

Efficacy of Visual Stent Boost-guided Percutaneous Coronary Intervention in Patients with Typical Angina Pectoris and Moderate-to-severe Calcified Lesions
-
摘要:
目的 探讨可视支架影像增强显影技术(Stent Boost)精显指导典型心绞痛合并中重度钙化病变的冠心病患者介入治疗的效果。 方法 前瞻性选取2022年1月至2024年1月180例重庆渝北区中医院典型心绞痛合并中重度钙化病变的冠心病患者作为研究对象,按照随机数字表法分为对照组(n = 90)与实验组(n = 90),并根据实际病情分为中度钙化亚组(n = 30)、重度钙化亚组(n = 30)、特殊人群亚组(n = 30)。对照组采用标准支架植入治疗方案,实验组采用可视Stent Boost精显指导+标准支架植入治疗方案,支架均选择药物洗脱支架。比较两组术中操作便利性及手术效果,以及手术前后心功能指标[左心室射血分数(left ventricular ejection fraction,LVEF)、左心室收缩末期容积(left ventricular end-systolic volume,LVESV)、左心室舒张末期容积(left ventricular end-diastolic volume,LVEDV)]、并发症。并随访12个月,观察对比两组靶病变血运重建、主要不良心血管事件(major adverse cardiovascular events,MACE)事件。 结果 实验组术中即刻支架可视性优良率、支架膨胀率、最小支架管腔直径、最大支架边缘直径、最小支架管腔面积(minimal stent area,MSA)、偏心指数、LVEF均高于对照组,且后扩张率、手术时间、对比剂用量、LVESV、LVEDV均低于对照组(P < 0.05);实验组术后即刻心肌梗死溶栓治疗(thrombolysis in myocardial infarction,TIMI)分级 3级血流比例高于对照组,并发症发生率、MACE发生率低于对照组(P < 0.05);但两组中度钙化亚组、重度钙化亚组、特殊人群亚组术后即刻TIMI 3级血流比例单独比较,差异均无统计学意义(P > 0.05);两组中度钙化亚组、重度钙化亚组患者并发症发生率、MACE发生率比较,差异无统计学意义(P > 0.05);实验组中特殊人群亚组并发症发生率、MACE发生率低于对照组的特殊人群亚组(P < 0.05)。 结论 对于典型心绞痛合并中重度钙化病变的冠心病患者,Stent Boost指导PCI可优化治疗效果,改善术后心功能,降低并发症及MACE发生率,尤其在重度钙化合并分叉病变的患者中价值显著。 -
关键词:
- 冠心病 /
- 冠状动脉钙化 /
- 经皮冠状动脉介入治疗 /
- 支架影像增强显影技术
Abstract:Objective To explore the efficacy of Stent Boost-guided percutaneous coronary intervention (PCI) in treating coronary artery disease (CAD) patients with typical angina pectoris and moderate to severe calcified lesions. Methods A prospective study enrolled 180 CAD patients with typical angina pectoris and moderate-to-severe calcified lesions from January 2022 to January 2024. Patients were randomly divided into control group (n = 90) and experimental group (n = 90), further stratified into three subgroups: moderate calcification subgroup (n = 30), severe calcification subgroup (n = 30), and special population subgroup (n = 30). The control group received standard stent implantation, while the experimental group received Stent Boost-guided visualization combined with standard stent implantation. All patients received drug-eluting stents. We compared intraoperative convenience and efficacy, cardiac function parameters[left ventricular ejection fraction (LVEF), left ventricular end-systolic volume (LVESV), left ventricular end-diastolic volume (LVEDV)] , and complications between the two groups. The patients were followed up for 12 months, and the target lesion revascularization and major adverse cardiovascular events (MACE) events were assessed between the two groups. Results The experimental group demonstrated superior immediate stent visibility, stent expansion rate, minimum stent lumen diameter, maximum stent edge diameter, minimal stent area (MSA), eccentricity index, and LVEF compared to controls. Post-dilation rate, operative time, contrast volume, LVESV, and LVEDV were significantly lower in the experimental group (P < 0.05). The experimental group showed higher proportion of Thrombolysis In Myocardial Infarction (TIMI) grade 3 flow immediately post-procedure, with lower complication and MACE rates (P < 0.05), However, TIMI grade 3 flow proportions showed no significant difference among subgroups between groups (P > 0.05). Complication and MACE rates were similar between groups in moderate and severe calcification subgroups (P > 0.05), while the special population subgroup showed significantly lower complication and MACE rates in the experimental group (P < 0.05). Conclusion For CAD patients with typical angina and moderate-to-severe calcified lesions, Stent Boost-guided PCI optimizes treatment outcomes, improves post-operative cardiac function, and reduces complications and MACE rates, particularly in patients with severe calcification and bifurcation lesions. -
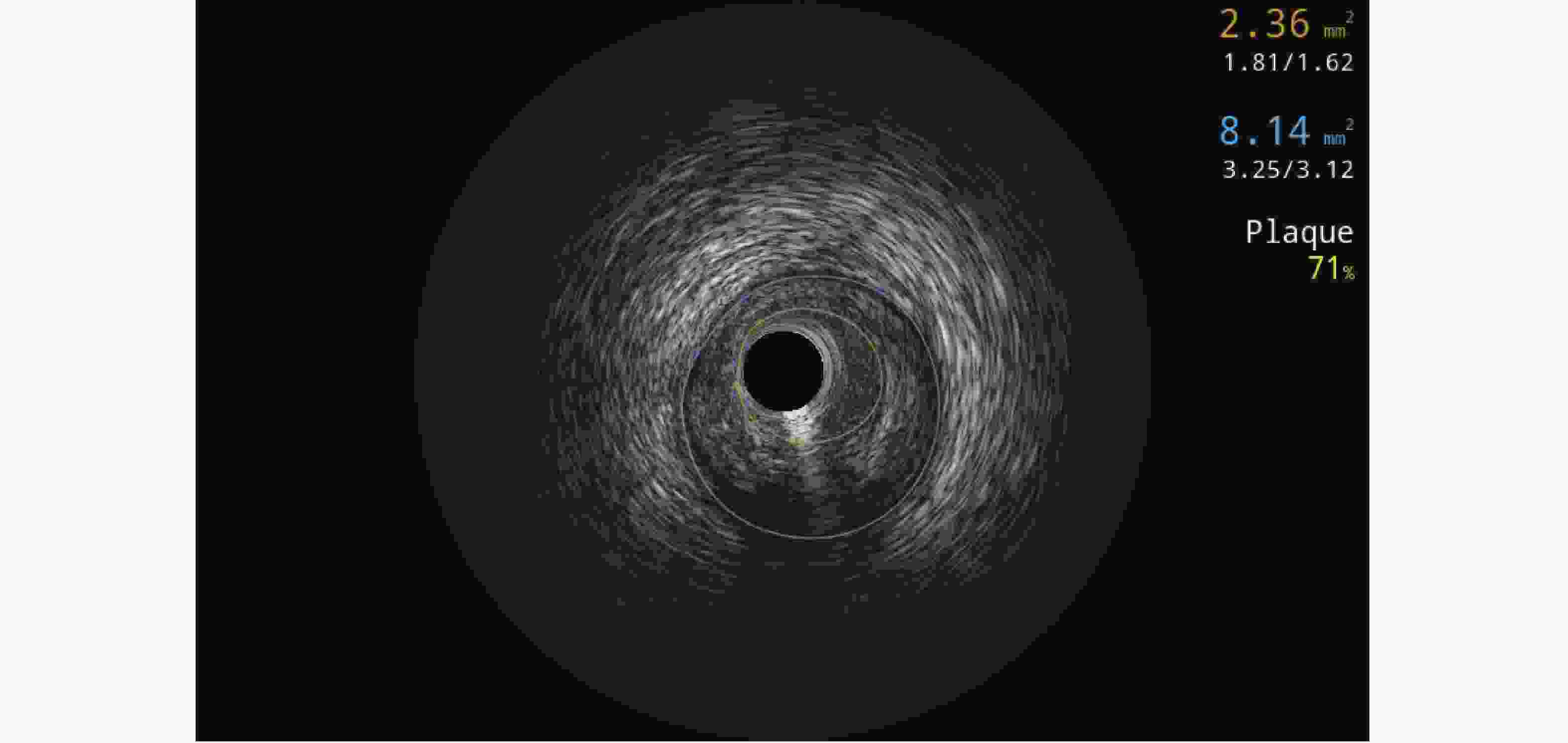
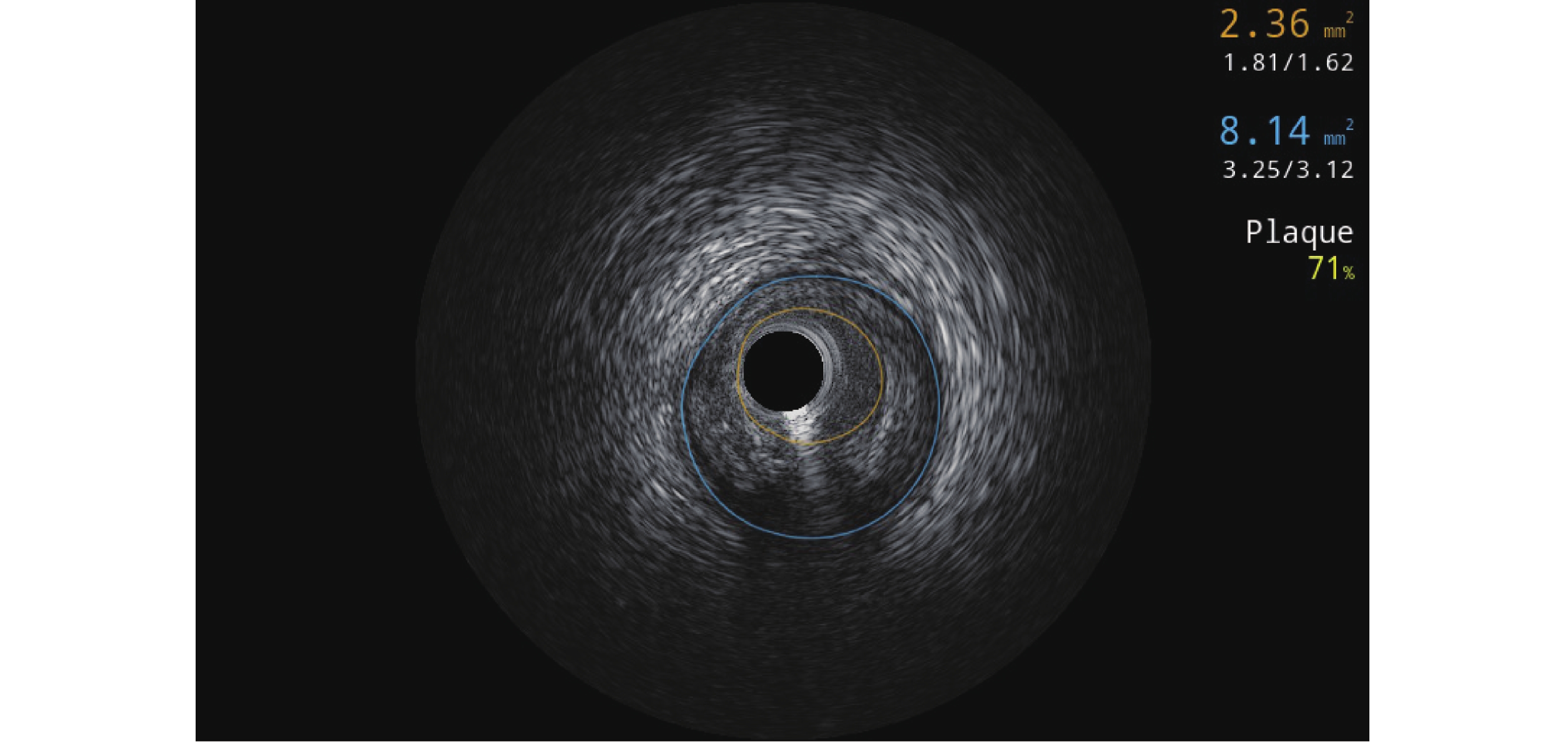
图 1 支架术前冠脉血管内超声图像
Figure 1. Coronary intravascular ultrasound image before stent implantation
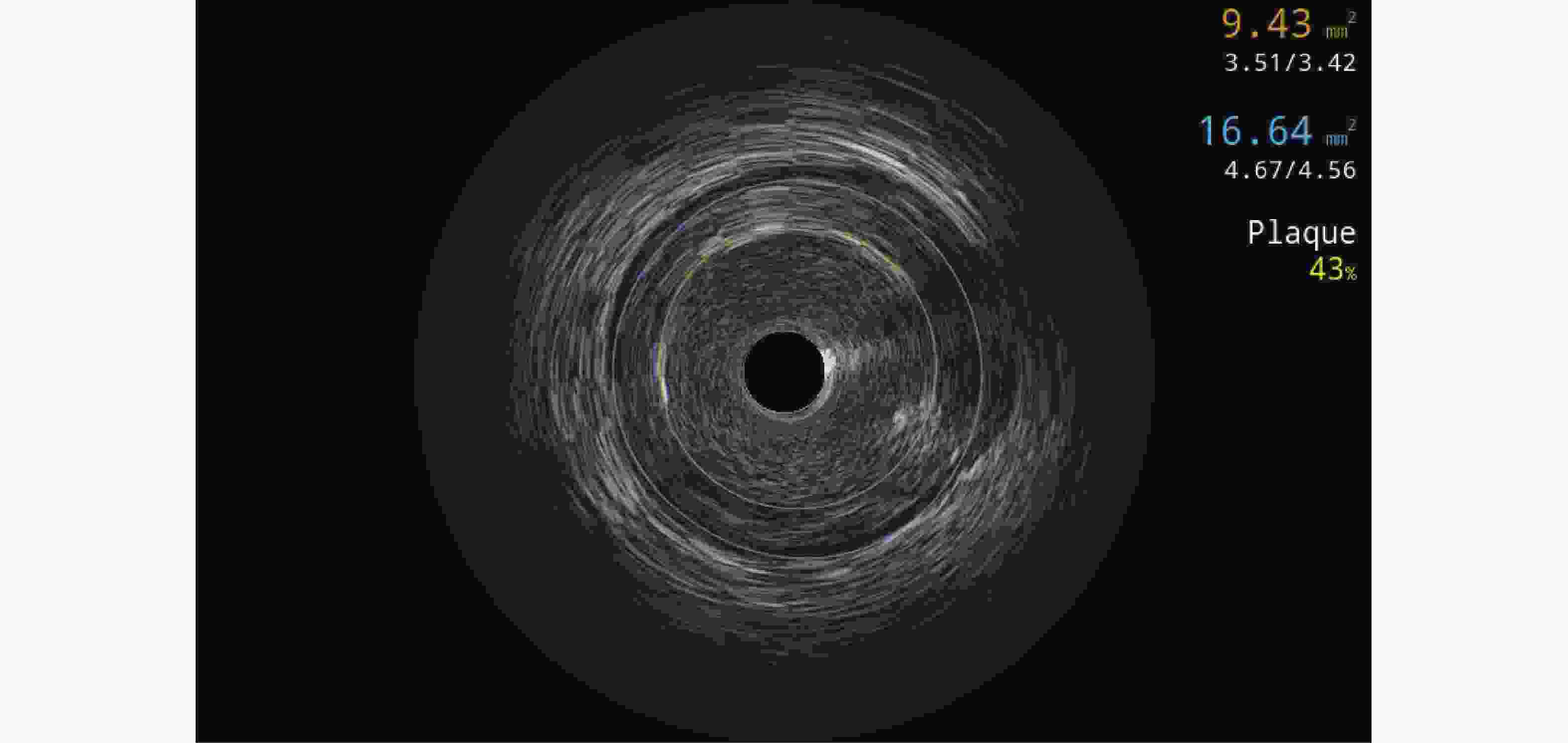
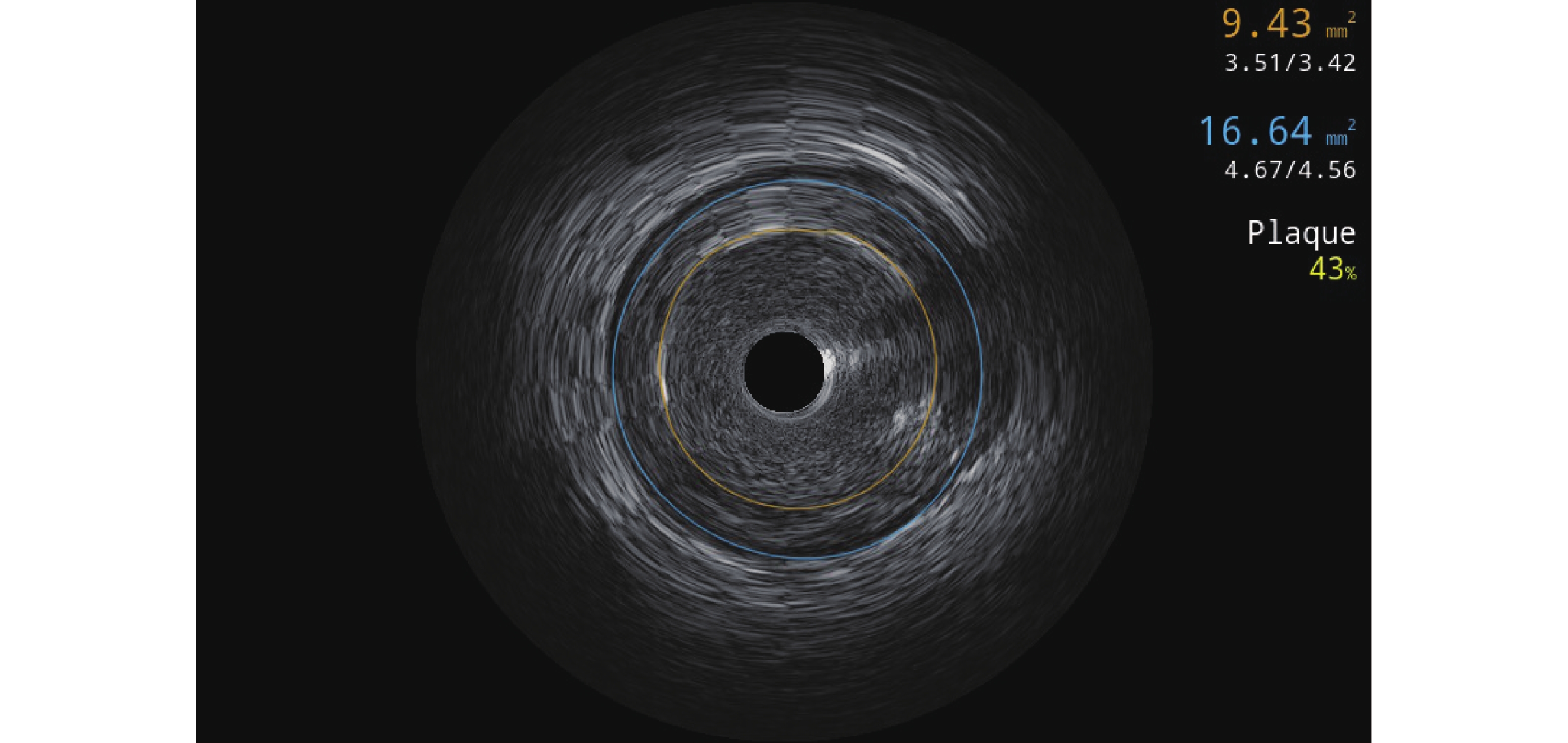
图 2 支架术后Stent Boost支架精显技术+冠脉血管内超声图像
Figure 2. Stent Boost stent precision display technique+coronary intravascular ultrasound image after stent implantation
表 1 两组一般资料比较[n(%)/($ \bar x \pm s $)]
Table 1. Comparison of general information between two groups[n(%)/($ \bar x \pm s $)]
项目 实验组(n=90) 对照组(n=90) χ2/t P 性别 0.602 0.438 男 60(66.67) 55(61.11) 女 30(33.33) 35(38.89) 年龄(岁) 60.49 ± 3.85 61.30 ± 4.10 1.366 0.174 体质量指数(kg/m2) 22.15 ± 1.06 21.93 ± 1.14 1.341 0.182 收缩压(mmHg) 131.02 ± 6.13 130.55 ± 5.58 0.538 0.591 合并高血压 45(50.00) 39(43.33) 0.804 0.370 合并高脂血症 23(25.56) 26(28.89) 0.252 0.615 合并糖尿病 19(21.11) 22(24.44) 0.284 0.594 吸烟史 48(53.33) 53(58.89) 0.564 0.453 靶血管分布 0.969 0.127 左前降支 44(48.89) 41(45.56) 左回旋支 21(23.33) 24(26.67) 右冠状动脉 18(20.00) 20(22.22) 左主干 7(7.78) 5(5.56) 病变长度(mm) 18.71 ± 3.25 19.02 ± 3.61 0.605 0.546 直径狭窄率(%) 85.02 ± 4.04 85.80 ± 4.30 1.254 0.211 Agatston积分 421.09 ± 80.05 430.80 ± 86.47 0.782 0.435  下载: 导出CSV
下载: 导出CSV
表 2 两组治疗效果、并发症、MACE事件比较[n(%)/($ \bar x \pm s $)]
Table 2. Comparison of treatment efficacy,complications,and MACE events between two groups[n(%)/($ \bar x \pm s $)]
观察指标 实验组(n=90) 对照组(n=90) χ2/t 校正后P 第一层(主要疗效指标) 术中即刻 支架可视性优良率 86(95.56) 66(73.33) 16.917 <0.001* 支架膨胀率(%) 89.62 ± 3.50 76.43 ± 5.17 20.042 <0.001* 第二层(次要疗效指标) 最小支架管腔直径(mm) 2.93 ± 0.16 2.80 ± 0.15 5.623 <0.001* 最大支架边缘直径(mm) 3.46 ± 0.23 3.25 ± 0.21 6.397 <0.001* MSA(mm2) 5.39 ± 0.84 4.28 ± 0.97 8.207 <0.001* 偏心指数(%) 15.32 ± 2.02 13.85 ± 1.71 5.269 <0.001* 后扩张率 18(20.00) 41(45.56) 13.338 <0.001* 手术指标 手术时间(min) 40.62 ± 6.21 45.58 ± 6.64 5.176 <0.001* 对比剂用量(mL) 131.49 ± 22.53 154.27 ± 28.19 5.989 <0.001* 术后即刻TIMI 3级血流 89(98.89) 81(90.00) 6.776 <0.001* 术前心功能指标 LVEF(%) 46.33 ± 3.77 46.51 ± 4.02 0.310 0.590 LVESV(mm) 72.08 ± 6.48 71.59 ± 6.13 0.521 0.801 LVEDV(mm) 136.20 ± 10.26 135.42 ± 10.44 0.506 0.745 术后6个月心功能指标 LVEF(%) 52.81 ± 4.18a 49.67 ± 3.97a 5.167 <0.001* LVESV(mm) 60.71 ± 6.07a 65.28 ± 6.29a 4.960 <0.001* LVEDV(mm) 121.57 ± 9.28a 128.63 ± 10.10a 4.883 <0.001* 并发症 冠状动脉穿孔 0(0.00) 1(1.11) 急性支架内血栓 0(0.00) 0(0.00) 导丝断裂/支架脱载 0(0.00) 1(1.11) 慢血流/无复流 1(1.11) 7(7.78) 支架内再狭窄 3(3.33) 5(5.56) 晚期支架内血栓 1(1.11) 1(1.11) 总发生率 5(5.56) 15(16.67) 5.625 0.002* MACE 靶病变血运重建 3(3.33) 5(5.56) 非致死性心肌梗死 1(1.11) 5(5.56) 非致死性卒中 0(0.00) 2(2.22) 心源性死亡 0(0.00) 1(2.22) 总发生率 4(4.44) 13(14.44) 5.262 0.001* 与同组术前比较,aP < 0.05;*P < 0.05。
下载: 导出CSV
表 3 两组中度钙化亚组治疗效果、并发症、MACE事件比较[n(%)/($ \bar x \pm s $)]
Table 3. Comparison of treatment outcomes,complications,and MACE events between two groups of moderate calcification subgroups[n(%)/($ \bar x \pm s $)]
观察指标 实验组中度钙化亚组(n=30) 对照组中度钙化亚组(n=30) χ2/t 校正后P 术中即刻 支架可视性优良率 30(100.00) 24(80.00) 6.667 0.003* 支架膨胀率(%) 92.31 ± 2.40 81.57 ± 2.88 15.691 <0.001* 最小支架管腔直径(mm) 2.96 ± 0.14 2.83 ± 0.12 3.862 <0.001* 最大支架边缘直径(mm) 3.50 ± 0.18 3.28 ± 0.13 5.427 <0.001* MSA(mm2) 5.44 ± 0.72 4.31 ± 0.91 5.334 <0.001* 偏心指数(%) 15.43 ± 1.84 13.72 ± 1.69 3.749 <0.001* 后扩张率 2(6.67) 9(30.00) 5.455 0.005* 手术指标 手术时间(min) 38.71 ± 4.81 42.17 ± 5.02 2.726 0.001* 对比剂用量(mL) 125.63 ± 20.57 146.77 ± 21.49 3.892 <0.001* 术后即刻TIMI 3级血流 30(100.00) 29(96.67) 1.017 0.502 术前心功能指标 LVEF(%) 46.81 ± 3.20 46.85 ± 3.27 0.048 0.496 LVESV(mm) 70.14 ± 5.13 70.08 ± 5.24 0.045 0.752 LVEDV(mm) 132.51 ± 8.18 132.18 ± 9.14 0.147 0.559 术后6个月心功能指标 LVEF(%) 53.36 ± 3.55a 50.27 ± 3.18a 3.551 <0.001* LVESV(mm) 58.35 ± 5.28a 62.17 ± 5.51a 2.742 <0.001* LVEDV(mm) 116.95 ± 7.69a 122.75 ± 8.02a 2.859 <0.001* 并发症 冠状动脉穿孔 0(0.0) 0(0.0) 急性支架内血栓 0(0.0) 0(0.0) 导丝断裂/支架脱载 0(0.0) 0(0.0) 慢血流/无复流 0(0.0) 1(3.33) 支架内再狭窄 1(3.33) 0(0.0) 晚期支架内血栓 0(0.00) 0(0.0) 总发生率 1(3.33) 1(3.33) 0.000 1.000 MACE 靶病变血运重建 1(3.33) 0(0.00) 非致死性心肌梗死 0(0.0) 1(3.33) 非致死性卒中 0(0.0) 0(0.0) 心源性死亡 0(0.0) 0(0.0) 总发生率 1(3.33) 1(3.33) 0.000 1.000 与同组术前比较,aP < 0.05;*P < 0.05。
下载: 导出CSV
表 4 两组重度钙化亚组治疗效果、并发症、MACE事件比较[n(%)/($ \bar x \pm s $)]
Table 4. Comparison of treatment outcomes,complications,and MACE events between two subgroups with severe calcification[n(%)/($ \bar x \pm s $)]
观察指标 实验组重度钙化亚组(n=30) 对照组重度钙化亚组(n=30) χ2/t 校正后P 术中即刻 支架可视性优良率 29(96.67) 22(73.33) 4.706 0.001* 支架膨胀率(%) 89.54 ± 2.71 76.08 ± 3.02 18.169 <0.001* 最小支架管腔直径(mm) 2.92 ± 0.15 2.79 ± 0.12 3.707 <0.001* 最大支架边缘直径(mm) 3.45 ± 0.17 3.24 ± 0.11 5.681 <0.001* MSA(mm2) 5.38 ± 0.72 4.27 ± 0.85 5.458 <0.001* 偏心指数(%) 15.36 ± 1.76 13.89 ± 1.63 3.356 <0.001* 后扩张率 7(23.33) 15(50.00) 4.593 0.001* 手术指标 手术时间(min) 40.53 ± 5.15 45.19 ± 5.23 3.477 <0.001* 对比剂用量(mL) 130.55 ± 20.93 155.21 ± 22.16 4.431 <0.001* 术后即刻TIMI 3级血流 30(100.00) 26(86.67) 2.411 0.159 术前心功能指标 LVEF(%) 46.34 ± 3.38 46.53 ± 3.41 0.217 0.421 LVESV(mm) 72.03 ± 5.39 71.84 ± 5.53 0.135 0.509 LVEDV(mm) 135.84 ± 8.72 135.80 ± 9.47 0.017 0.492 术后6个月心功能指标 LVEF(%) 52.74 ± 3.37a 49.68 ± 3.25a 3.580 <0.001* LVESV(mm) 60.52 ± 6.03a 65.03 ± 6.14a 2.870 <0.001* LVEDV(mm) 120.37 ± 8.15a 128.55 ± 8.32a 3.847 <0.001* 并发症 冠状动脉穿孔 0(0.00) 0(0.00) 急性支架内血栓 0(0.00) 0(0.00) 导丝断裂/支架脱载 0(0.00) 0(0.00) 慢血流/无复流 0(0.00) 3(10.00) 支架内再狭窄 1(3.33) 2(6.67) 晚期支架内血栓 0(0.00) 0(0.00) 总发生率 1(3.33) 5(16.67) 1.667 0.698 MACE 靶病变血运重建 1(3.33) 1(3.33) 非致死性心肌梗死 0(0.00) 2(6.67) 非致死性卒中 0(0.00) 0(0.00) 心源性死亡 0(0.00) 0(0.00) 总发生率 1(3.33) 3(10.00) 0.268 0.526 与同组术前比较,aP < 0.05;*P < 0.05。
下载: 导出CSV
表 5 两组特殊人群亚组治疗效果、并发症、MACE事件比较[n(%)/($ \bar x \pm s $)]
Table 5. Comparison of treatment outcomes,complications,and MACE events between two subgroups of special populations[n(%)/($ \bar x \pm s $)]
观察指标 实验组特殊人群亚组(n=30) 对照组特殊人群亚组(n=30) χ2/t 原始P 校正后P 术中即刻 支架可视性优良率 27(90.00) 20(66.67) 4.812 0.028 0.002* 支架膨胀率(%) 87.01 ± 3.14 71.64 ± 3.39 18.219 <0.001 <0.001* 最小支架管腔直径(mm) 2.91 ± 0.12 2.78 ± 0.11 4.374 <0.001 <0.001* 最大支架边缘直径(mm) 3.43 ± 0.13 3.23 ± 0.10 6.679 <0.001 <0.001* MSA(mm2) 5.35 ± 0.74 4.26 ± 0.82 5.405 <0.001 <0.001* 偏心指数(%) 15.16 ± 1.72 13.93 ± 1.57 2.893 0.005 <0.001* 后扩张率 9(30.00) 17(56.67) 4.344 0.037 0.002* 手术指标 手术时间(min) 42.62 ± 5.28 49.38 ± 5.37 4.917 <0.001 <0.001* 对比剂用量(mL) 138.29 ± 21.42 160.83 ± 23.57 3.876 <0.001 <0.001* 术后即刻TIMI 3级血流 29(96.67) 26(86.67) 1.964 0.161 0.203 术前心功能指标 LVEF(%) 45.84 ± 3.52 46.15 ± 3.60 0.337 0.737 0.361 LVESV(mm) 74.07 ± 5.84 72.85 ± 5.96 0.801 0.427 0.255 LVEDV(mm) 140.25 ± 9.31 138.28 ± 10.02 0.789 0.433 0.308 术后6个月心功能指标 LVEF(%) 52.33 ± 3.64a 49.06 ± 3.40a 3.596 0.001 <0.001* LVESV(mm) 63.26 ± 6.48a 68.64 ± 6.52a 3.206 0.002 <0.001* LVEDV(mm) 127.39 ± 8.36a 134.59 ± 8.73a 3.263 0.002 <0.001* 并发症 冠状动脉穿孔 0(0.00) 1(3.33) 急性支架内血栓 0(0.00) 0(0.00) 导丝断裂/支架脱载 0(0.00) 1(3.33) 慢血流/无复流 0(0.00) 3(10.00) 支架内再狭窄 1(3.33) 3(10.00) 晚期支架内血栓 1(3.33) 1(3.33) 总发生率 2(6.67) 9(30.00) 5.455 0.020 0.003* MACE 靶病变血运重建 1(3.33) 4(13.33) 非致死性心肌梗死 1(3.33) 2(6.67) 非致死性卒中 0(0.00) 1(3.33) 心源性死亡 0(0.00) 1(3.33) 总发生率 2(6.67) 8(26.67) 4.320 0.038 0.005* 与同组术前比较,aP < 0.05;*P < 0.05。
下载: 导出CSV
-
[1] 沈玉, 杨雪梅, 杨露, 等. 高龄人群发生冠心病的影响因素及PCI术的疗效分析[J]. 心血管康复医学杂志, 2023, 32(6): 564-569. doi: 10.3969/j.issn.1008-0074.2023.06.04 [2] Ali Z A, Landmesser U, Maehara A, et al. OCT-guided vs angiography-guided coronary stent implantation in complex lesions an ILUMIEN IV substudy[J]. J Am Coll Cardiol, 2024, 84(4): 368-378. [3] Pesarini G, Hellig F, Seth A, et al. Percutaneous coronary intervention for calcified and resistant lesions[J]. EuroIntervention, 2025, 21(7): e339-e355. doi: 10.4244/EIJ-D-24-00195 [4] El Jattari H, Holvoet W, De Roeck F, et al. Intracoronary lithotripsy in calcified coronary lesions: A multicenter observational study[J]. J Invasive Cardiol, 2022, 34(1): 24-31. doi: 10.25270/jic/21.00021 [5] Shin D, Karimi Galougahi K, Spratt J C, et al. Calcified nodule in percutaneous coronary intervention: Therapeutic challenges[J]. JACC Cardiovasc Interv, 2024, 17(10): 1187-1199. doi: 10.1016/j.jcin.2024.03.032 [6] Dong H, Shan Y, Gong S, et al. Clinical research of drug-coated balloon after rotational atherectomy for severe coronary artery calcification[J]. BMC Cardiovasc Disord, 2023, 23(1): 40. doi: 10.1186/s12872-023-03071-8 [7] Demuyakor A, Hu S, Koniaeva E, et al. Impact of nodular calcification in patients with acute coronary syndrome (ACS) treated with primary percutaneous coronary intervention (PCI)[J]. BMC Cardiovasc Disord, 2022, 22(1): 103. doi: 10.1186/s12872-022-02551-7 [8] Shin D, Hong D, Singh M, et al. Intravascular imaging-guided percutaneous coronary intervention for heavily calcified coronary lesions: A systematic review and meta-analysis[J]. Int J Cardiovasc Imaging, 2024, 40(8): 1653-1659. doi: 10.1007/s10554-024-03150-7 [9] 李利军, 罗建平, 刘安恒, 等. 支架影像增强显影技术指导冠状动脉支架球囊后扩张的辐射剂量[J]. 临床与病理杂志, 2019, 39(6): 1255-1259. doi: 10.3978/j.issn.2095-6959.2019.06.017 [10] 贾小伟, 张蛟, 李屹, 等. 支架影像增强显影技术对冠状动脉分叉病变介入治疗的作用[J]. 武警医学, 2017, 28(7): 672-674. doi: 10.3969/j.issn.1004-3594.2017.07.007 [11] Kapoor K, Cainzos-Achirica M, Nasir K. The evolving role of coronary artery calcium in preventive cardiology 30 years after the Agatston score[J]. Curr Opin Cardiol, 2020, 35(5): 500-507. doi: 10.1097/HCO.0000000000000771 [12] 张蛟, 段媛媛, 俞泓, 等. 支架影像增强显影技术对老年ST段抬高型心肌梗死患者支架膨胀不良的指导作用[J]. 中华老年心脑血管病杂志, 2022, 24(2): 132-135. doi: 10.3969/j.issn.1009-0126.2022.02.006 [13] Hecht H S, Blaha M J, Kazerooni E A, et al. CAC-DRS: Coronary artery calcium data and reporting system. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT)[J]. J Cardiovasc Comput Tomogr, 2018, 12(3): 185-191. doi: 10.1016/j.jcct.2018.03.008 [14] Watanabe Y, Sakakura K, Taniguchi Y, et al. Long-term outcomes of the modest stent expansion strategy for the culprit lesion of acute myocardial infarction[J]. Cardiovasc Interv Ther, 2022, 37(4): 660-669. doi: 10.1007/s12928-022-00841-7 [15] 崔云峰, 卫铁军, 盛强, 等. 支架血流精显技术评估冠状动脉支架贴壁性的初步临床研究[J]. 实用放射学杂志, 2022, 38(4): 639-642. doi: 10.3969/j.issn.1002-1671.2022.04.030 [16] 陈亚楠. 生物可吸收冠脉支架的弹塑性变形及动力学行为研究[D]. 北京: 北京科技大学, 2023. [17] Fujita T, Tazaki J, Toyofuku M. A case report of coronary artery aneurysms with restenosis and stent fractures developed 14 years after sirolimus eluting stents implantation successfully treated with drug-coated balloons[J]. Eur Heart J Case Rep, 2024, 8(2): ytae050. doi: 10.1093/ehjcr/ytae050 [18] Chen D, Gadeley R, Wang A, et al. Coronary artery perforation after bioresorbable scaffold implantation treated with a new generation covered stent-OCT insights[J]. BMC Cardiovasc Disord, 2022, 22(1): 66. doi: 10.1186/s12872-022-02501-3 [19] Onnis C, Virmani R, Kawai K, et al. Coronary artery calcification: Current concepts and clinical implications[J]. Circulation, 2024, 149(3): 251-266. doi: 10.1161/CIRCULATIONAHA.123.065657 [20] Aldana-Bitar J, Karlsberg R P, Budoff M J. Dealing with calcification in the coronary arteries[J]. Expert Rev Cardiovasc Ther, 2023, 21(4): 237-240. doi: 10.1080/14779072.2023.2197594 [21] van der Bie J, Sharma S P, Hirsch A, et al. Coronary stent imaging with photon-counting detector CT[J]. Radiol Cardiothorac Imaging, 2025, 7(3): e240338. doi: 10.1148/ryct.240338 [22] 李夺, 向园, 刘欣, 等. 冠状动脉侧支循环影响PCI术后再狭窄风险的meta分析[J]. 临床心血管病杂志, 2019, 35(1): 79-83. [23] Wang G, Wu X. Ostial lesion of the anterior descending coronary artery treated via Szabo technique supported by stent boost imaging: A case report[J]. J Cardiothorac Surg, 2021, 16(1): 134. doi: 10.1186/s13019-021-01516-9 [24] Mansour H M, Mohamed A M, Ibrahim S G, et al. Value of stent boost imaging in decision making after coronary stenting[J]. Int J Cardiovasc Imaging, 2023, 39(12): 2557-2566. doi: 10.1007/s10554-023-02961-4 [25] 刘伟丽, 廉哲勋, 李大成, 等. 支架精显技术在冠状动脉支架植入术中的应用[J]. 介入放射学杂志, 2020, 29(7): 659-663. doi: 10.3969/j.issn.1008-794X.2020.07.004 [26] 付强, 李欢欢, 陈迎春, 等. 支架精细显影与3D-DSA影像融合技术在评价血流导向装置贴壁性的应用[J]. 中国微侵袭神经外科杂志, 2023, 27(12): 95-98. doi: 10.11850/j.issn.1009-122X.2023.12.021 [27] Leancă S A, Crișu D, Petriș A O, et al. Left ventricular remodeling after myocardial infarction: From physiopathology to treatment[J]. Life, 2022, 12(8): 1111. doi: 10.3390/life12081111 [28] Cirillo P, Izzo R, Mancusi C, et al. Impact of drug-eluting stents on left ventricular wall motion after successful reperfusion of first anterior ST elevation myocardial infarction[J]. Minerva Cardiol Angiol, 2021, 69(2): 144-153. doi: 10.23736/s2724-5683.20.05176-2 [29] 胡司淦, 陈天平, 陈耀, 等. 血管内超声评估冠状动脉钙化病变特征对PCI术后支架膨胀的影响[J]. 介入放射学杂志, 2023, 32(4): 354-358. doi: 10.3969/j.issn.1008-794X.2023.04.009 [30] Duan Y, Jing L, Pan S, et al. Optical coherence tomography: Evaluating the effects of stent boost subtract imaging on stent underexpansion in STEMI patients[J]. BMC Cardiovasc Disord, 2022, 22(1): 62. doi: 10.1186/s12872-022-02498-9 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 380
- HTML全文浏览量: 230
- PDF下载量: 140
- 被引次数: 0
