示子宫内膜的结构和血流状态[4]。近年来,随着超声技术的发展,经阴道三维超声技术已经成为评估辅助生殖者子宫内膜容受性的重要手段[5−6]。大量研究表明[7],利用经阴道三维超声技术对辅助生殖者的子宫内膜类型、血流分型、子宫内膜容积、子宫内膜及内膜下血流参数等参数进行评估,以准确预测胚胎移植的妊娠结局,因此,在子宫内膜容受性判定中具有重要价值,然而,目前对于这些参数的评估标准尚未统一,仍需要进一步的研究和探讨[8−9]。基于此,本研究选取昆明市妇幼保健院2022 年 4月至2023 年6 月106 例拟行辅助生殖者,通过对比妊娠组和未妊娠组的数据,探讨子宫内膜形态、容积与血流参数以及妊娠结果之间的关系,分析影响子宫内膜容受性的因素,为临床医生提供更准确的辅助生殖决策依据,评估子宫动脉和内膜动脉血流动力学指标,探讨其在子宫内膜容受性评估中的作用。
1. 资料与方法
1.1 一般资料
选取昆明市妇幼保健院2022 年4 月至2023 年6 月106 例拟行辅助生殖者,在妊娠前均接受经阴道三维超声检测,根据临床妊娠与否分为妊娠组(n = 48 )和未妊娠组(n = 58 )。纳入标准[10]:(1)年龄24~49 岁,拟行辅助生殖技术的女性患者;(2)月经周期1~47 d;(3)无严重心、肝、肾等重要脏器疾病;(4)无生殖系统肿瘤疾病、子宫内膜异位症等影响子宫内膜容受性的疾病;(5)无内分泌失调、免疫系统疾病等影响生育的疾病。排除标准[11]:(1)生殖道炎性、出血性疾病以及存在宫腔宫颈粘连情况者;(2)子宫内膜出现息肉、粘膜下肌瘤或者存在子宫内膜异位症与子宫畸形情况者;(3)甲状腺功能异常状况者;(4)卵巢储备功能降低、早发性卵巢功能不全以及存在卵巢早衰情况者;(5)免疫性不孕症者;(6)精神系统疾病者。本研究已获得昆明市妇幼保健院医学伦理会批准(2022-04-32),且知情同意书所有患者均已签署。
1.2 研究方法
采用彩色多普勒超声 (仪器型号:GE Voluson E10及三维能量多普勒超声成像技术,经阴道三维容积探头。设置探头频率(6~10 MHz之间)、脉冲频率(0.6 kHz)扫查角度(180° )、颜色质量等参数,以确保获取清晰的子宫内膜图像。患者排空膀胱并保持膀胱截石位,并确保探头消毒干净,探头顶端应用一次性用超声隔离套,将阴道超声 探头缓慢置入患者阴道内,直至后穹窿处,观察子宫、附件区与盆腔的情况,记录子宫内膜的形态和厚度;启动三维成像模式,获取子宫内膜的三维重建图像。实时记录并存储所有获取的超声图像和数据,以便后续分析。
1.3 观察指标
(1)记录宫内膜类型、子宫内膜血流分型、子宫内膜容积。子宫内膜类型,A型:子宫内膜三线征清晰,子宫腔内中线回声明显,子宫肌层和子宫内膜之间有强回声的子宫蜕膜基质,呈“三明治”结构;B型:子宫内膜与子宫肌层分界线变得模糊,子宫腔内中线回声不清或消失;C型:子宫内膜回声与子宫肌层回声相似,无明显的子宫内膜中线回声;子宫内膜血流分型:Ⅰ级表示子宫内膜内未见血流信号,Ⅱ级表示子宫内膜内可见点状或小条状血流信号,Ⅲ级表示子宫内膜内可见丰富的螺旋状或树枝状血流信号;子宫内膜容积:运用三维能量多普勒超声设备,借助三维成像,使用VOCAL分析软件(模式:手动勾画),切面间为30度进行勾画,计算出子宫内膜容积。(2)记录子宫内膜指标以及内膜下血流参数,涵盖血流指数(FI)以及血管化指数(VI)与血管-血流指数(VFI)指标,应用直方图分析软件,获取血流参数信息,选择内膜下区域厚度1 mm,取得内膜下VI、FI、VFI数值,对每个指标进行测量,每次测量后均取平均值,共测量3 次。
1.4 统计学处理
应用SPSS22.0实行统计学分析,其中,计量资料用均数±标准差($\bar x \pm s $)表示,组间比较采用t检验;计数资料采用(n,%)表示,组间比较采用χ2检验,以P < 0.05为差异有统计学意义。
2. 结果
2.1 一般资料比较
2 组在年龄、BMI、不孕类型方面比较,差异无统计学意义(P > 0.05),见表1。
表 1 2组一般资料比较[($\bar x \pm s $)/n(%)]Table 1. Comparison of general data between the two groups[($\bar x \pm s $)/n(%)]组别 n 平均年龄(岁) BMI(kg/m2) 不孕类型 原发性不孕 继发性不孕 不明原因不孕 妊娠组 48 30.7±6.1 21.65±2.56 33(68.75) 13(27.08) 2(4.17) 未妊娠组 58 32.5±5.6 22.07±2.35 41(70.69%) 14(24.14) 3(5.17) t/χ2 / 1.387 1.194 1.176 P / 0.170 0.235 0.915 2.2 2组子宫内膜类型、血流分型分布及容积情况比较
妊娠组中,子宫内膜类型以A型为主,占比达58.33 %,B型与C型分别占比为22.92 %、18.75 %;未妊娠组中,A型子宫内膜类型占比32.76 %,但B型与C型子宫内膜的分布相对均衡,占比分别为31.03 %、36.21 %;妊娠组子宫内膜容积大于未妊娠组,差异有统计学意义(P < 0.05),见表2。
表 2 2 组子宫内膜类型、血流分型分布及容积情况比较[($\bar x \pm s $)/n(%)]Table 2. Comparison of endometrial types,blood flow classification distribution and volume between the two groups[($\bar x \pm s $)/n(%)]组别 n 子宫内膜类型 子宫内膜血流分型 子宫内膜容积(mL) A型 B型 C型 Ⅰ级 Ⅱ级 Ⅲ级 妊娠组 48 28(58.33) 11(22.92) 9(18.75) 5(10.42) 14(29.17) 29(60.42) 3.52±1.31 未妊娠组 58 19(32.76) 18(31.03) 21(36.21) 27(46.55) 16(27.59) 15(25.86) 0.86±1.12 χ2/t / 6.265 6.457 4.962 P / 0.043* 0.039* 0.001* *P < 0.05。 2.3 子宫内膜类型、子宫内膜血流分型与妊娠率
妊娠组子宫内膜形态分型为A、B、C妊娠率分别为59.57 %(28/47)、37.93 %(11/29)、30.00 %(9/30),A型妊娠率明显高于C型,差异有统计学意义(χ2 = 4.100,P = 0.043);其中,A型与B型、B型与C型之间比较差异无统计学意义(χ2 = 0.095、0.039,P = 0.775、0.840)。
妊娠组子宫内膜血流分型为Ⅰ级、Ⅱ级、Ⅲ级妊娠率分别为15.63 %(5/32)、46.67 %(14/30)、65.91 %(29/44),Ⅲ级妊娠率明显高于Ⅰ级,差异有统计学意义(χ2 = 16.518,P = 0.001);其中,Ⅲ级与Ⅱ级、Ⅱ级与Ⅰ级之间比较,差异无统计学意义(χ2=0.002、0.018, P = 0.925,0.899)。
2.4 2组子宫内膜及内膜下血流的血流参数和血管化程度比较
妊娠组子宫内膜在VI、FI 、VFI方面比较均高于未妊娠组,差异有统计学意义(P < 0.05);妊娠组子宫内膜下在VI、FI 、VFI方面比较均高于未妊娠组,差异有统计学意义(P < 0.05),见表3。
表 3 2 组子宫内膜及内膜下血流的血流参数和血管化程度比较($\bar x \pm s $)(1)Table 3. Comparison of blood flow parameters and degree of vascularization of endometrial and subendometrial blood flow between the two groups($\bar x \pm s $)(1)组别 n 子宫内膜 VI FI VFI 妊娠组 48 22.41±3.12 32.15±2.63 6.59±1.09 未妊娠组 58 16.54±2.56 28.66±2.60 4.89±0.88 t / 6.973 4.475 4.254 P / 0.001* 0.001* 0.001* *P < 0.05。 表 3 2 组子宫内膜及内膜下血流的血流参数和血管化程度比较($\bar x \pm s $)(2)Table 3. Comparison of blood flow parameters and degree of vascularization of endometrial and subendometrial blood flow between the two groups($\bar x \pm s $)(2)组别 n 子宫内膜下 VI FI VFI 妊娠组 48 44.23±3.79 33.27±3.07 15.62±2.27 未妊娠组 58 36.15±3.55 30.79±3.17 11.16±2.07 t / 7.606 3.573 7.552 P / 0.001* 0.001* 0.001* *P < 0.05。 3. 讨论
3.1 生殖医学中子宫内膜容受性评估现状
子宫内膜容受性评估是生殖医学领域的关键环节,在辅助生殖技术中,准确评估子宫内膜容受性对辅助生殖者胚胎移植的成功至关重要[12−13]。传统评估方法包括宫腔镜检查和组织活检,在一定程度上发挥重要作用,但随着现代医学科技的不断进步以及生殖医学领域的需求,传统方法对辅助生殖者评估方面存在明显的局限性与不足,传统评估方法无法提供动态、实时的信息,其次,宫腔镜检查是一种有创性检查,存在导致子宫内膜潜在的损伤,从而对胚胎着床产生不良影响,此外,宫腔镜检查给患者带来不适或存在轻微疼痛感,在宫腔镜检查时往往需要在宫颈处局部麻醉,且存在一定风险,检查后需要足够时间恢复[14−15];组织活检虽然能够提供子宫内膜的病理学信息,但同样属于一种有创性操作,极容易引起子宫内膜炎症、出血等并发症,对子宫内膜容受性产生不良影响[16−17]。相比之下,近年来经阴道三维超声的发展为子宫内膜容受性的非侵入性、安全与可重复评估提供新的选择,方法克服传统方法的创伤性和不便性,为医生提供更全面、准确的子宫内膜容受性评估手段。
3.2 三维超声评估子宫内膜对妊娠的影响
经阴道三维超声是1种无创、无痛、无辐射且属于非侵入性的超声技术,具有高分辨率与准确性的特点,能够提供辅助生殖者的子宫内膜形态、分型、血流以及容积等方面的详细信息[18]。子宫内膜的形态和分型对于判断其容受性具有重要意义,对子宫内膜的A型和B型在接受胚胎移植时有着不同的成功率。结果显示,子宫内膜类型与妊娠成功概率具有明显相关性,妊娠组A型子宫内膜妊娠率最高,为59.57 %、B型为37.93 %、C型妊娠率最低仅为30.00 %,说明子宫内膜类型对妊娠具有重要影响,利于胚胎着床与发育的子宫内膜类型是A型,在超声评估中子宫内膜类型的判定有助于预测妊娠者生育能力,陈慧佳等[19]研究表明,子宫内膜A型与子宫内膜B型妊娠率分别为78.48%、45.76%,而子宫内膜C型妊娠率最低,观点与本研究基本一致。其次,子宫内膜血流分型与妊娠率也呈显著相关性,结果中,Ⅰ级血流分型妊娠率最低,仅为15.63 %,Ⅱ级为46.67 %,Ⅲ级最高为65.91 %,说明子宫内膜血流状态对妊娠影响的重要性,妊娠者良好的血流状态则有助于提高妊娠率。研究还显示,妊娠组子宫内膜容积显著高于未妊娠组(P < 0.05),子宫内膜的容积是评估其容受性的重要参数,研究数据则说明子宫内膜的容积太小则不利于胚胎着床,而大小适中的子宫内膜容积则可以成功提升成功率,子宫内膜容积的增加与子宫内膜的血流灌注有关,可以更好满足胚胎的发育需求。
3.3 三维超声评估子宫内膜血流对妊娠的影响
经阴道三维超声通过彩色多普勒超声和三维能量多普勒超声成像技术可以评估子宫内膜及内膜下血流的情况[20]。血流指数、血管化指数和血管-血流指数参数是反映子宫内膜营养供应和血流灌注程度的指标,其与子宫内膜容受性密切相关,血流丰富、血管化程度高的子宫内膜更有利胚胎的着床[21-23]。研究发现,妊娠组的子宫内膜及内膜下血流指数、血管化指数和血管-血流指数均显著高于未妊娠组(P < 0.05),表明妊娠组的子宫内膜具有更好的血流灌注和血管发育情况,其良好的血流灌注可以为胚胎提供足够的营养和氧气,促进其正常胚胎发育与着床。杨彬等[24]学者研究认为较高的VI、FI和VFI值表明子宫内膜的血流灌注较好,有利于胚胎的植入和发育,同时,适当的血管化程度可能有助于提高IVF-ET的成功率,对预测妊娠结局具有重要价值。研究通过经阴道三维超声技术,在评估子宫内膜容受性方面呈现显著的创新性和独特价值,相较于传统的有创检查方法,经阴道三维超声方法具非侵入性、安全,降低患者不适感和风险,提供更全面、准确的信息[25-26];研究还强调血流指数、容积等参指数对胚胎着床与发育的重要性,为优化辅助生殖治疗方案提供新方向,提供个性化治疗,提高妊娠成功率,为辅助生殖医学带来新的思路。
综上所述,在辅助生殖技术中,子宫内膜容受性评估在辅助生殖技术中扮演着关键角色。传统评估方法存在诸多局限性,如有创性、局部麻醉需求及潜在并发症。经阴道三维超声弥补了传统方法的不足,通过形态、血流等方面评估,判断子宫内膜容受性,其中子宫内膜类型、血流状态和容积与妊娠成功率密切相关;良好的血流灌注和血管发育有助于提高着床率,而适中的子宫内膜容积对胚胎发育至关重要;血流指数和血管化程度反映子宫内膜的营养供应情况,对胚胎发育起着关键作用;因此,经阴道三维超声作为一种准确评估方法,对于提高辅助生殖技术成功率具有重要意义。
本研究存在局限性,样本量相对较小,且存在样本选择偏倚的问题,同时,研究仅关注超声评估子宫内膜容受性,而胚胎着床受多种因素影响,因此需要进一步开展多中心、加大样本,对其影响因素进行更为深入的探讨。
综上所述,子宫内膜容受性是胚胎成功着床的关键,而经阴道三维超声为其准确评估提供可靠超声诊断手段。通过该技术,可以获得更为全面和详细的子宫内膜类型、子宫内膜血流分型、容积、血流参数指标信息,对评估子宫内膜的适应性、血流灌注情况以及胚胎着床具有重要意义。
-
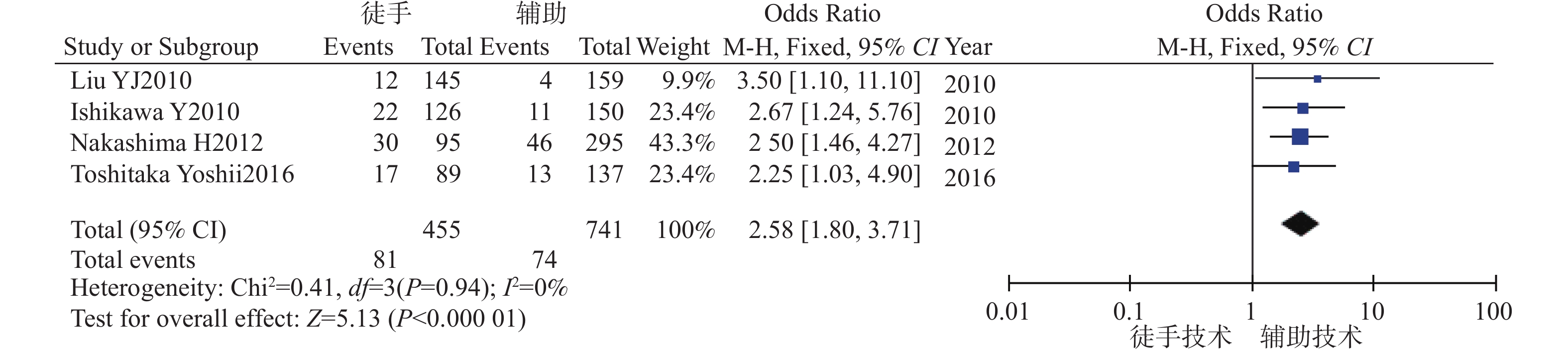
图 2 徒手置钉技术与辅助置钉技术准确率的Meta分析
Figure 2. Meta analysis of the accuracy of free-hand techniques vs assisted techniques
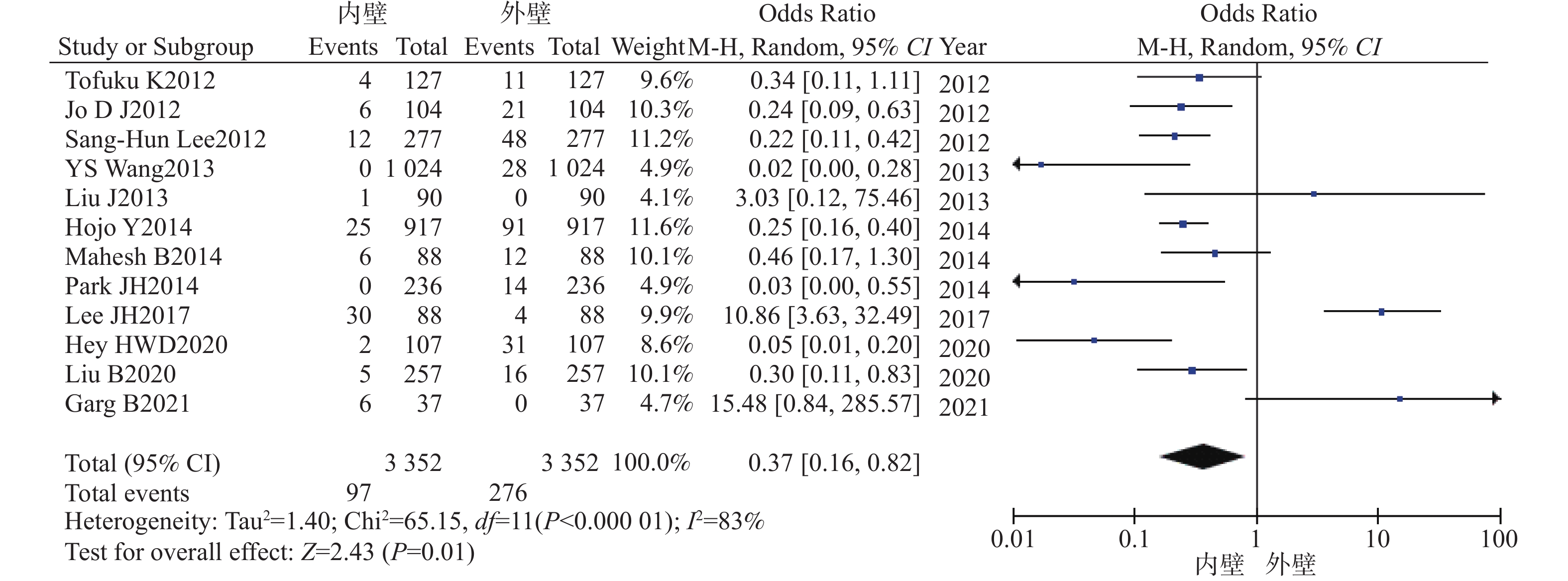
图 3 徒手置钉组穿破椎弓根内外壁的森林图
Figure 3. Forest plot of the free-hand techniques group perforation the medial and lateral walls of the pedicle

图 4 徒手置钉组穿破椎弓根上下壁的森林图
Figure 4. Forest plot of the free-hand techniques group perforation the superior and inferior walls of the pedicle
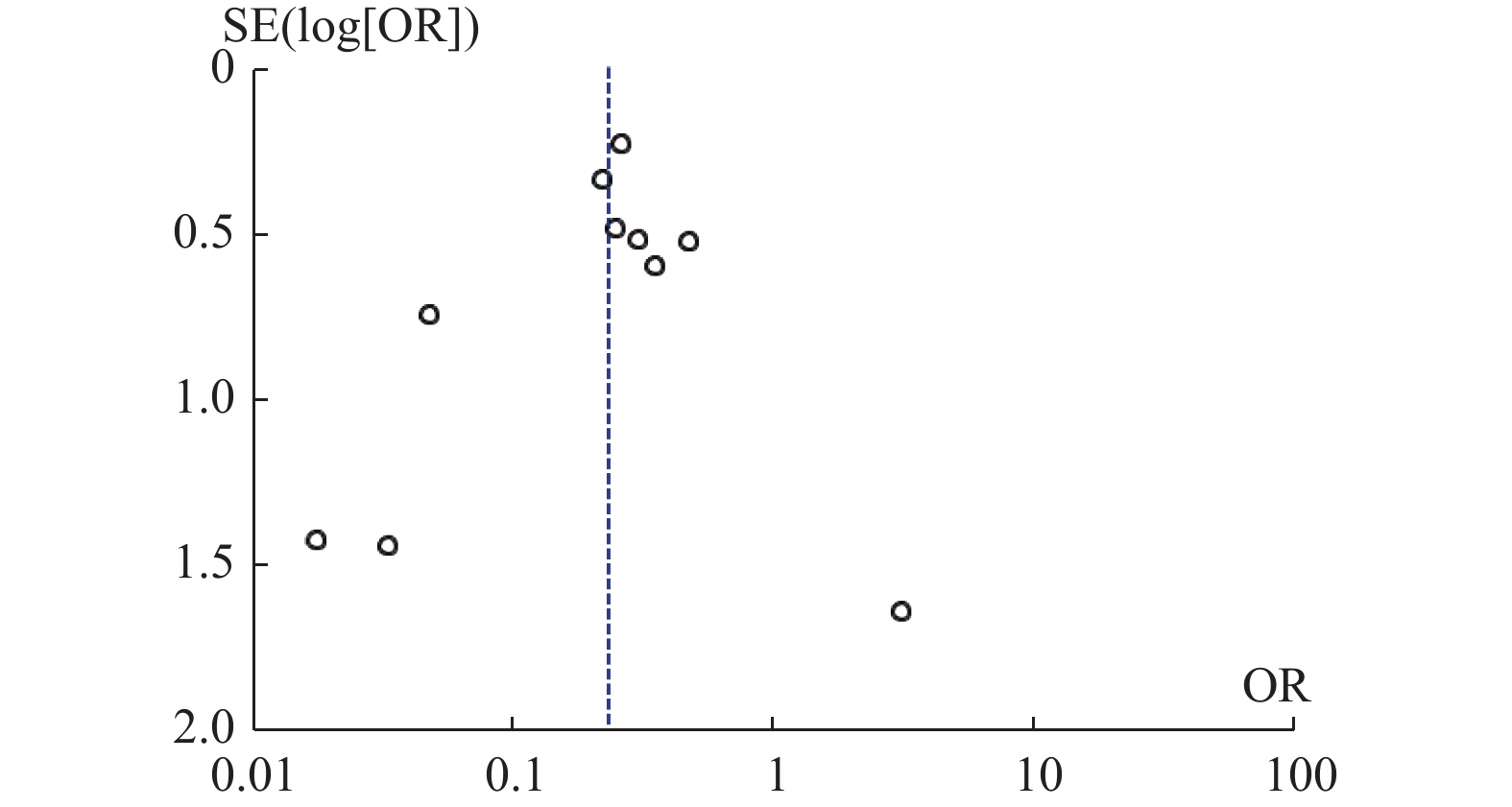
图 5 徒手置钉组穿过椎弓根内外壁的漏斗图
Figure 5. Funne plot of the free-hand techniques group perforation the medial and lateral walls of the pedicle
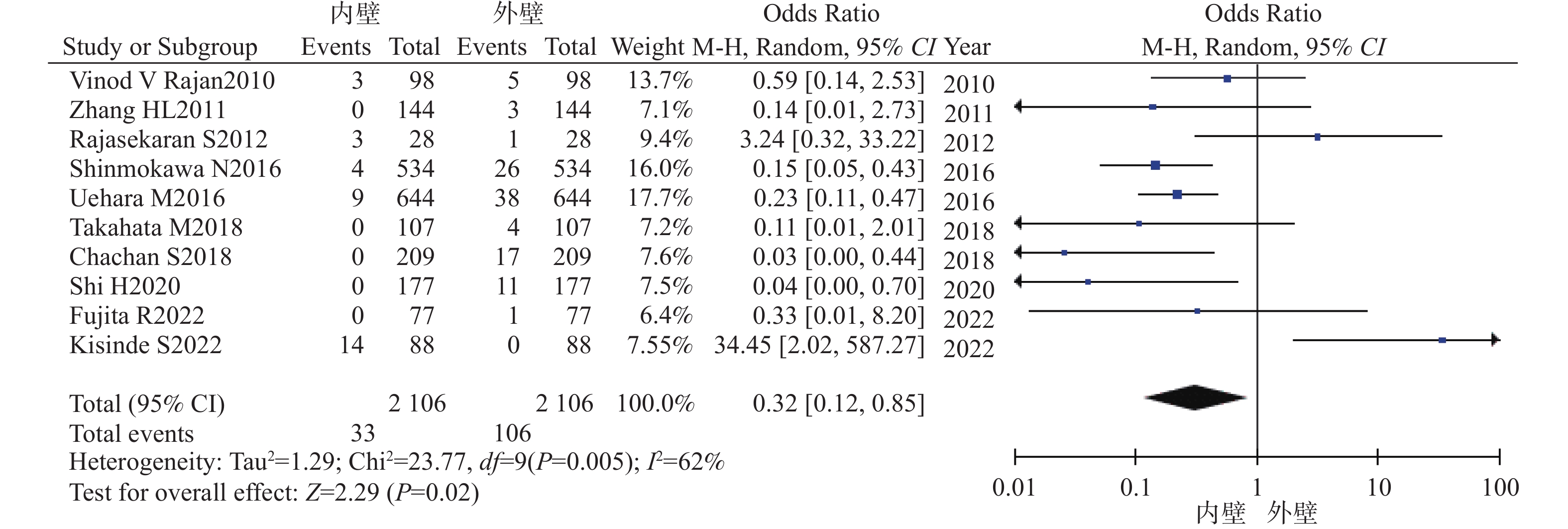
图 6 辅助置钉组穿破椎弓根内外壁的Meta分析
Figure 6. Meta analysis of the assisted techniques group perforation the medial and lateral walls of the pedicle
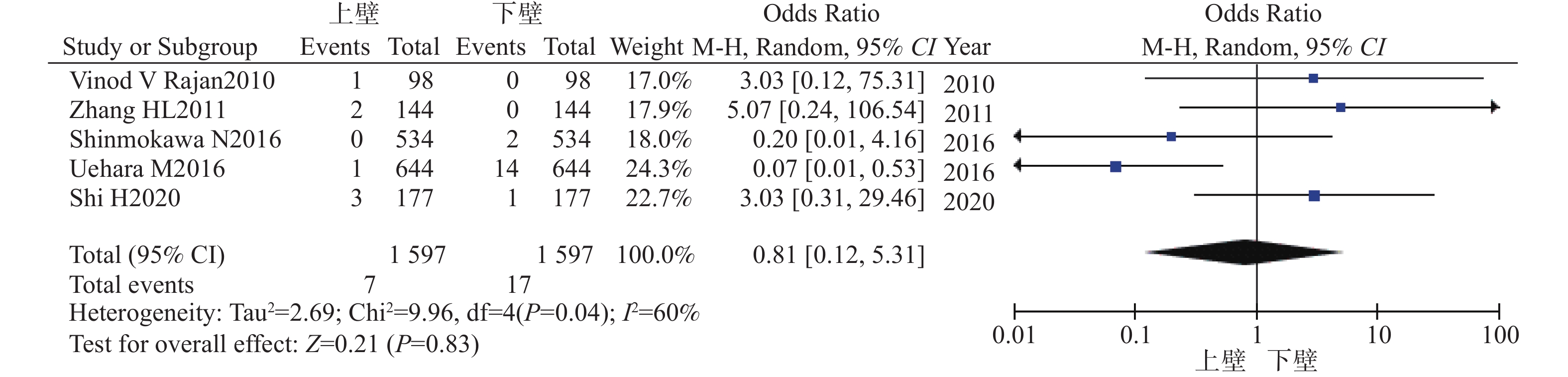
图 7 辅助置钉组穿破椎弓根上下壁的Meta分析
Figure 7. Meta analysis of the assisted techniques group perforation the superiorly and inferiorly walls of the pedicle
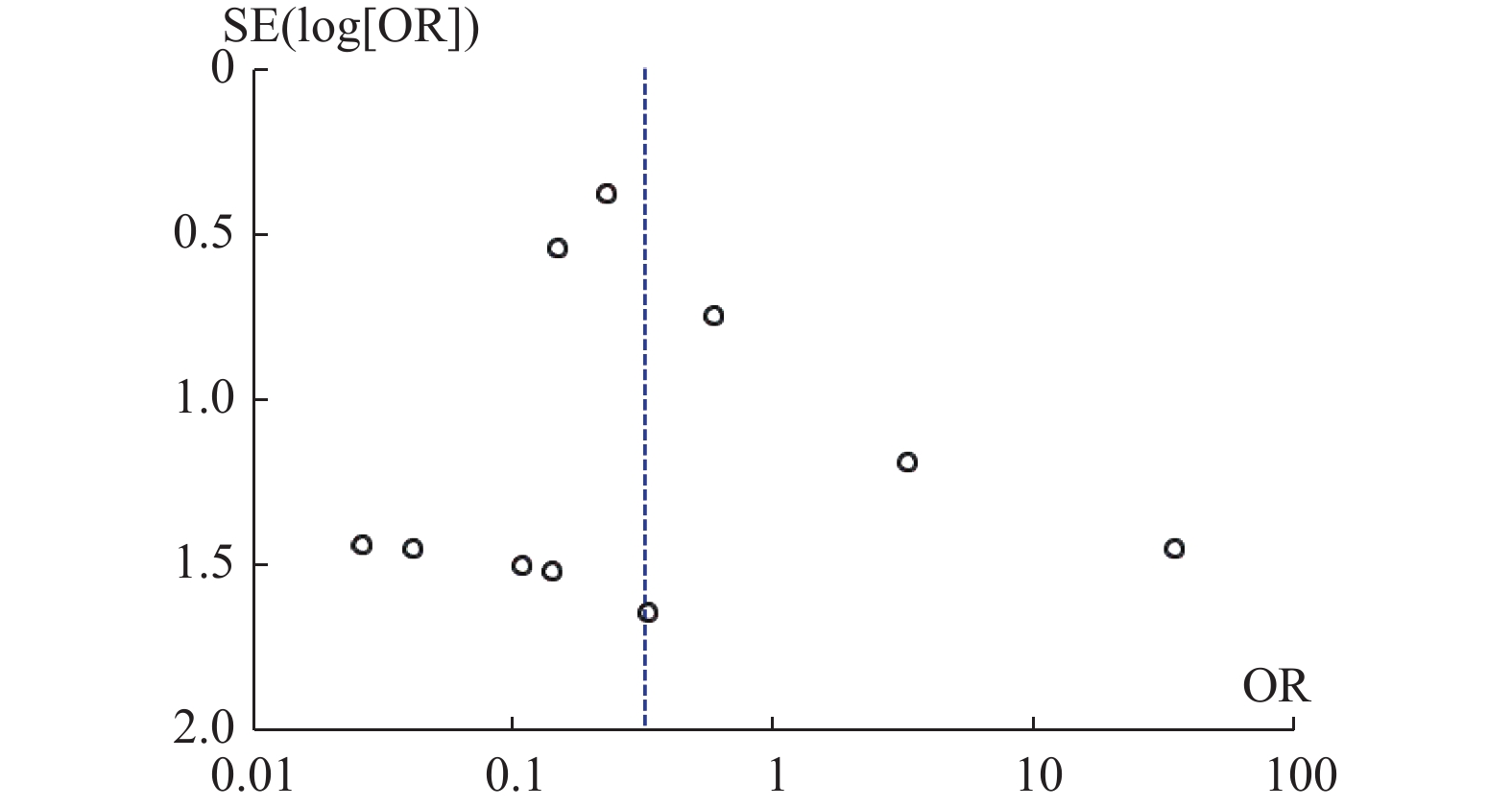
图 8 辅助置钉组穿过椎弓根内外壁的漏斗图
Figure 8. Funne plot of the assisted techniques group perforation the medial and lateral walls of the pedicle
-
[1] Abumi K,Itoh H,Taneichi H,et al. Transpedicular screw fixation for traumatic lesions of the middle and lower cervical spine: Description of the techniques and preliminary report[J]. Journal of Spinal Disorders,1994,7(1):19-28. doi: 10.1097/00002517-199407010-00003 [2] Abumi K,Shono Y,Ito M,et al. Complications of pedicle screw fixation in reconstructive surgery of the cervical spine[J]. Spine,2000,25(8):962969. [3] Kotani Y,Cunningham B W,Abumi K,et al. Biomechanical analysis of cervical stabilization systems. An assessment of transpedicular screw fixation in the cervical spine[J]. Spine (Phila Pa,1976,),1994,19(22):2529-2539. [4] Jo D J,Seo E M,Kim K T,et al. Cervical pedicle screw insertion using the technique with direct exposure of the pedicle by laminoforaminotomy[J]. J Korean Neurosurg Soc,2012,52(5):459-465. doi: 10.3340/jkns.2012.52.5.459 [5] Lee S H,Kim K T,Abumi K,et al. Cervical pedicle screw placement using the "key slot technique": The feasibility and learning curve[J]. J Spinal Disord Tech,2012,25(8):415-421. doi: 10.1097/BSD.0b013e3182309657 [6] Tofuku K,Koga H,Komiya S. Cervical pedicle screw insertion using a gutter entry point at the transitional area between the lateral mass and lamina[J]. Eur Spine J,2012,21(2):353-358. doi: 10.1007/s00586-011-1969-1 [7] Wang Y,Xie J,Yang Z,et al. Computed tomography assessment of lateral pedicle wall perforation by free-hand subaxial cervical pedicle screw placement[J]. Arch Orthop Trauma Surg,2013,133(7):901-909. doi: 10.1007/s00402-013-1752-3 [8] Liu J,Li Y,Wu Y,et al. A novel method of cervical pedicle screw placement from C3 to C5 and its clinical applications[J]. Spine (Phila Pa,1976,),2013,38(8):E504-E512. [9] Hojo Y,Ito M,Suda K,et al. A multicenter study on accuracy and complications of freehand placement of cervical pedicle screws under lateral fluoroscopy in different pathological conditions: CT-based evaluation of more than 1,000 screws[J]. Eur Spine J,2014,23(10):2166-2174. doi: 10.1007/s00586-014-3470-0 [10] Mahesh B,Upendra B,Mahan RS. The medial cortical pedicle screw-a new technique for cervical pedicle screw placement with partial drilling of medial cortex[J]. Spine J,2014,14(2):371-380. doi: 10.1016/j.spinee.2013.09.033 [11] Park J H,Jeon S R,Roh S W,et al. The safety and accuracy of freehand pedicle screw placement in the subaxial cervical spine: A series of 45 consecutive patients[J]. Spine (Phila Pa,1976,),2014,39(4):280-285. [12] Lee JH,Choi BK,Han IH,et al. Cervical sedicle screw placement using medial funnel technique[J]. Korean J Spine,2017,14(3):84-88. doi: 10.14245/kjs.2017.14.3.84 [13] Liu B,Liu X,Shen X,et al. The "slide technique"-a novel free-hand method of subaxial cervical pedicle screw placement[J]. BMC Musculoskelet Disord,2020,21(1):399. doi: 10.1186/s12891-020-03420-0 [14] Hey H W D,Zhuo W H,Tan Y H J,et al. Accuracy of freehand pedicle screws versus lateral mass screws in the subaxial cervical spine[J]. Spine Deform,2020,8(5):1049-1058. doi: 10.1007/s43390-020-00119-z [15] Garg B,Mehta N. Safety and feasibility of cervical pedicle screw insertion in pediatric subaxial cervical spine without navigation: A retrospective cohort study[J]. J Pediatr Orthop,2021,41(2):119-126. doi: 10.1097/BPO.0000000000001694 [16] V Rajan V,Kamath V,Shetty A P,et al. Iso-C3D navigation assisted pedicle screw placement in deformities of the cervical and thoracic spine[J]. Indian J Orthop,2010,44(2):163-168. doi: 10.4103/0019-5413.62083 [17] Zhang H L,Zhou D S,Jiang Z S. Analysis of accuracy of computer-assisted navigation in cervical pedicle screw installation[J]. Orthop Surg,2011,3(1):52-56. doi: 10.1111/j.1757-7861.2010.00110.x [18] Shimokawa N,Takami T. Surgical safety of cervical pedicle screw placement with computer navigation system[J]. Neurosurg Rev,2017,40(2):251-258. doi: 10.1007/s10143-016-0757-0 [19] Uehara M,Takahashi J,Ikegami S,et al. Screw perforation rates in 359 consecutive patients receiving computer-guided pedicle screw insertion along the cervical to lumbar spine[J]. Eur Spine J,2017,26(11):2858-2864. doi: 10.1007/s00586-016-4843-3 [20] Shi H,Zhu L,Ma J,et al. The accuracy of a novel pedicle screw insertion technique assisted by a special angular scale in the subaxial cervical spine using lateral mass as a reference marker[J]. J Orthop Surg Res,2020,15(1):551. doi: 10.1186/s13018-020-02054-1 [21] Rajasekaran S,Kanna P R,Shetty A P. Safety of cervical pedicle screw insertion in children: A clinicoradiological evaluation of computer-assisted insertion of 51 cervical pedicle screws including 28 subaxial pedicle screws in 16 children[J]. Spine (Phila Pa,1976,),2012,37(4):E216-E223. [22] Takahata M,Yamada K,Akira I,et al. A novel technique of cervical pedicle screw placement with a pilot screw under the guidance of intraoperative 3D imaging from C-arm cone-beam CT without navigation for safe and accurate insertion[J]. Eur Spine J,2018,27(11):2754-2762. doi: 10.1007/s00586-018-5706-x [23] Chachan S,Bin Abd Razak H R,Loo W L,et al. Cervical pedicle screw instrumentation is more reliable with O-arm-based 3D navigation: Analysis of cervical pedicle screw placement accuracy with O-arm-based 3D navigation[J]. Eur Spine J,2018,27(11):2729-2736. doi: 10.1007/s00586-018-5585-1 [24] Fujita R,Oda I,Takeuchi H,et al. Accuracy of pedicle screw placement using patient-specific template guide system[J]. Orthop Sci,2022,27(2):348-354. doi: 10.1016/j.jos.2021.01.007 [25] Kisinde S,Hu X,Hesselbacher S,et al. Robotic-guided placement of cervical pedicle screws: Feasibility and accuracy[J]. Eur Spine J,2022,31(3):693-701. doi: 10.1007/s00586-022-07110-4 [26] Ishikawa Y,Kanemura T,Yoshida G,et al. Clinical accuracy of three-dimensional fluoroscopy-based computer-assisted cervical pedicle screw placement: A retrospective comparative study of conventional versus computer-assisted cervical pedicle screw placement[J]. Neurosurg Spine,2010,13(5):606-611. doi: 10.3171/2010.5.SPINE09993 [27] Liu Y J,Tian W,Liu B,et al. Comparison of the clinical accuracy of cervical (C2-C7) pedicle screw insertion assisted by fluoroscopy,computed tomography-based navigation,and intraoperative three-dimensional C-arm navigation[J]. Chin Med J (Engl),2010,123(21):2995-2998. [28] Nakashima H,Yukawa Y,Imagama S,et al. Complications of cervical pedicle screw fixation for nontraumatic lesions: A multicenter study of 84 patients[J]. Neurosurg Spine,2012,16(3):238-247. doi: 10.3171/2011.11.SPINE11102 [29] Yoshii T,Hirai T,Sakai K,et al. Cervical pedicle screw placement using intraoperative computed tomography imaging with a mobile scanner gantry[J]. Eur Spine J,2016,25(6):1690-1697. doi: 10.1007/s00586-016-4508-2 -

 下载:
下载:
 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 1186
- HTML全文浏览量: 707
- PDF下载量: 22
- 被引次数: 0
