

Analysis of the Correlation Between miR-125b-5p,Cardiac Function,and Myocardial Injury in Patients with HFpEF
-
摘要:
目的 探究射血分数保留型心衰(heart failure with preserved ejection fraction,HFpEF)患者中血清微小核糖核酸-125b-5p(microRNA-125b-5p,miR-125b-5p)、心功能相关指标与心肌损伤的相关性分析。 方法 本研究为横断面研究,选取2023年12月至2025年4月期间于衡水市人民医院接受治疗的225例HFpEF患者,按照美国纽约心脏病学会(New York Heart Association,NYHA)心功能分级将HFpEF患者分为60例Ⅳ级组、98例Ⅲ级组、67例Ⅱ级组。对比各组miR-125b-5p、心功能、心肌损伤相关指标水平。对患者随访12个月,记录患者心血管不良事件(Major adverse cardiovascular events,MACEs)的发生情况,根据MACEs发生情况分为MACEs组(67例)、非MACEs组(158例)。收集各组患者临床资料,比较患者血清miR-125b-5p、心功能、心肌损伤指标水平;Pearson相关分析miR-125b-5p、心功能相关指标与心肌损伤的关系;多因素Logistic回归分析HFpEF患者发生MACEs的风险因素;用受试者工作特征(receiver operating characteristic ,ROC)曲线评估miR-125b-5p、心功能指标对HFpEF患者心血管不良事件的预测价值。 结果 与Ⅱ级相比,Ⅲ级、Ⅳ级组LVEF、miR-125b-5p水平下降,心肌肌钙蛋白 I(cardiac troponin I,cTnI)、N 末端 B 型利钠肽原(N-terminal pro-B-type natriuretic peptide,NT-proBNP)、心室舒张末期内径(left ventricular end diastolic diameter,LVEDD)、左心室质量指数(left ventricular mass index,LVMI)水平和T1 mapping、细胞外容积分数(extracellular volume fraction,ECV)值均上升;与Ⅲ级相比,Ⅳ级组miR-125b-5p、左室射血分数(left ventricular ejection fraction,LVEF)下降,cTnI、NT-proBNP、LVEDD、LVMI水平与T1 mapping、ECV值上升(P < 0.05)。行Logistic回归分析发现,在调整了混杂因素后,LVEF、HDL-C、红细胞比容、cTnI、NT-proBNP、miR-125b-5p均是影响HFpEF患者MACEs发生的影响因素;Pearson相关分析,cTnI、NT-proBNP、T1 mapping、ECV值与LVEF、miR-125b-5p呈负相关,与LVMI、LVEDD呈正相关(P < 0.05)。ROC曲线显示LVEF、LVMI、LVEDD、miR-125b-5p联合检测对MACEs发生的AUC值、敏感度及准确度均高于单一指标检测(P < 0.05)。 结论 HFpEF患者血清 miR-125b-5p水平降低、心功能指标异常,并与心肌损伤之间有关联性,miR-125b-5p、心功能指标联合检测对患者MACEs发生有较高的预测价值。 Abstract:Objective To investigate the correlation between serum microRNA-125b-5p (miR-125b-5p), cardiac function indexes and myocardial injury in patients with heart failure with preserved ejection fraction (HFpEF), and their predictive value for major adverse cardiovascular events (MACEs). Methods A total of 225 patients with HFpEF treated in Hengshui People’s Hospital from December 2023 to April 2025 were selected. According to New York Heart Association (NYHA) cardiac function classification, they were divided into class Ⅱ group (67 cases), class Ⅲ group (98 cases) and class Ⅳ group (60 cases). Serum miR-125b-5p, cardiac troponin I (cTnI), N-terminal pro-B-type natriuretic peptide (NT-proBNP), left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVEDD), left ventricular mass index (LVMI), T1 mapping and extracellular volume fraction (ECV) were detected in each group. All patients were followed up for 12 months, and the occurrence of MACEs was recorded. The patients were divided into MACEs group (67 cases) and non-MACEs group (158 cases). Collect clinical data from patients in each group and compare levels of serum miR-125b-5p, cardiac function, and markers of myocardial injury; Pearson correlation analysis of the relationship between miR-125b-5p, cardiac function-related indicators, and myocardial injury; Multivariate logistic regression analysis was performed to identify risk factors for MACE in patients with HFpEF; receiver operating characteristic (ROC) curves were used to evaluate the predictive value of miR-125b-5p and cardiac function indices for cardiovascular adverse events in patients with HFpEF. Results Compared with the Class II group, the Class III and IV groups showed decreased LVEF and miR-125b-5p levels, as well as elevated levels of cardiac troponin I (cTnI), N-terminal pro-B-type natriuretic peptide (N-terminal pro-B-type natriuretic peptide, NT-proBNP), left ventricular end-diastolic diameter (LVEDD), and left ventricular mass index (LVMI), while T1 mapping and extracellular volume fraction (ECV) values were all elevated; Compared with the Grade III group, the Grade IV group showed decreased levels of miR-125b-5p and left ventricular ejection fraction (LVEF), as well as increased levels of cTnI, NT-proBNP, LVEDD, and LVMI, along with elevated T1 mapping and ECV values (P < 0.05). Logistic regression analysis revealed that, after adjusting for confounding factors, LVEF, HDL-C, hematocrit, cTnI, NT-proBNP, and miR-125b-5p were all risk factors for the occurrence of MACE in patients with HFpEF; Pearson correlation analysis revealed that cTnI, NT-proBNP, T1 mapping, and ECV were negatively correlated with LVEF and miR-125b-5p, and positively correlated with LVMI and LVEDD (P < 0.05). The ROC curve showed that the combined assessment of LVEF, LVMI, LVEDD, and miR-125b-5p had higher AUC values, sensitivity, and accuracy for predicting the occurrence of MACEs than any single parameter (P < 0.05). Conclusion Patients with HFpEF have reduced serum miR-125b-5p levels and abnormal cardiac function parameters, which are associated with myocardial injury; combined testing of miR-125b-5p and cardiac function parameters has high predictive value for the occurrence of MACE in these patients. -
Key words:
- Chronic heart failure /
- Cardiac function /
- Myocardial injury /
- Oxidative stress
-
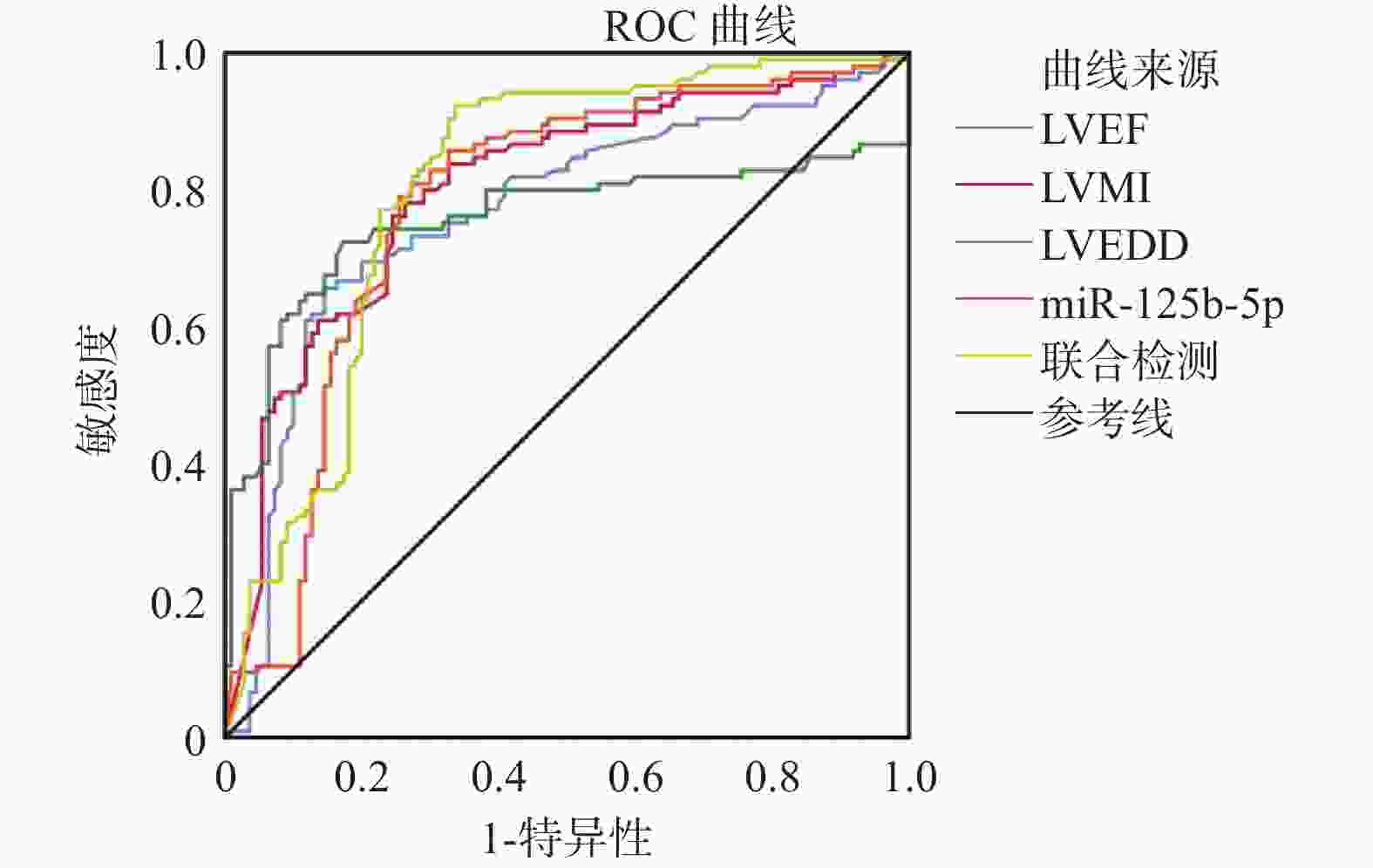
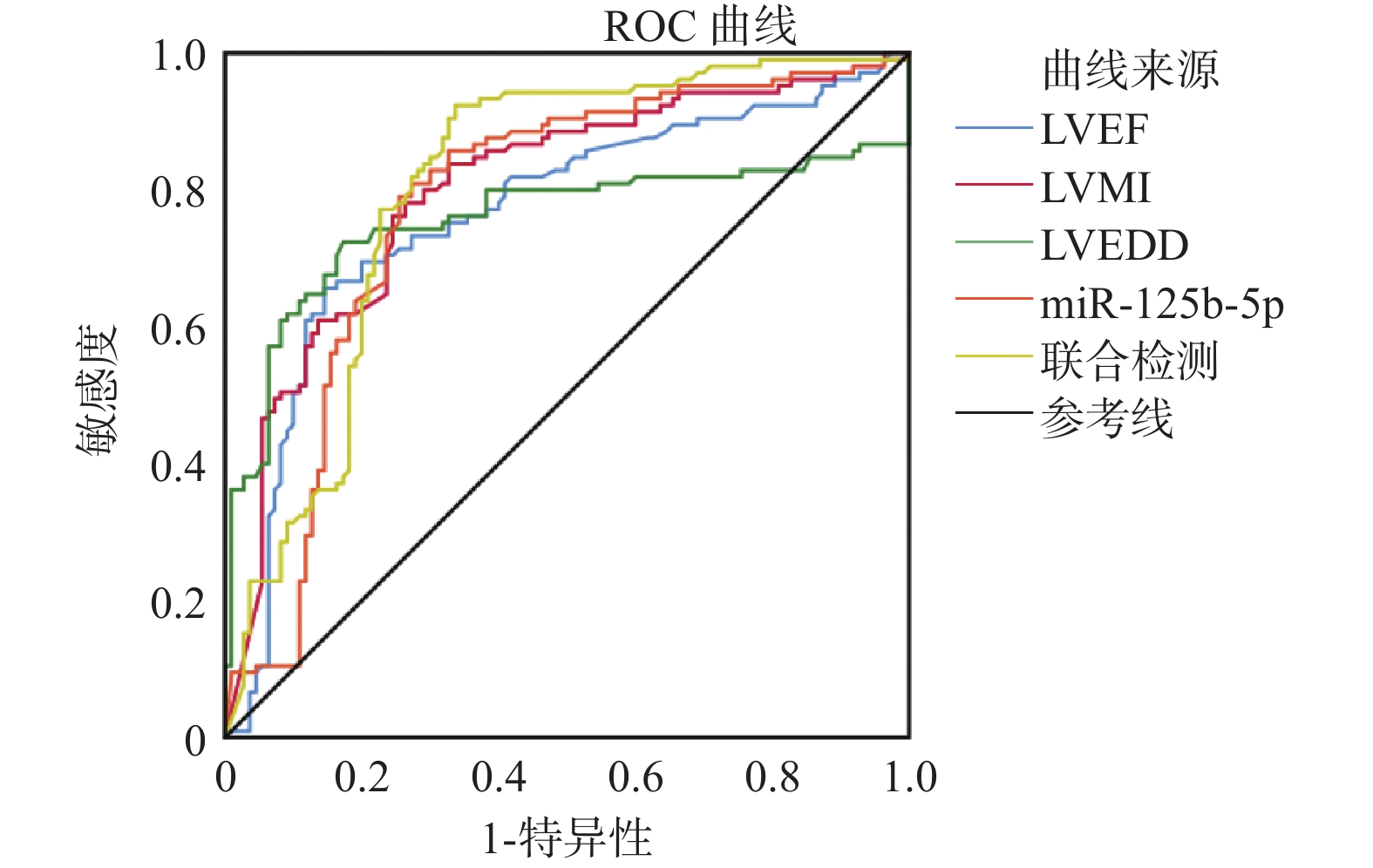
图 1 血清miR-125b-5p、心功能相关指标对HFpEF患者MACEs发生的预测价值(ROC曲线)
Figure 1. Predictive Value of Serum miR-125b-5p and Cardiac Function-Related Indicators for the Occurrence of MACEs in Patients with HFpEF (ROC Curve)
表 1 实时荧光定量PCR使用的引物序列
Table 1. primer sequences designed for real-time quantitative PCR
基因 引物序列(5'-3') 引物长度(bp) U6 F:5'-GCTTCGGCAGCACATATACTAAAAT-3' 42 R:5'-CGCTTCACGAATTTGCGTGTCAT-3' 26 miR-125b-5p F:5'-CAGGAAAGGTTCTGAAGTGACC-3' 37 R:5'-TCACATCCTTTTCGGTTGTAG-3' 60  下载: 导出CSV
下载: 导出CSV
表 2 不同心功能分级下心功能相关指标、miR-125b-5p水平变化($ \bar{x}\pm s $)
Table 2. Changes in heart function-related indicators and mir-125b-5p levels across different heart function grades($ \bar{x}\pm s $)
组别 例数(n) LVEF(%) LVEDD(mm) LVMI(g/m2) Ⅱ级组 67 59.71 ± 2.26 62.32 ± 3.11 121.52 ± 12.53 Ⅲ级组 98 56.05 ± 2.53* 67.24 ± 5.18* 134.55 ± 13.74* Ⅳ级组 60 52.55 ± 3.03*** 72.39 ± 4.22*** 149.58 ± 15.03*** F 120.425 83.054 65.871 P <0.001 <0.001 <0.001 注:与Ⅱ级组相比,*P < 0.05;与Ⅲ级组相比,**P < 0.05
下载: 导出CSV
表 3 不同心功能分级下心肌损伤标志物水平及T1 mapping、ECV值变化($ \bar{x}\pm s $)
Table 3. Levels of cardiac injury markers and changes in t1 mapping and ecv values across different cardiac function classifications ($ \bar{x}\pm s $)
组别 例数(n) cTnI(μg/L) NT-proBNP(μg/L) miR-125b-5p T1 mapping(ms) ECV值(%) Ⅱ级组 67 2.80 ± 0.90 173.07 ± 36.92 0.91 ± 0.28 1033.28 ± 89.6025.94 ± 4.80 Ⅲ级组 98 3.79 ± 1.12* 239.35 ± 38.50* 0.77 ± 0.24* 1144.30 ± 108.75*32.77 ± 5.16* Ⅳ级组 60 4.75 ± 1.31*** 388.18 ± 40.61*** 0.58 ± 0.18*** 1251.47 ± 123.50***44.10 ± 5.69*** F 48.444 514.287 30.314 65.061 195.811 P <0.001 <0.001 <0.001 <0.001 <0.001 与Ⅱ级组相比,*P < 0.05;与Ⅲ级组相比,**P < 0.05
下载: 导出CSV
表 4 MACEs组与非MACEs组基线资料比较[($\bar x \pm s $)/n(%)]
Table 4. Comparison of baseline characteristics between mace and non-mace groups [($\bar x \pm s $)/n(%)]
临床资料 非MACEs组(n = 158) MACEs组(n = 67) t/χ2 P 年龄(岁) 66.13 ± 10.11 66.30 ± 9.82 0.116 0.908 性别 女 69(43.67) 22(32.84) 2.293 0.130 男 89(56.33) 45(67.16) 体重指数(kg/m2) 22.44 ± 2.80 22.62 ± 2.90 0.436 0.663 舒张压(mmHg) 70.17 ± 7.02 69.74 ± 7.92 0.404 0.687 收缩压(mmHg) 127.29 ± 14.80 128.05 ± 12.88 0.366 0.715 心律失常 有 22(13.92) 13(19.40) 1.075 0.299 无 136(86.08) 54(80.60) 冠心病 有 25(15.82) 15(22.39) 1.387 0.239 无 133(84.18) 52(77.61) 合并症情况 糖尿病 31(19.62) 17(25.37) 0.928 0.335 高血压 63(39.87) 32(47.76) 1.199 0.273 心功能分级 Ⅱ 45(28.48) 22(32.84) 0.579 0.749 Ⅲ 69(43.67) 29(43.28) Ⅳ 44(27.85) 16(23.88) 药物治疗史 ACEI/ARB 38(65.52) 42(62.69) 0.108 0.742 阿司匹林 29(50.00) 32(47.76) 0.062 0.803 β受体阻滞剂 24(41.38) 35(52.24) 1.471 0.225 他汀类药物 42(72.41) 50(74.63) 0.078 0.780 5-HT2抑制剂 13(22.41) 17(25.37) 0.149 0.699 钙通道阻滞剂 22(37.93) 28(41.79) 0.193 0.660 其他 13(22.41) 17(25.37) 0.038 0.847 总胆红素(μmol/L) 11.97 ± 3.15 11.34 ± 4.07 1.253 0.211 血钾(mmol/L) 4.05 ± 0.52 4.10 ± 0.53 0.656 0.513 血钠(mmol/L) 139.60 ± 4.09 138.75 ± 3.94 1.441 0.151 红细胞比容(%) 35.79 ± 3.69 34.45 ± 3.62 2.505 0.013 HDL-C(mmol/L) 1.28 ± 0.22 0.82 ± 0.31 12.619 <0.001 LVEF(%) 59.60 ± 3.17 52.22 ± 2.80 16.515 <0.001 LVEDD(mm) 45.08 ± 5.28 46.15 ± 6.70 1.279 0.202 LVMI 129.03 ± 13.74 132.93 ± 13.92 1.939 0.054 cTnI(pμg/L) 2.45 ± 0.57 3.70 ± 0.92 12.385 <0.001 NT-proBNP(μg/L) 153.93 ± 36.01 258.83 ± 40.72 19.205 <0.001 miR-125b-5p 0.93 ± 0.29 0.60 ± 0.20 8.492 <0.001
下载: 导出CSV
表 5 多因素Logistic回归分析HFpEF患者MACEs发生的影响因素
Table 5. Multivariate logistic regression analysis of factors influencing the occurrence of MACEs in patients with HFpEF
因素 β SE Waldx2 OR P 95%可信区间 VIF 红细胞比容 1.105 0.602 3.369 3.019 <0.001 1.815~4.223 1.820 HDL-C 0.862 0.474 3.307 2.368 <0.001 1.420~3.316 1.957 LVEF 0.526 0.183 8.262 1.692 <0.001 1.326~2.058 2.108 cTnI 1.619 0.711 5.185 5.048 <0.001 3.626~6.470 1.794 NT-proBNP 0.008 0.002 16.000 1.008 <0.001 1.004~1.012 2.030 miR-125b-5p 1.396 0.622 5.037 4.039 <0.001 2.795~5.283 1.880
下载: 导出CSV
表 6 HFpEF患者心功能相关指标与心肌损伤的相关性分析
Table 6. Correlation analysis of cardiac function-related indicators and myocardial injury in patients with chronic heart failure
指标 cTnI NT-proBNP T1 mapping ECV值 r P r P r P r P LVEF −0.327 <0.001 −0.308 <0.001 −0.294 <0.001 −0.336 <0.001 LVMI 0.296 <0.001 0.314 <0.001 0.317 <0.001 0.414 <0.001 LVEDD 0.344 <0.001 0.358 <0.001 0.370 <0.001 0.364 <0.001 miR-125b-5p −0.297 <0.001 −0.303 <0.001 −0.306 <0.001 −0.314 <0.001
下载: 导出CSV
表 7 血清miR-125b-5p、心功能相关指标对HFpEF患者MACEs发生的预测效能
Table 7. Predictive performance of serum mir-125b-5p and cardiac function-related indicators for the occurrence of maces in patients with hfpef
指标 AUC值 校正AUC值 敏感度 特异度 准确度 95%CI 校正95%CI LVEF 0.765 0.753 65.19(103/158) 85.07(57/67) 71.11(160/225) 0.698~0.831 0.688~0.817 LVMI 0.781 0.770 77.22(122/158) 77.61(52/67) 77.33(174/225) 0.741~0.841 0.724~0.829 LVEDD 0.756 0.749 71.52(113/158) 82.09(55/67) 74.67(168/225) 0.684~0.829 0.669~0.811 miR-125b-5p 0.778 0.772 81.01(128/158) 73.13(49/67) 78.67(177/225) 0.713~0.843 0.695~0.827 联合检测 0.805 0.802 93.67(148/158) 68.66(46/67) 86.22(194/225) 0.744~0.866 0.737~0.860
下载: 导出CSV
-
[1] Guo B, Shi S, Guo Y, et al. Interventional therapies for chronic heart failure: An overview of recent developments[J]. ESC Heart Fail, 2025, 12(2): 1081-1094. doi: 10.1002/ehf2.15114 [2] Fayyaz A U, Eltony M, Prokop L J, et al. Pathophysiological insights into HFpEF from studies of human cardiac tissue[J]. Nat Rev Cardiol, 2025, 22(2): 90-104. doi: 10.1038/s41569-024-01067-1 [3] Kavousi S, Hosseinpour A, Bahmanzadegan Jahromi F, et al. Efficacy of mesenchymal stem cell transplantation on major adverse cardiovascular events and cardiac function indices in patients with chronic heart failure: A meta-analysis of randomized controlled trials[J]. J Transl Med, 2024, 22(1): 786. doi: 10.1186/s12967-024-05352-y [4] Hinton A Jr, Claypool S M, Neikirk K, et al. Mitochondrial structure and function in human heart failure[J]. Circ Res, 2024, 135(2): 372-396. doi: 10.1161/CIRCRESAHA.124.323800 [5] 唐茜, 张浩, 程景林. NT-proBNP、cTnI、CK-MB在老年冠心病PCI术后预测心衰发生风险的探讨[J]. 分子诊断与治疗杂志, 2022, 14(10): 1770-1774. [6] 刘静, 尤露瑶, 杨羚. 血清proBNP、RDW-CV对射血分数保留型心力衰竭患者发生主要心血管不良事件的预测价值[J]. 中国现代医学杂志, 2025, 35(14): 67-72. doi: 10.3969/j.issn.1005-8982.2025.14.012 [7] Members: A F, McDonagh T A, Metra M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC[J]. European J Heart Fail, 2022, 24(1): 4-131. [8] 袁胜兰, 谭虹珺, 丁鹍. 心力衰竭超声指数与射血分数保留型心力衰竭患者左心功能分级、脑钠肽的相关性及其预后预测价值[J]. 实用临床医药杂志, 2026, 30(2): 90-95. [9] 杜小琴, 王燕侠, 李霞, 等. 血清IL-18、IL-1β及NLRP3炎症小体在射血分数保留型心衰患者中的表达及其与肠道菌群的相关性分析[J]. 现代生物医学进展, 2023, 23(23): 4492-4495. [10] 孙君怡, 薛睿聪, 梁玮昊, 等. 慢性心力衰竭的诊疗现状[J]. 自然杂志, 2022, 44(2): 126-148. [11] 曲鹏, 娄大元. 第四次心肌梗死全球统一定义(2018)要点解读: 重视心肌损伤, 细化心肌梗死诊断[J]. 中国心血管病研究, 2018, 16(11): 961-966. [12] Ciuca-Pană M A, Boulmpou A, Ileri C, et al. Chronic heart failure and coronary artery disease: Pharmacological treatment and cardiac rehabilitation[J]. Medicina, 2025, 61(2): 211. [12] Pastore M C, Campora A, Mandoli G E, et al. Stress echocardiography in heart failure patients: Additive value and caveats[J]. Heart Fail Rev, 2024, 29(5): 1117-1133. doi: 10.1007/s10741-024-10423-9 [13] 祝欣欣, 张琦, 陈芸儿, 等. 射血分数保留型心力衰竭的病理生理学机制研究进展[J]. 中国病理生理杂志, 2023, 39(8): 1499-1508. [14] 谭铭月, 金奕丰, 张俊, 等. 芦荟素减轻大鼠心肌细胞缺氧损伤: 抑制氧化应激和铁死亡[J]. 中国组织工程研究, 2025, 29(25): 5335-5344. doi: 10.12307/2025.525 [15] 沈惠峰, 张小飞, 卢黎敏. 老年慢性心力衰竭患者血清可溶性转铁蛋白受体及可溶性纤维蛋白原2水平与心功能指标及心室重构的相关性[J]. 心脑血管病防治, 2025, 25(2): 36-39. [16] 段宏宇, 刘丹, 王国强. 慢性心力衰竭患者血清miR-217和miR-665表达与心功能和心肌重构的关系研究[J]. 中国循证心血管医学杂志, 2024, 16(9): 1112-1115. doi: 10.3969/j.issn.1674-4055.2024.09.20 [17] 贾妍, 张瑞宁, 黄柳, 等. 慢性心衰患者血清miR-125b-5p、miR-129-5p水平变化及临床意义[J]. 成都医学院学报, 2025, 20(6): 999-1003. [18] He W, Zhao L, Wang P, et al. miR-125b-5p ameliorates ox-LDL-induced vascular endothelial cell dysfunction by negatively regulating TNFSF4/TLR4/NF-κB signaling[J]. BMC Biotechnol, 2025, 25(1): 11. doi: 10.1186/s12896-025-00944-y [19] Bibi A, Madè A, Greco S, et al. Circular PVT1 promotes cardiac fibroblast activation interacting with miR-30a-5p and miR-125b-5p[J]. Cell Death Dis, 2025, 16(1): 325. doi: 10.1038/s41419-025-07652-7 [20] 贾妍, 张瑞宁, 黄柳, 等. 慢性心衰患者血清miR-125b-5p、miR-129-5p水平变化及临床意义[J]. 成都医学院学报, 2025, 20(6): 999-1003. [21] Sakamoto D, Sotomi Y, Matsuoka Y, et al. Prognostic utility and cutoff differences in NT-proBNP levels across subgroups in heart failure with preserved ejection fraction: Insights from the PURSUIT-HFpEF registry[J]. J Card Fail, 2025, 31(5): 771-780. doi: 10.1016/j.cardfail.2024.10.440 [22] 林志彬, 滕中华, 徐艳如, 等. 全血细胞衍生的炎症标志物及其联合N末端B型利钠肽原对慢性心力衰竭患者预后的预测价值[J]. 中华心血管病杂志, 2025, 53(2): 143-150. doi: 10.3760/cma.j.cn112148-20241211-00774 [23] 朱峰, 程娟. AMI合并HF患者血清cTnI、MYO、CK-MB与心力衰竭分级、心室重塑及预后关系[J]. 中国急救复苏与灾害医学杂志, 2024, 19(4): 501-505. [24] 伍伟光, 颜建辉, 何敏锋, 等. 炎症因子、心功能指标与重症脓毒症患者心功能损伤的相关性分析[J]. 检验医学与临床, 2025, 22(7): 969-973. doi: 10.3969/j.issn.1672-9455.2025.07.021 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 104
- HTML全文浏览量: 92
- PDF下载量: 19
- 被引次数: 0
