

Construction of A 28-day Mortality Risk Prediction Model in Patients with Acute Left Heart Failure Complicated by Respiratory Failure Based on Serum HIF-1α and CysC
-
摘要:
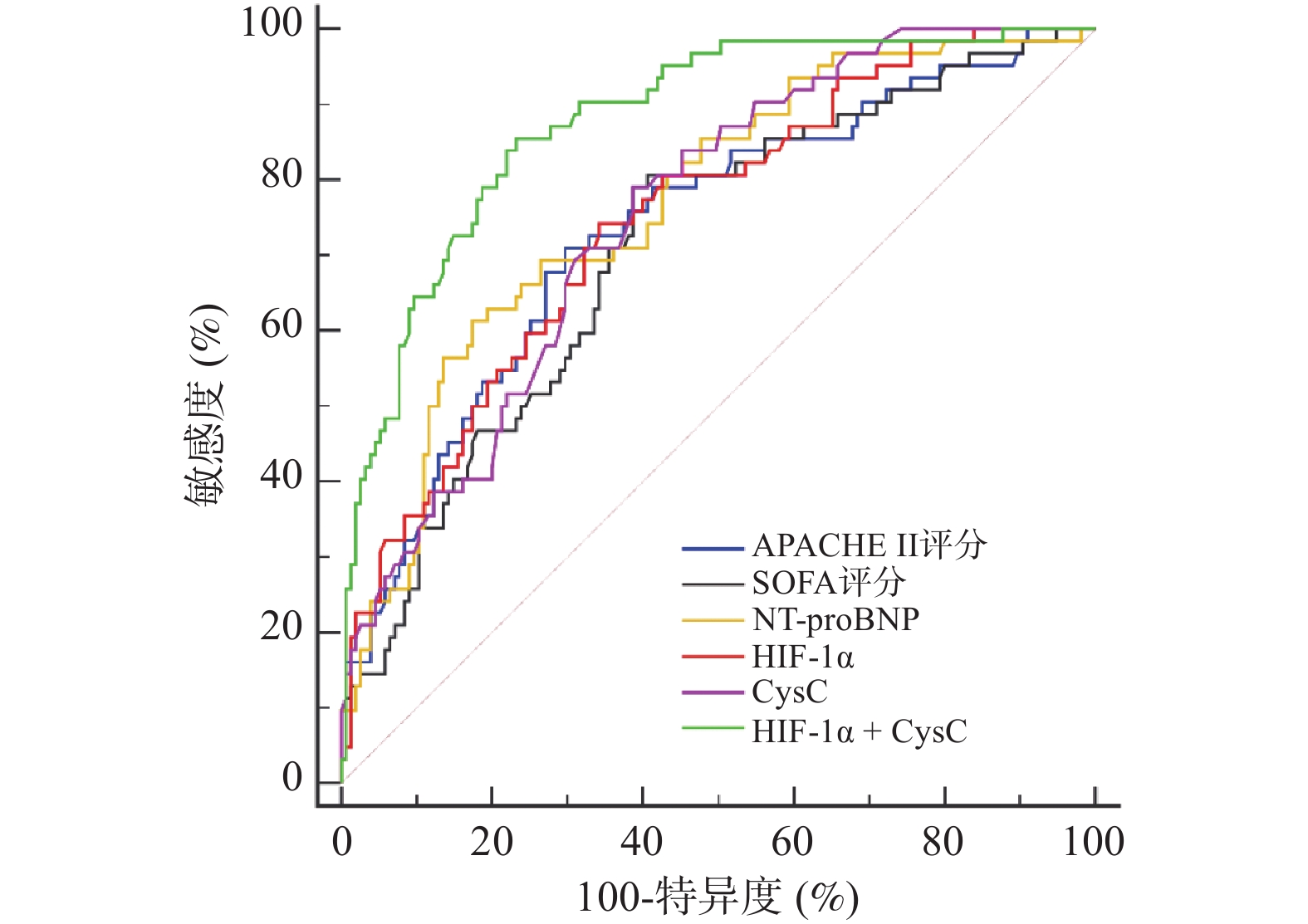
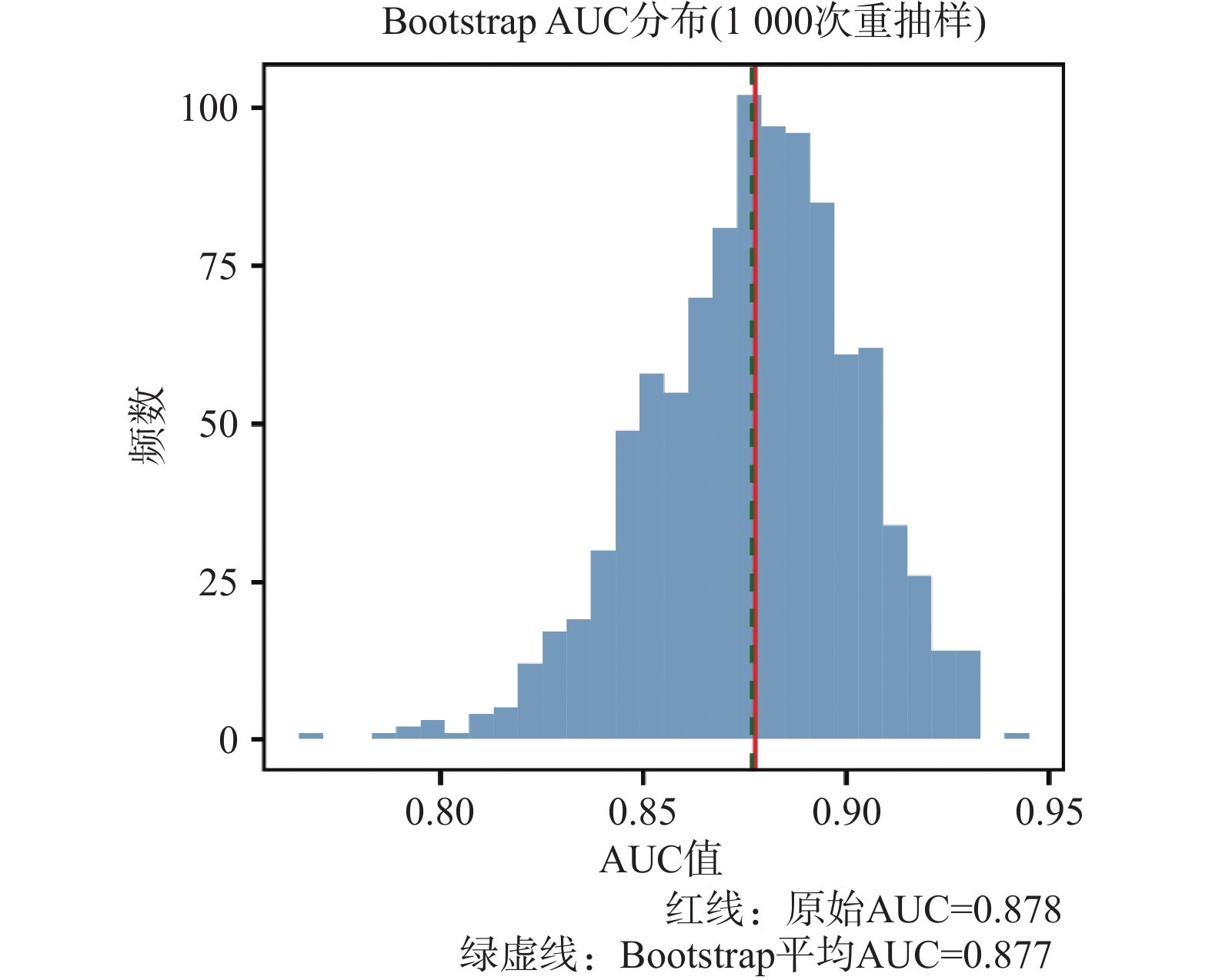
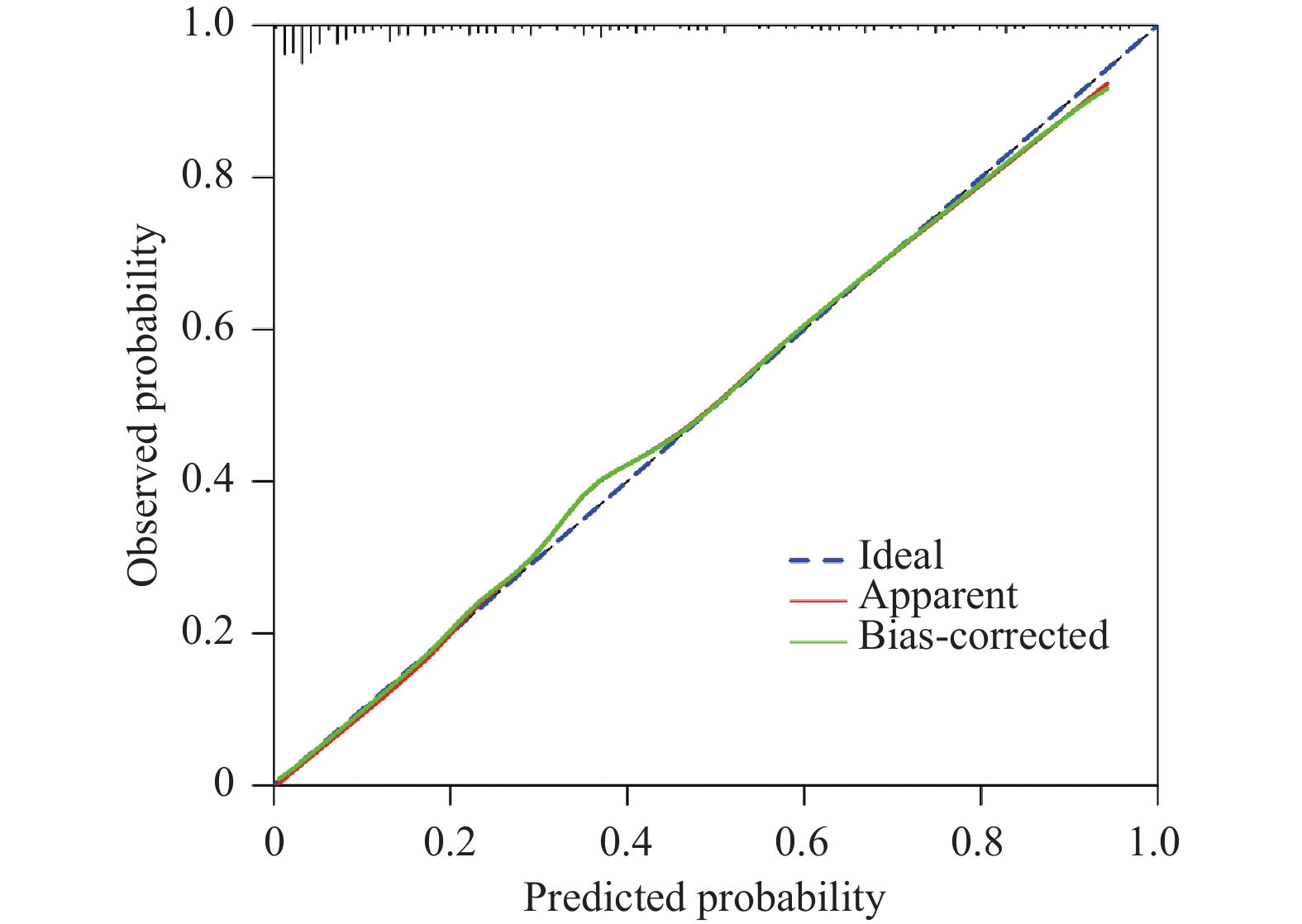
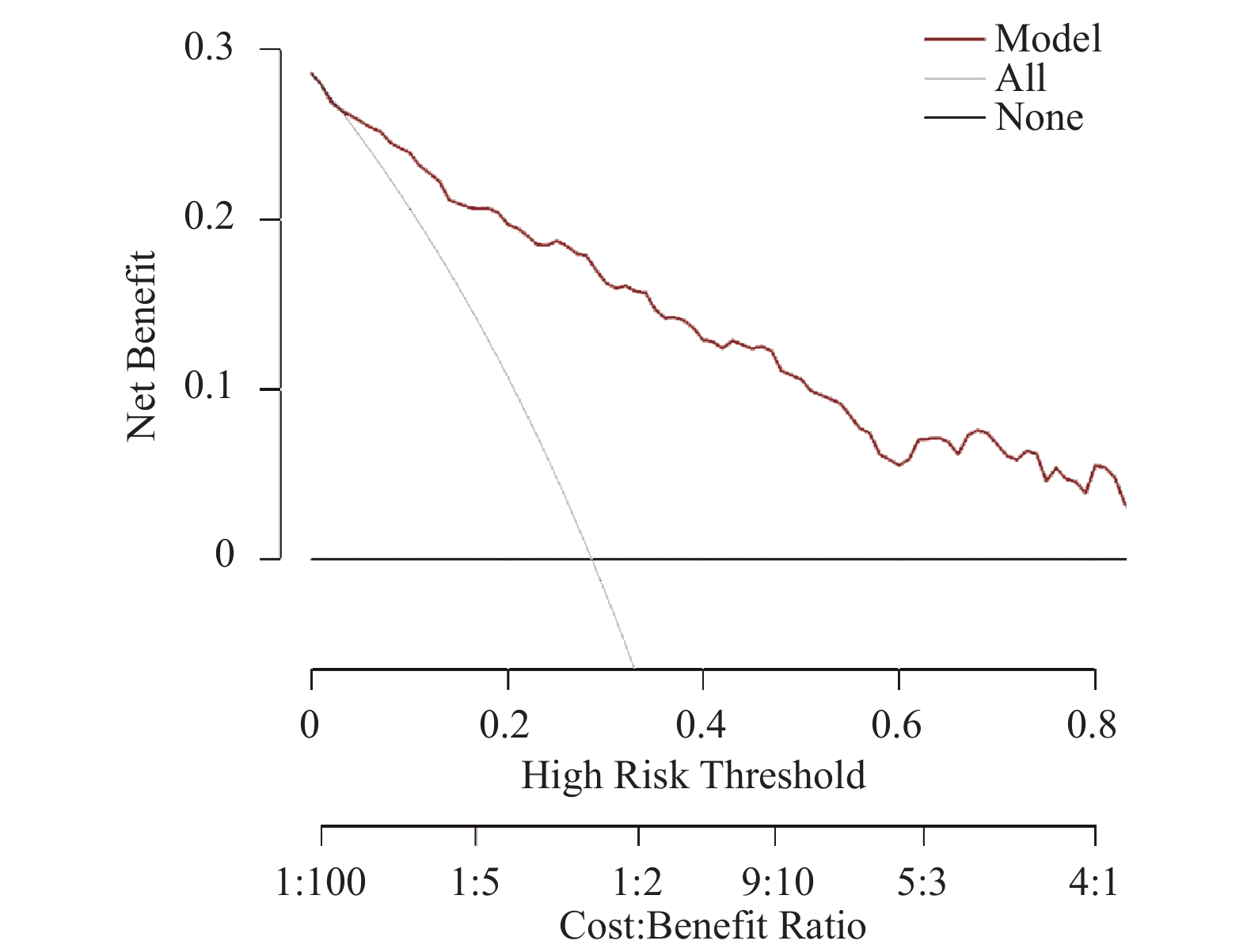
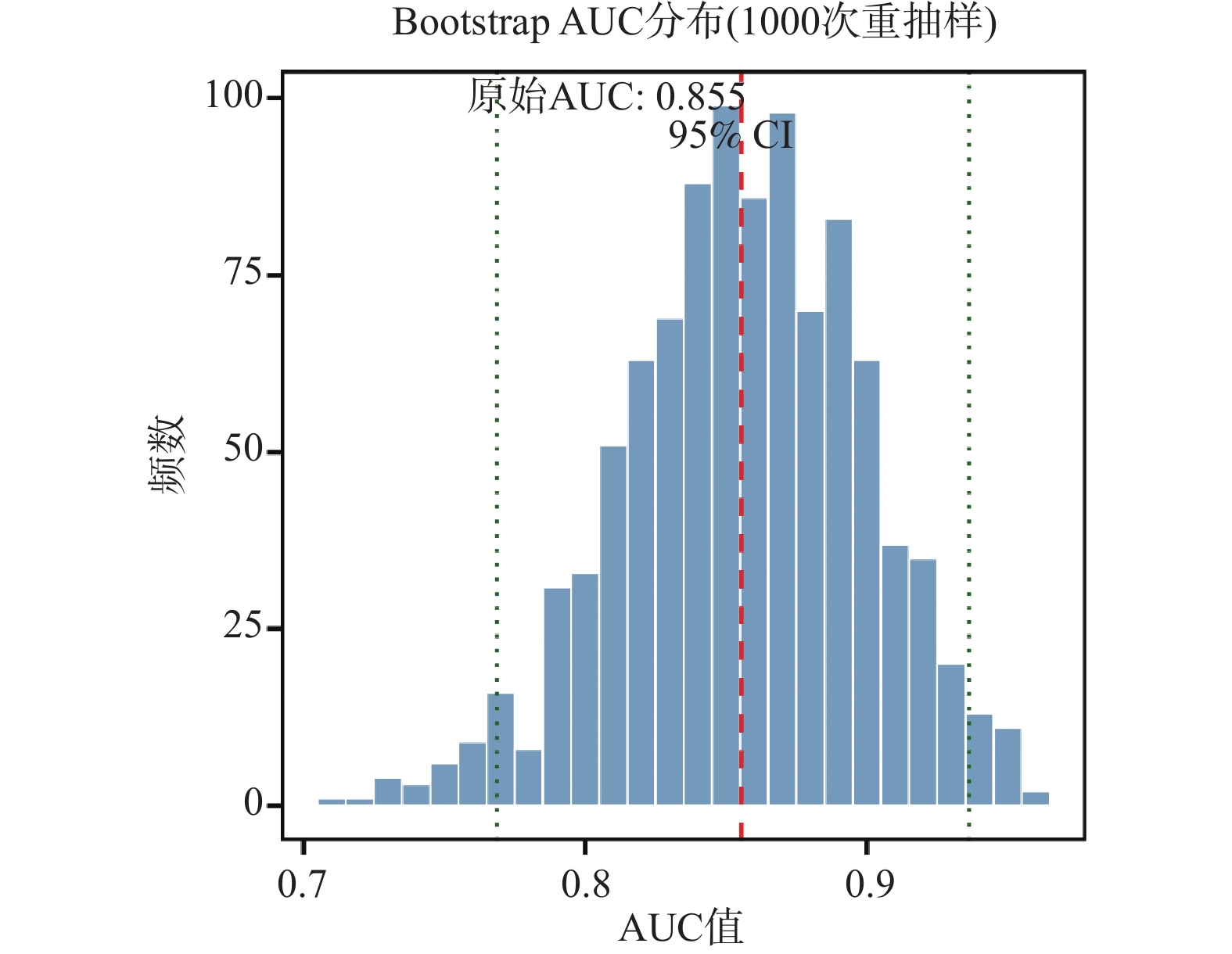
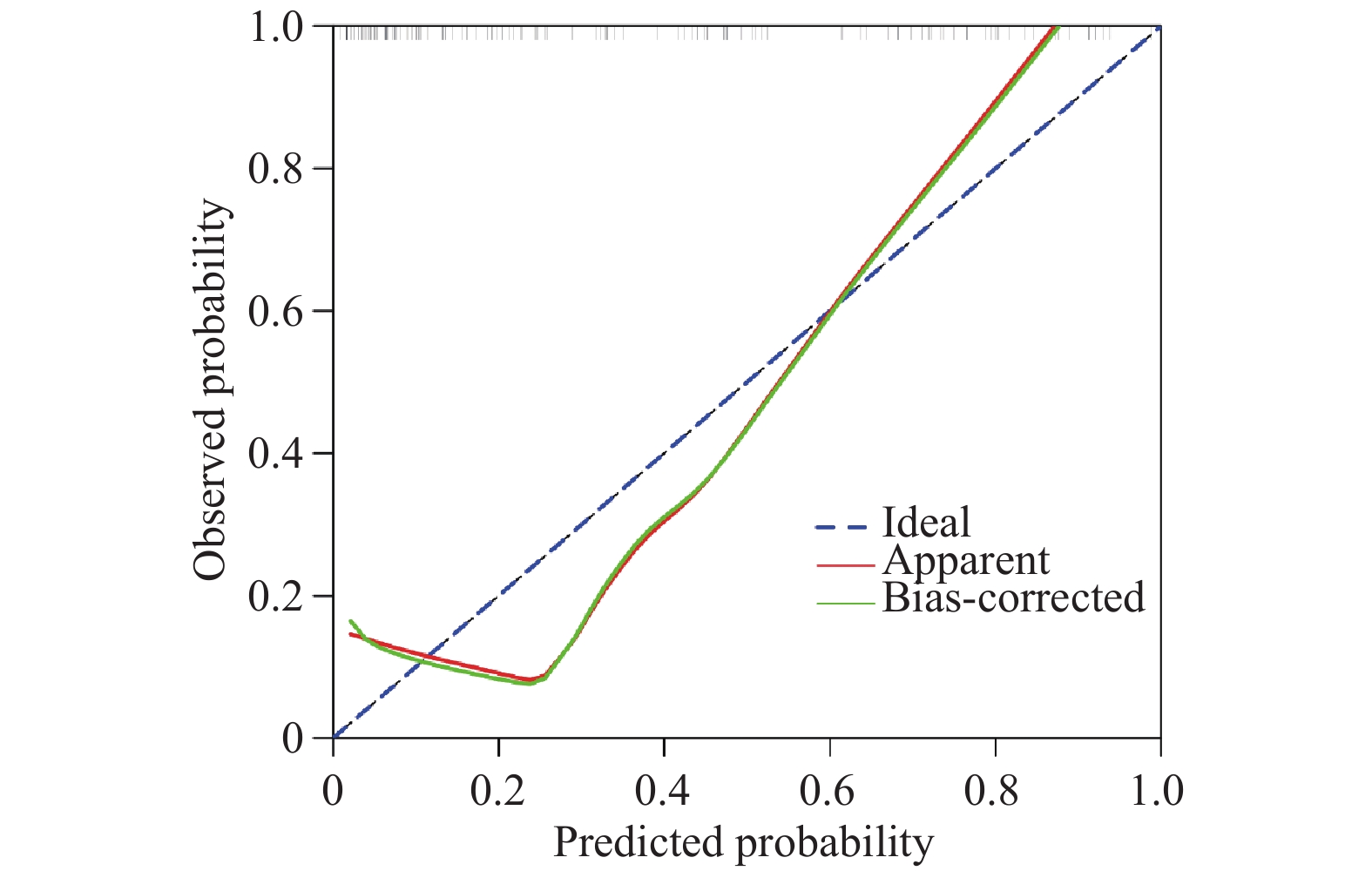
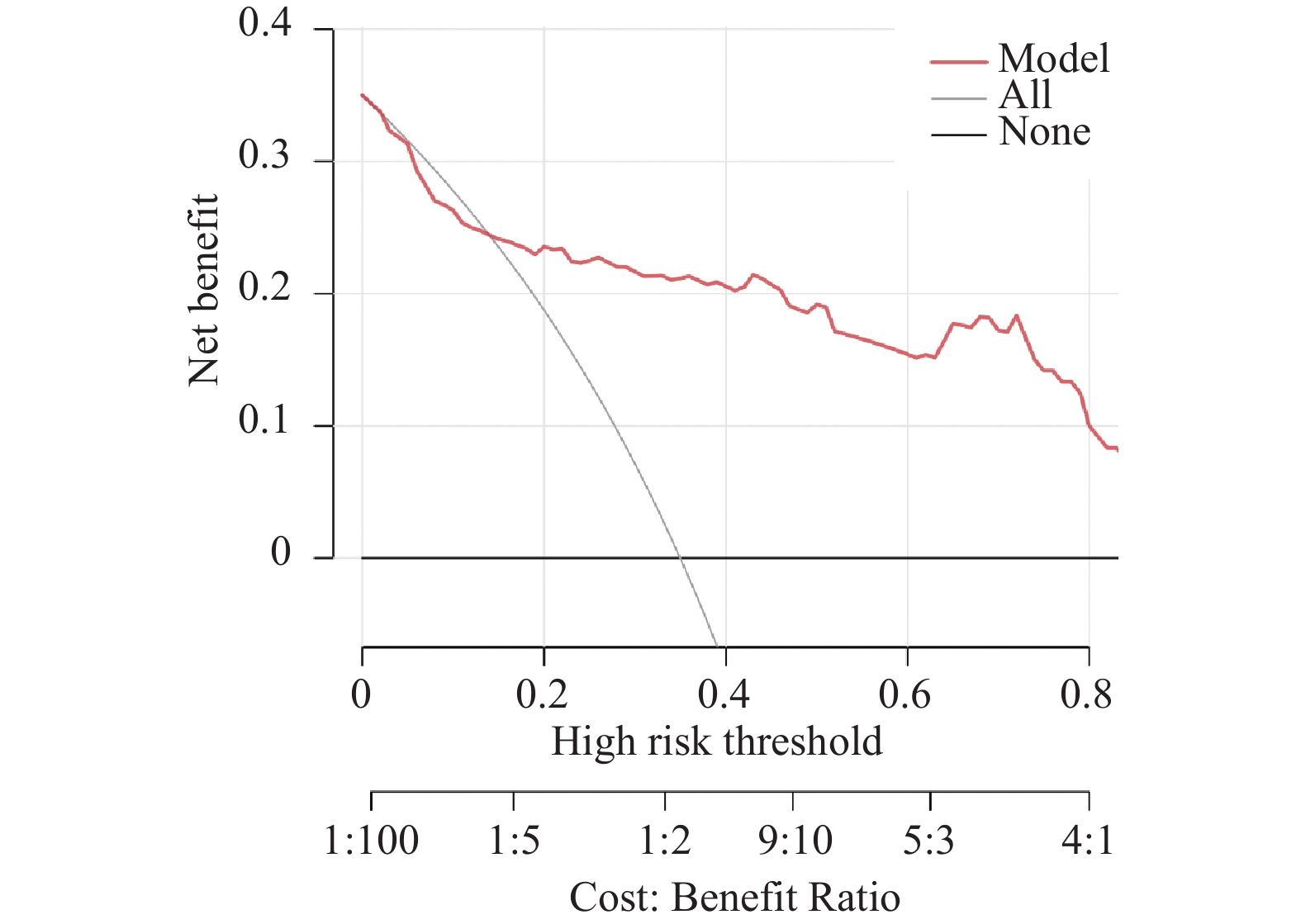
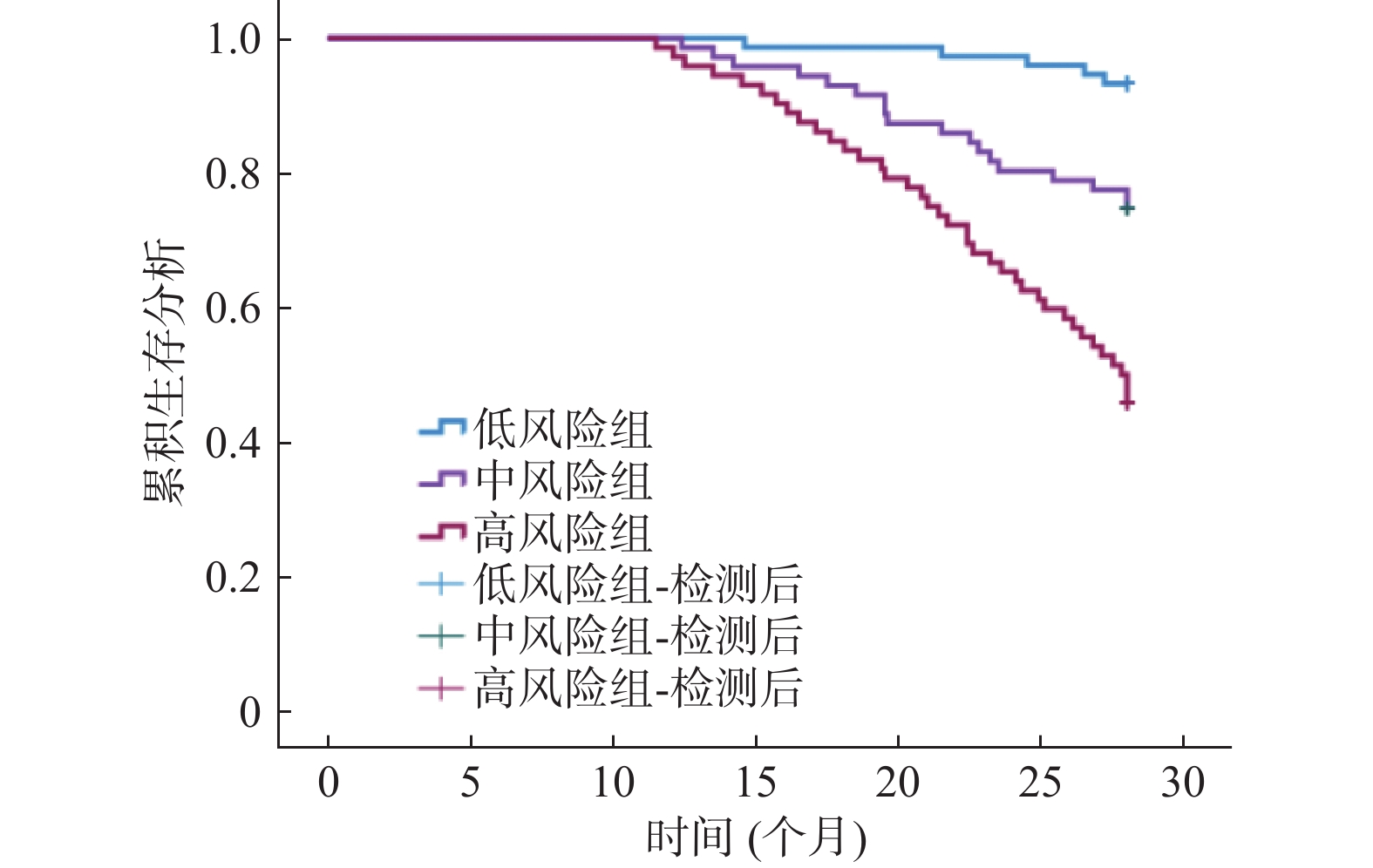
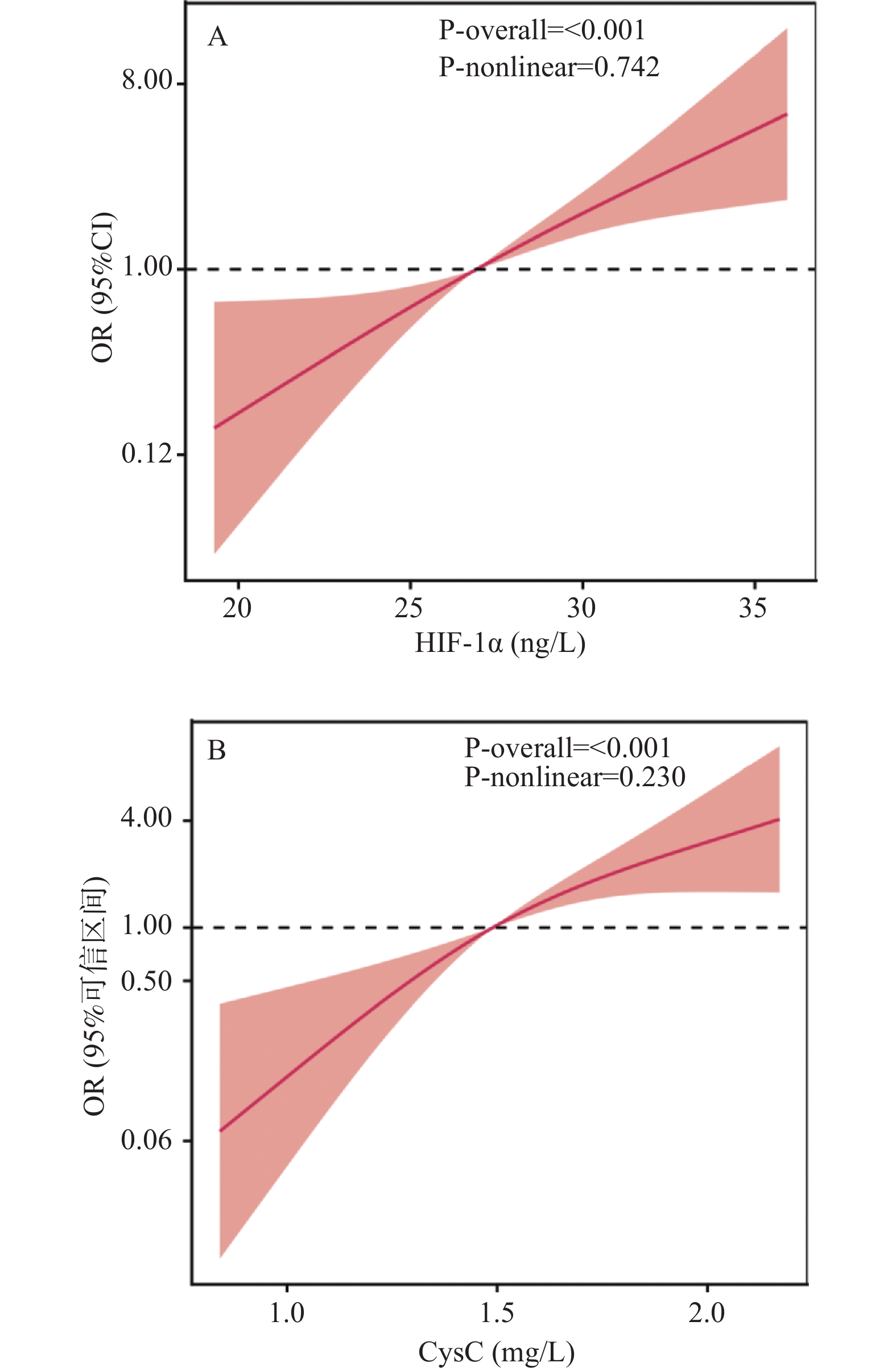
目的 探究急性左心衰(acute left heart failure,AHF)并发呼吸衰竭(respiratory failure,RF)患者血清缺氧诱导因子-1α(hypoxia-inducible factor-1alpha,HIF-1α)、胱抑素C(Cystatin C,CysC)水平预测28 d死亡风险的价值。 方法 回顾性分析2022年1月至2024年12月株洲市中心医院收治的217例AHF伴RF患者的临床资料,根据患者出院28 d生存情况分组,其中死亡组(n = 62)与存活组(n = 155)。比较两组患者一般资料及血清HIF-1α、CysC水平,分析AHF伴RF患者28 d死亡风险影响因素及血清HIF-1α、CysC水平与28 d死亡风险的关系,采用受试者工作特征(receiver operating characteristic,ROC)曲线评价AHF伴RF患者HIF-1α、CysC对28 d死亡风险的预测价值,并基于联合预测模型的进行风险分层与临床验证。 结果 死亡组急性生理学与慢性健康状 况评分Ⅱ(acute physiology and chronic health evaluation Ⅱ , APACHEⅡ)评分、序贯性脏器衰竭评价评分(sequential organ failure assessment ,SOFA)评分、N 端 B 型脑钠肽前体(n-terminal pro-b-type natriuretic peptide ,NT-proBNP)、HIF-1α、 CysC均高于存活组(P < 0.05); Logistic 回归显示 HIF-1α、CysC均为AHF 伴 RF 患者 28 d 死亡风险独立影响 因素(P < 0.05); 限制性立方样条(restricted cubic spline ,RCS)模型分析显示, 调整其他变量后, 血清 HIF-1α、 CysC 水平仍与 AHF 伴 RF 患者 28 d 死亡风险呈线性正相关(P < 0.05), 随血清 HIF-1α、CysC 升高, AHF 伴 RF 患者的死亡风险逐渐增加; ROC 曲线显示, APACHE II 评分、SOFA 评分、 NT-proBNP、HIF-1α、CysC 预 测 AHF 伴 RF 患者 28 d 死亡风险的曲线下面积(area under curve,AUC)分别为0.737、 0.711、 0.768、 0.748、 0.753, 各指标单独预测 AUC 比较差异无统计学意义(P > 0.05); 交互作用分析 RERI = 1.09、 AP = 0.253、SI = 2.727 ,HIF-1α 与 CysC 两者同时升高时,对 28 d 死亡风险存在正向相加交互作用, 即联合效应大于各自单独效应之和;血清 HIF-1α、 CysC 联合预测 AHF 伴 RF 患者 28 d 死亡风险的 AUC 为 0.878, 明显大于 APACHE II 评分、SOFA 评分、 NT- proBNP、HIF-1α、CysC 单独预测的 AUC(P < 0.05); 绘制校准曲线显示, 预测风险与实际观察风险在整个风 险范围内具有良好的一致性(Hosmer-Lemeshow 检验,χ2 = 2.224 ,P = 0.086);通过 Bootstrap 法(1 000 次重抽样) 进行内部验证, 校正后模型的 AUC 为 0.877,且校准曲线显示预测风险与实际风险一致 性良好。DCA 表明在 0.2~0.8 阈值概率范围内, 使用该模型具有临床净获益, 且时间验证集显示,模型具有较 高的稳健性和较高的预测效能。基于联合预测模型将患者分为低、中、高风险组, 三组 28 d 实际死亡率分别 为 4.17%、27.40%、54.17%(P < 0.05)。 结论 AHF伴RF患者血清HIF-1α、CysC水平与28 d死亡风险密切相关,基于二者构建的联合预测模型具有良好的区分能力。 Abstract:Objective To explore the predictive value of serum hypoxia-inducible factor-1alpha (HIF-1α) and Cystatin C (CysC) levels for 28-day mortality risk in patients with acute left heart failure (AHF) complicated with respiratory failure (RF). Methods A retrospective analysis was conducted on clinical data from 217 AHF patients with concurrent RF admitted between January 2022 and December 2024. Patients were stratified based on 28-day survival status post-discharge into a mortality group (n = 62) and a survival group (n = 155). General demographic data and serum HIF-1α and CysC levels were compared between the two groups. The influencing factors for 28-day mortality risk in AHF patients with RF and the relationship between serum HIF-1α, CysC levels and 28-day mortality risk were analyzed. Receiver operating characteristic (ROC) curves were used to evaluate the predictive value of HIF-1α and CysC for 28-day mortality risk in AHF with RF patients. Risk stratification and clinical validation were performed based on a combined predictive model. Results The mortality group demonstrated significantly higher Acute Physiology and Chronic Health Evaluation II (APACHE II) scores (16.59±3.05 vs 13.72±2.47, t = 7.214, P < 0.001), Sequential Organ Failure Assessment (SOFA) scores(12.61±2.24 vs 11.89±2.15, t = 2.202, P = 0.029), N-terminal pro-B-type natriuretic peptide (NT-proBNP) (507.41±82.44 vs 329.49±70.55 pg/mL, t = 15.975, P < 0.001), HIF-1α (30.14±4.58 vs 21.37±3.82 ng/L, t = 14.410, P < 0.001) and CysC (1.72±0.35 vs 1.30±0.28 mg/L, t = 9.270, P < 0.001) compared with the survival group. Logistic regression analysis showed that HIF-1α (OR = 1.315, 95%CI: 1.129-1.532) and CysC (OR = 1.260, 95%CI: 1.105-1.437) were independent influencing factors for 28 day mortality risk in AHF with RF patients (P < 0.05). Restricted cubic spline (RCS) model analysis demonstrated that after adjusting for other variables, serum HIF-1α and CysC levels remained linearly and positively correlated with 28 day mortality risk in AHF with RF patients (P < 0.05), with mortality risk progressively increasing as serum HIF-1α and CysC levels elevated. ROC curve analysis revealed that the area under the curve (AUC) for predicting 28-day mortality risk were as follows: APACHE II score 0.737 (95% CI: 0.673–0.794), SOFA score 0.711 (0.646–0.771), NT-proBNP 0.768 (0.706–0.822), HIF-1α 0.748 (0.684–0.804), and CysC 0.753 (0.690–0.809), with no statistically significant differences in AUC between individual indicators (P>0.05). Interaction analysis revealed RERI=1.09, AP=0.253, and SI=2.727, indicating a positive additive interaction between HIF-1α and CysC when both were simultaneously elevated, with the combined effect exceeding the sum of individual effects. The combined predictive AUC for serum HIF-1α and CysC for 28-day mortality risk in AHF with RF patients was 0.878, significantly higher than the individual AUCs for APACHE II score, SOFA score, NT-proBNP, HIF-1α, and CysC (P < 0.05). Calibration curves demonstrated good concordance between predicted and observed risk across the entire risk spectrum(Hosmer-Lemeshow test, χ2=2.224, P = 0.086). Internal validation via Bootstrap resampling ( 1000 iterations) yielded a corrected model AUC of 0.877 (95% CI: 0.828–0.927), with calibration curves demonstrating good agreement between predicted and actual risk. Decision curve analysis (DCA) indicated clinical net benefit within the threshold probability range of 0.2–0.8, and temporal validation demonstrated high model robustness and predictive performance. Patients stratified into low, intermediate, and high-risk groups based on the combined predictive model had actual 28-day mortality rates of 4.17%, 27.40%, and 54.17%, respectively (P<0.05).Conclusion Serum HIF-1α and CysC levels in AHF patients with concurrent RF are closely associated with 28-day mortality risk. A combined predictive model constructed from these two markers demonstrates excellent discriminative ability. -
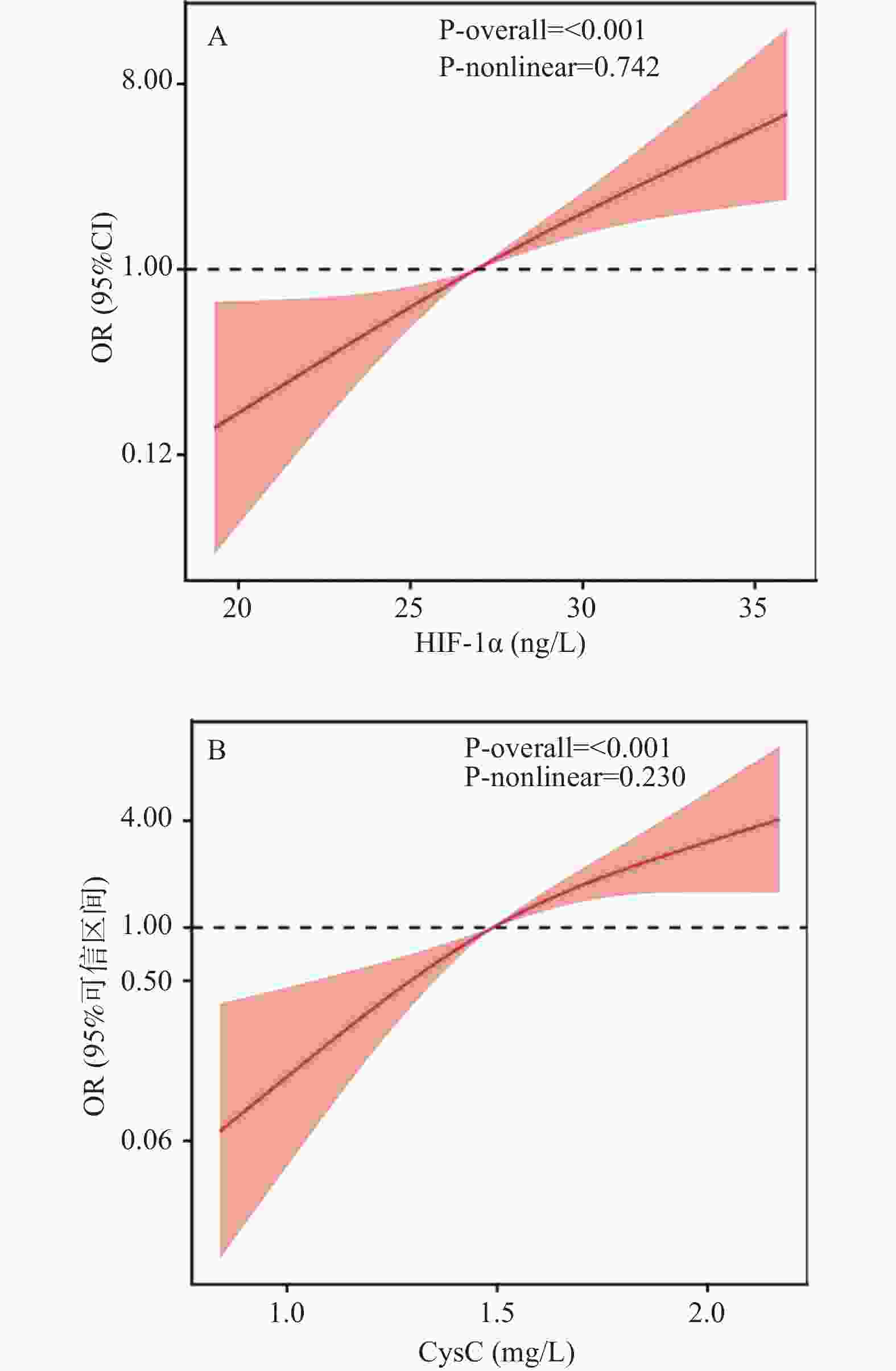
图 1 血清HIF-1α、CysC水平与AHF伴RF患者28 d死亡风险的关系
A:HIF-1α与AHF伴RF患者28 d死亡风险的关系;B:CysC与AHF伴RF患者28 d死亡风险的关系。
Figure 1. Correlation between serum HIF-1α,CysC levels and 28-day mortality risk in AHF patients with RF
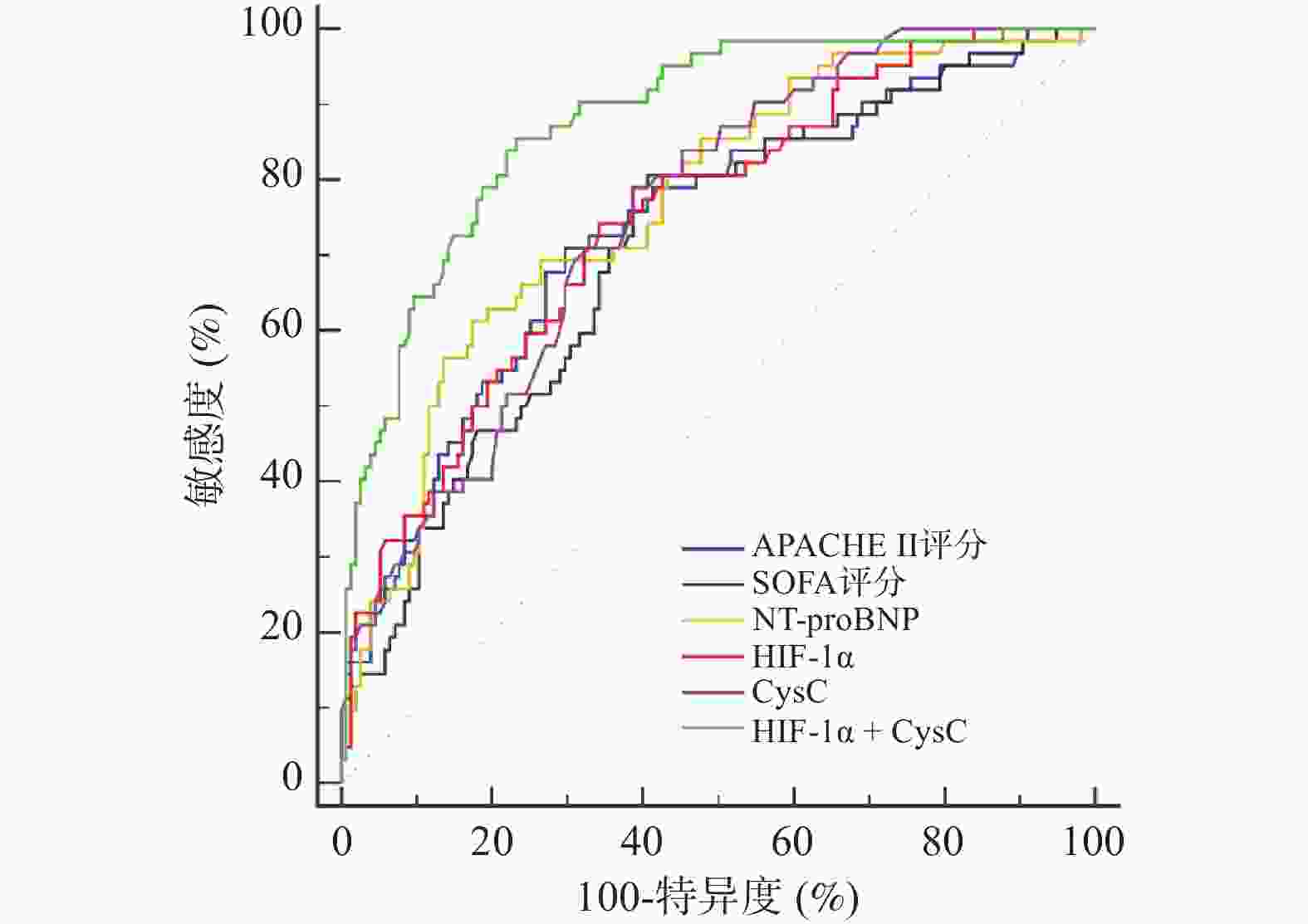
图 2 APACHE II评分、SOFA评分、NT-proBNP、HIF-1α、CysC预测AHF伴RF患者28 d死亡风险的ROC曲线
Figure 2. ROC curves of APACHE II score,SOFA score,NT-proBNP,HIF-1α and CysC for predicting 28-day mortality risk in AHF patients with RF
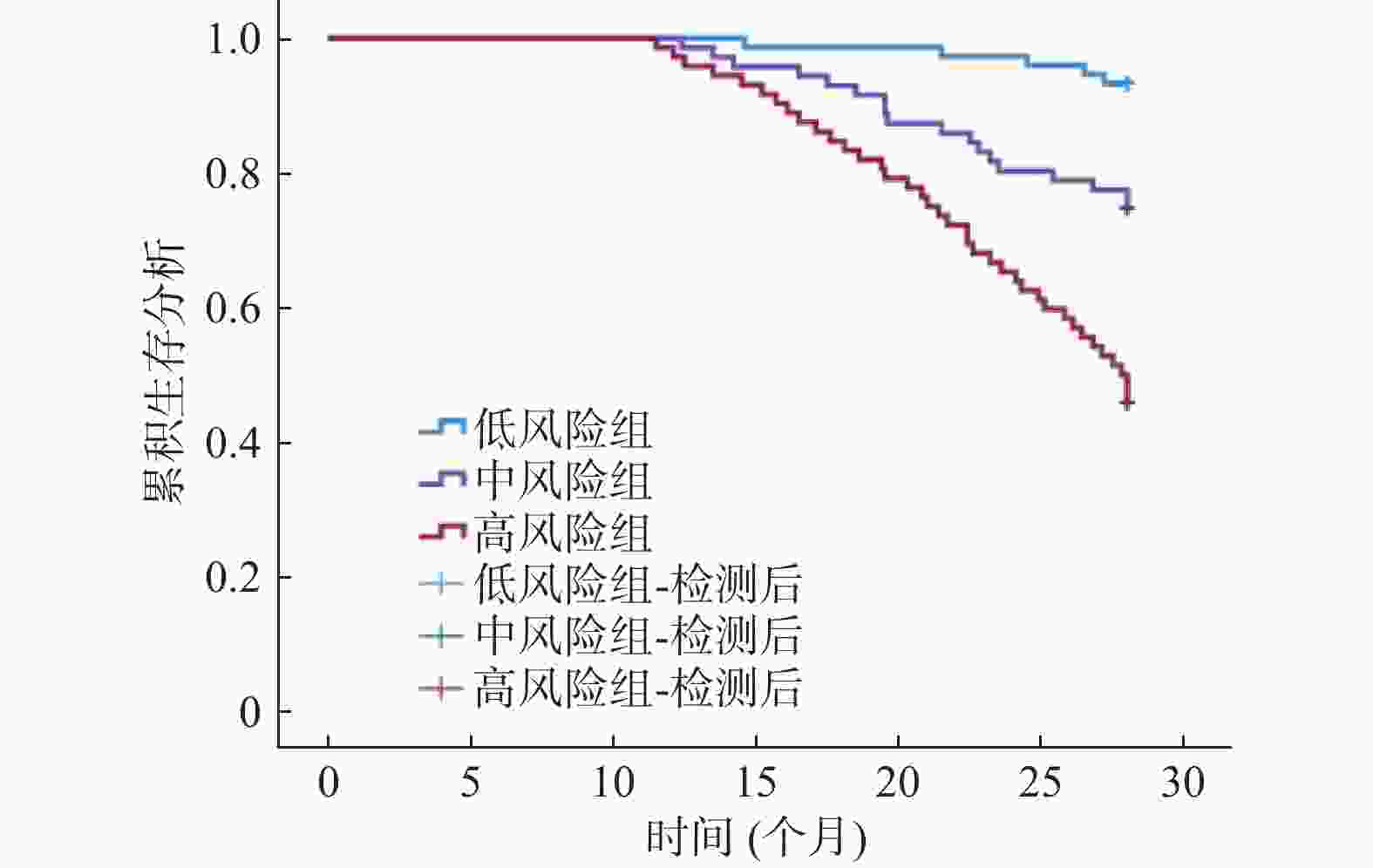
图 9 基于联合预测模型风险分组的患者生存曲线
Figure 9. Patient survival curves based on risk stratification from the combined prediction model
表 1 两组一般资料及血清HIF-1α、CysC水平比较[n(%)/($ \bar x \pm s $)]
Table 1. Comparison of general data and serum HIF-1α,CysC levels between two groups [n(%)/($ \bar x \pm s $)]
项目 死亡组(n = 62) 存活组(n = 155) t/χ2 P 性别 0.017 0.897 男 33(53.23) 84(54.19) 女 29(46.77) 71(45.81) 年龄(岁) 61.42 ± 6.83 59.57 ± 7.22 1.731 0.085 体重指数(kg/m2) 21.57 ± 2.43 21.33 ± 2.50 0.644 0.520 基础疾病 高血压 13(20.97) 26(16.77) 0.528 0.467 糖尿病 11(17.74) 20(12.90) 0.847 0.357 冠心病 7(11.29) 14(9.03) 0.258 0.611 高脂血症 11(17.74) 22(14.19) 0.432 0.511 心功能分级 3.617 0.057 Ⅲ级 45(72.58) 130(83.87) Ⅳ级 17(27.42) 25(16.13) 呼吸衰竭类型 0.185 0.667 Ⅰ型 32(51.61) 85(54.84) Ⅱ型 30(48.39) 70(45.16) 生命体征 心率(次/min) 119.25 ± 10.31 117.12 ± 9.82 1.423 0.156 舒张压(mmHg) 94.32 ± 9.17 92.14 ± 10.25 1.457 0.147 收缩压(mmHg) 142.83 ± 15.06 140.29 ± 12.88 1.249 0.213 呼吸频率(次/min) 36.24 ± 2.83 35.72 ± 2.77 1.242 0.216 动脉血气 pH 7.11 ± 0.52 7.20 ± 0.45 1.272 0.205 PaO2(mmHg) 54.78 ± 2.11 55.12 ± 2.28 1.013 0.312 PaCO2(mmHg) 67.06 ± 11.03 65.29 ± 10.84 1.081 0.281 病情评分(分) APACHE II评分 16.59 ± 3.05 13.72 ± 2.47 7.214 <0.001* SOFA评分 12.61 ± 2.24 11.89 ± 2.15 2.202 0.029* 发病至机械通气时间(h) 5.527 0.019* ≤2 35(56.45) 113(72.90) >2 27(43.55) 42(27.10) 血清指标 CRP(mg/L) 22.74 ± 5.69 21.41 ± 7.35 1.279 0.202 PCT(ng/mL) 3.84 ± 0.67 3.78 ± 0.62 0.629 0.530 NT-proBNP(pg/mL) 507.41 ± 82.44 329.49 ± 70.55 15.975 <0.001* HIF-1α(ng/L) 30.14 ± 4.58 21.37 ± 3.82 14.410 <0.001* CysC(mg/L) 1.72 ± 0.35 1.30 ± 0.28 9.270 <0.001* LVEF(%) 33.57 ± 3.47 36.86 ± 3.77 5.938 <0.001* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 AHF伴RF患者28 d死亡风险的多因素Logistic回归分析
Table 2. Multivariate Logistic regression analysis of 28-day mortality risk in AHF patients with RF
因素 赋值 β S.E. Waldχ2 OR 95%CI P 模型1 常数项 — 1.987 0.107 22.833 — — <0.001* APACHE II评分 原值带入 0.389 0.112 12.083 1.476 1.079~2.019 <0.001* SOFA评分 原值带入 0.414 0.125 10.952 1.512 1.154~1.982 <0.001* 发病至机械通气时间(h) ≤2=1,>2=2 1.408 0.362 15.134 4.089 2.749~6.082 <0.001* NT-proBNP 原值带入 0.469 0.121 15.018 1.598 1.254~2.037 <0.001* HIF-1α 原值带入 0.463 0.140 10.931 1.589 1.191~2.119 <0.001* CysC 原值带入 0.452 0.116 15.191 1.572 1.179~2.095 <0.001* 模型2 常数项 — 1.325 0.084 17.241 — — <0.001* HIF-1α 原值带入 0.274 0.102 7.214 1.315 1.129~1.532 <0.001* CysC 原值带入 0.231 0.074 9.762 1.260 1.105~1.437 <0.001* 模型1为校正APACHE II评分、SOFA评分、发病至机械通气时间前,模型2为校正APACHE II评分、SOFA评分、发病至机械通气时间后;—表示无数据;*P < 0.05。
下载: 导出CSV
表 3 APACHE II评分、SOFA评分、NT-proBNP、HIF-1α、CysC对AHF伴RF患者28 d死亡风险的预测价值
Table 3. Predictive value of APACHE II score,SOFA score,NT-proBNP,HIF-1α and CysC for 28-day mortality risk in AHF patients with RF
项目 AUC 95%CI 截断值 P 特异度(%) 敏感度(%) 约登指数 APACHE II评分 0.737 0.673~0.794 14.35分 <0.001* 70.32 70.97 0.413 SOFA评分 0.711 0.646~0.771 11.16分 <0.001* 61.29 79.03 0.403 NT-proBNP 0.768 0.706~0.822 510.53 pg/mL <0.001* 82.58 61.29 0.439 HIF-1α 0.748 0.684~0.804 27.51 ng/L <0.001* 70.81 74.19 0.400 CysC 0.753 0.690~0.809 1.48 mg/L <0.001* 71.61 79.03 0.403 HIF-1α+CysC 0.878 0.826~0.918 0.623 <0.001* 76.77 85.48 0.623 *P < 0.05。
下载: 导出CSV
表 4 HIF-1α、CysC对AHF伴RF患者28 d死亡风险的交互作用
Table 4. Interactive effect of HIF-1α and CysC on 28-day mortality risk in AHF patients with RF
HIF-1α CysC 28 d结局 OR(95%CI) RERI AP SI 死亡 生存 低水平 低水平 10 43 1 1.09 0.253 2.727 低水平 高水平 16 48 1.43(0.59~3.48) 高水平 低水平 19 46 1.78(0.74~4.27) 高水平 高水平 18 18 4.30(1.66~11.13)
下载: 导出CSV
-
[1] Del Buono M G, Moroni F, Montone R A, et al. Ischemic cardiomyopathy and heart failure after acute myocardial infarction[J]. Curr Cardiol Rep, 2022, 24(10): 1505-1515. doi: 10.1007/s11886-022-01766-6 [2] 闻晓霞. 呼吸机辅助时机对急性左心衰伴呼吸衰竭患者预后及心肺功能的影响[J]. 吉林医学, 2023, 44(2): 393-396. doi: 10.3969/j.issn.1004-0412.2023.02.032 [3] Henneges C, Morbach C, et al. Sex-specific bimodal clustering of left ventricular ejection fraction in patients with acute heart failure[J]. ESC Heart Fail, 2022, 9(1): 786-790. doi: 10.1002/ehf2.13618 [4] Xu M, Warner C, Duan X, et al. HIV coinfection exacerbates HBV-induced liver fibrogenesis through a HIF-1α- and TGF-β1-dependent pathway[J]. J Hepatol, 2024, 80(6): 868-881. doi: 10.1016/j.jhep.2024.01.026 [5] Sato T, Takeda N. The roles of HIF-1α signaling in cardiovascular diseases[J]. J Cardiol, 2023, 81(2): 202-208. doi: 10.1016/j.jjcc.2022.09.002 [6] Liu Z, Zheng X, Li N, et al. Baicalein suppresses inflammation and attenuates acute lung injury by inhibiting glycolysis via HIF-1α signaling[J]. Mol Med Rep, 2024, 31: 18. doi: 10.3892/mmr.2024.13383 [7] Nagy E E, Puskás A, Kelemen P, et al. Elevated serum cystatin C and decreased cathepsin S/cystatin C ratio are associated with severe peripheral arterial disease and polyvascular involvement[J]. Diagnostics, 2022, 12(4): 833. doi: 10.3390/diagnostics12040833 [8] Saito T, Arashi H, Yamaguchi J, et al. Elevated cystatin-C levels are associated with increased mortality in acute coronary syndrome patients: An HIJ-PROPER sub-analysis[J]. Cardiorenal Med, 2022, 12(1): 20-28. doi: 10.1159/000522412 [9] Ider M, Ok M, Naseri A, et al. Acute kidney injury is associated with higher serum cys-C and NGAL concentrations, and risk of mortality in premature calves with respiratory distress syndrome[J]. Animals, 2023, 13(2): 232. doi: 10.3390/ani13020232 [10] 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 急性心力衰竭诊断和治疗指南(2010)[J]. 中国实用乡村医生杂志, 2013, 20(12): 3-8. [11] 中国医疗保健国际交流促进会循证医学分会, 海峡两岸医药卫生交流协会老年医学专业委员会. 心力衰竭生物标志物中国专家共识[J]. 中华检验医学杂志, 2020, 43(2): 130-141. doi: 10.3760/cma.j.issn.1009-9158.2020.02.007 [12] Laczynski D J, Gallop J, Sicard G A, et al. Benchmarking a center of excellence in vascular surgery: Using acute physiology and chronic health evaluation II to validate outcomes in a tertiary care institute[J]. Vasc Endovascular Surg, 2023, 57(8): 856-862. doi: 10.1177/15385744231183744 [13] Fleiss N, Polin R A. Sequential organ failure assessment scores to predict outcomes: From adults to neonates[J]. Curr Opin Pediatr, 2023, 35(2): 218-222. doi: 10.1097/MOP.0000000000001207 [14] Palazzuoli A, Cartocci A, Pirrotta F, et al. Different right ventricular dysfunction and pulmonary coupling in acute heart failure according to the left ventricular ejection fraction[J]. Prog Cardiovasc Dis, 2023, 81: 89-97. doi: 10.1016/j.pcad.2023.07.008 [15] 李玲, 张乙川, 刘珂良, 等. HIF-1α与食管癌患者内镜黏膜下剥离术后血管新生及预后的关系[J]. 现代消化及介入诊疗, 2024, 29(4): 465-469. [16] Xu L, Yang M, Wei A, et al. Aerobic exercise-induced HIF-1α upregulation in heart failure: Exploring potential impacts on MCT1 and MPC1 regulation[J]. Mol Med, 2024, 30(1): 83. doi: 10.1186/s10020-024-00854-3 [17] Li Z L, Ding L, Ma R X, et al. Activation of HIF-1α C-terminal transactivation domain protects against hypoxia-induced kidney injury through hexokinase 2-mediated mitophagy[J]. Cell Death Dis, 2023, 14: 339. doi: 10.1038/s41419-023-05854-5 [18] Zhao H, Yang M, Han Y, et al. HIF-1α/BNIP3-mediated endoplasmic reticulum degradation via autophagy protects against ischemia reperfusion-induced acute kidney injury[J]. Antioxid Redox Signal, 2025, 42(4-6): 212-227. doi: 10.1089/ars.2023.0467 [19] 吴倩, 杨娟, 孙斌. 血清ET-1、NT-proBNP、HIF-1α水平与急性左心衰竭患者预后的相关性[J]. 川北医学院学报, 2024, 39(8): 1064-1067. [20] 刘华伟. 血清HIF-1α、SP-D、Copeptin水平联合检测预测慢性阻塞性肺疾病合并Ⅱ型呼吸衰竭患者预后的价值[J]. 中国民康医学, 2024, 36(13): 132-135. doi: 10.3969/j.issn.1672-0369.2024.13.039 [21] Fu E L, Levey A S, Coresh J, et al. Accuracy of GFR estimating equations based on creatinine, cystatin C or both in routine care[J]. Nephrol Dial Transplant, 2024, 39(4): 694-706. doi: 10.1093/ndt/gfad219 [22] Xu X, Nie S, Xu H, et al. Detecting neonatal AKI by serum cystatin C[J]. J Am Soc Nephrol, 2023, 34(7): 1253-1263. doi: 10.1681/ASN.0000000000000125 [23] Wang N, Han F, Pan J, et al. Serum Cys C predicts acute kidney injury in patients with acute pancreatitis: A retrospective study[J]. Arab J Gastroenterol, 2023, 24(4): 238-244. doi: 10.1016/j.ajg.2023.09.003 [24] Fukui K, Yoshida K, Yokochi Y, et al. The importance of the C-terminal cys pair of phosphoribulokinase in phototrophs in thioredoxin-dependent regulation[J]. Plant Cell Physiol, 2022, 63(6): 855-868 doi: 10.1093/pcp/pcac050 [25] 辛国勇, 郑高梅, 唐伟. Cys⁃C、RBP联合UA对老年急性心肌梗死患者PCI术后心力衰竭的诊断价值[J]. 临床误诊误治, 2023, 36(5): 73-77. [26] 陈晓芬, 於林军, 曾宝金. Cys-c KL-6及CC16在新生儿呼吸衰竭中的表达及临床意义[J]. 中国妇幼保健, 2023, 38(12): 2259-2262. doi: 10.19829/j.zgfybj.issn.1001-4411.2023.12.032 [27] 鲁俊, 全斌. 血清hs-CRP、Cys C及PCT水平与肺炎心力衰竭患者预后相关性分析[J]. 中国医药导报, 2020, 17(22): 86-89. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 156
- HTML全文浏览量: 107
- PDF下载量: 68
- 被引次数: 0
