

Predictors of Left Ventricular Reverse Remodeling in HFrEF Patients Treated with ARNI Combined with Standard Heart Failure Therapy
-
摘要:
目的 基于心脏磁共振成像(cardiac magnetic resonance imaging,CMR),分析影响射血分数降低的心力衰竭(heart failure with reduced ejection fraction,HFrEF)患者经血管紧张素受体脑啡肽酶抑制剂(angiotensin receptor-neprilysin inhibitor,ARNI)联合标准抗心衰药物治疗后发生左心室逆重构(left ventricular reverse remodeling,LVRR)的影响因素。 方法 本研究纳入就诊于昆明医科大学第一附属医院的HFrEF患者65名,均采用ARNI联合标准抗心衰药物治疗。收集患者的临床资料、用药情况、CMR及超声心动图指标。根据超声心动图随访结果分为LVRR组和非LVRR组,并进行统计学分析,得出LVRR的预测因素。 结果 患者中位随访时间10(5,20)个月。LVRR组31例(48%),非LVRR组34例(52%)。与非LVRR组相比,LVRR组ARNI起始剂量较高,房颤发生率较低,室间隔厚度、左室侧壁厚度、心肌质量及心肌质量指数较高,左心房前后径(left atrial anterior-posterior diameter,LAAPD)较小,钆延迟强化(late gadolinium enhancement,LGE)心肌占左室心肌质量百分比(LGE%)较低,差异均有统计学意义(P < 0.05)。将这些变量以LVRR为终点事件进行回归分析,最终得出3个LVRR的预测因素:ARNI起始剂量(OR: 3.253,95%CI: 1.277~8.285,P = 0.013)、LGE%(OR: 0.789 95%CI: 0.647~0.963,P = 0.020)、LAAPD(OR: 0.883,95%CI: 0.804~0.969,P = 0.009)。 结论 ARNI起始剂量、LGE%及LAAPD是HFrEF患者经ARNI联合标准抗心衰药物治疗后LVRR的预测因素。CMR可为ARNI抗心衰治疗提供疗效预测指标。 -
关键词:
- 射血分数降低的心力衰竭 /
- 左心室逆重构 /
- 心脏磁共振成像 /
- 血管紧张素受体脑啡肽酶抑制剂
Abstract:Objective To analyze, based on cardiac magnetic resonance imaging (CMR), the factors influencing the occurrence of left ventricular reverse remodeling (LVRR) in patients with heart failure with reduced ejection fraction (HFrEF) following treatment with an angiotensin receptor-neprilysin inhibitor (ARNI) combined with standard anti-heart failure medications. Methods This study enrolled 65 patients with HFrEF who were treated at the First Affiliated Hospital of Kunming Medical University. All of whom received treatment with ARNI combined with standard anti-heart failure medications. Clinical data, medication history, and CMR and echocardiographic parameters were collected. Patients were divided into an LVRR group and a non-LVRR group based on echocardiographic follow-up results, and statistical analysis was performed to identify predictors of LVRR. Results The median follow-up duration was 10 (5, 20) months. The LVRR group comprised 31 patients (48%), and the non-LVRR group comprised 34 patients (52%). Compared with the non-LVRR group, the LVRR group had a higher initial ARNI dose, a lower incidence of atrial fibrillation, and higher values for interventricular septal thickness, left ventricular lateral wall thickness, myocardial mass, and myocardial mass index. Additionally, the LVRR group had a smaller left atrial anterior-posterior diameter (LAAPD) and a lower percentage of late gadolinium enhancement (LGE) myocardium relative to total left ventricular myocardial mass (LGE%). All these differences were statistically significant (P < 0.05). Regression analysis of these variables with LVRR as the endpoint identified three predictors of LVRR: ARNI starting dose (OR: 3.253, 95%CI: 1.277~8.285, P = 0.013), LGE% (OR: 0.789, 95%CI: 0.647~0.963, P = 0.020), LAAPD (OR: 0.883, 95%CI: 0.804~0.969, P = 0.009). Conclusion ARNI starting dose, LGE%, and LAAPD are predictors of LVRR in patients with HFrEF treated with ARNI combined with standard heart failure medications. CMR can provide prognostic indicators for ARNI therapy in heart failure. -
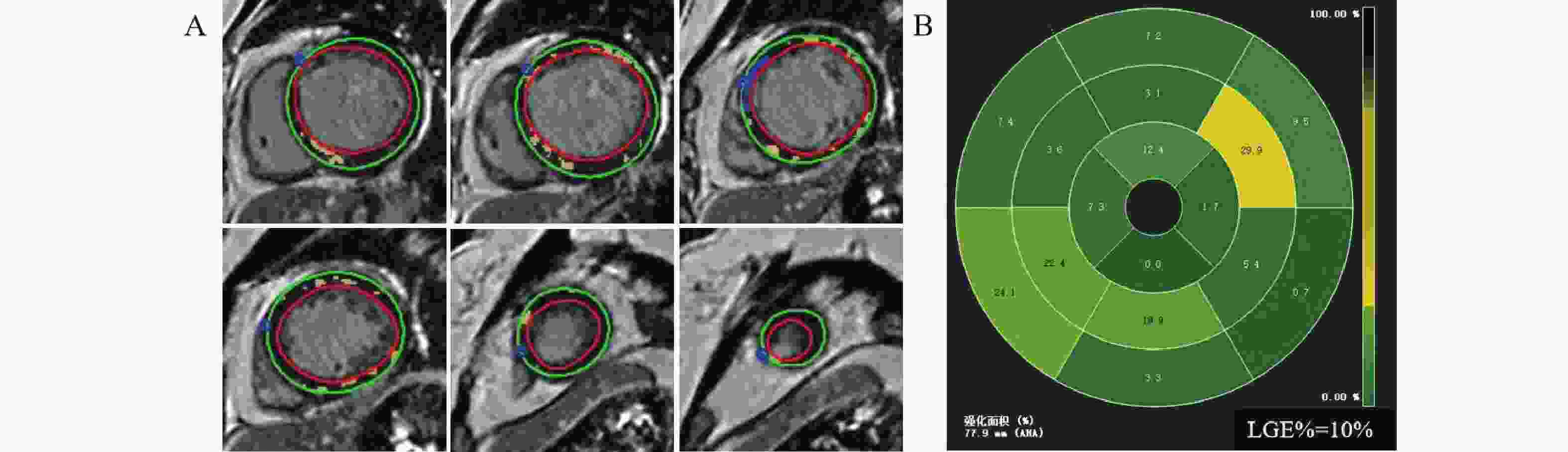
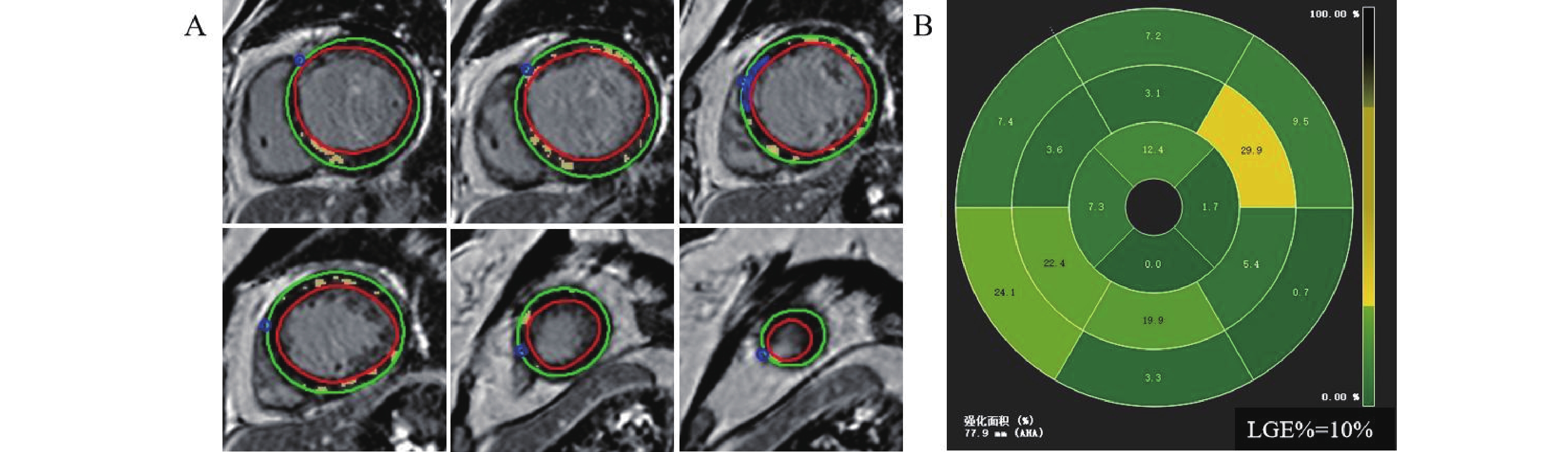
图 1 LGE图像后处理
A:短轴LGE序列图像:红线勾画区域为心内膜,绿线勾画区域为心外膜,蓝线勾画区域为正常心肌参考区,黄色区域为延迟强化心肌;B:左室心肌16节段LGE牛眼图。
Figure 1. LGE Image Post-processing
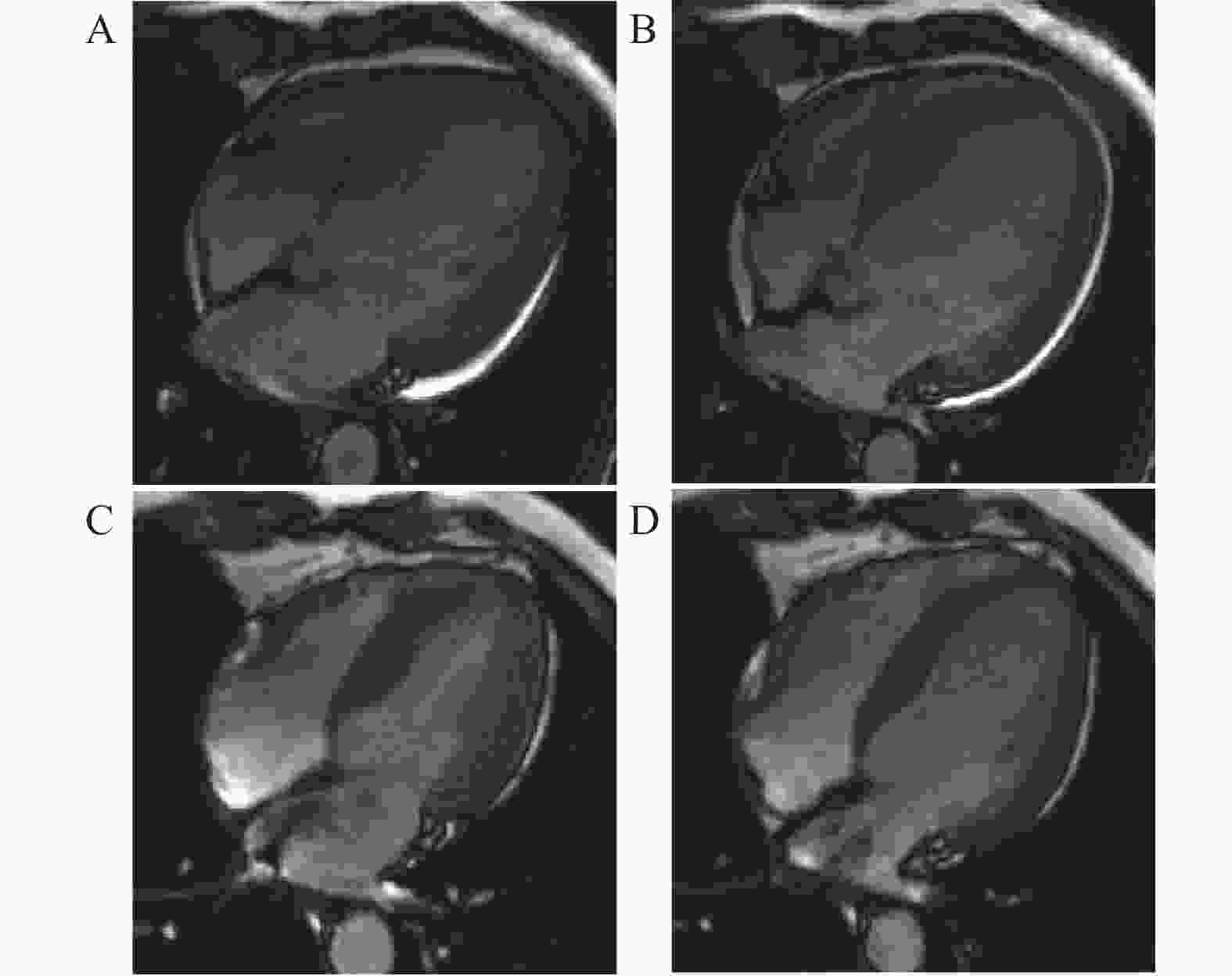
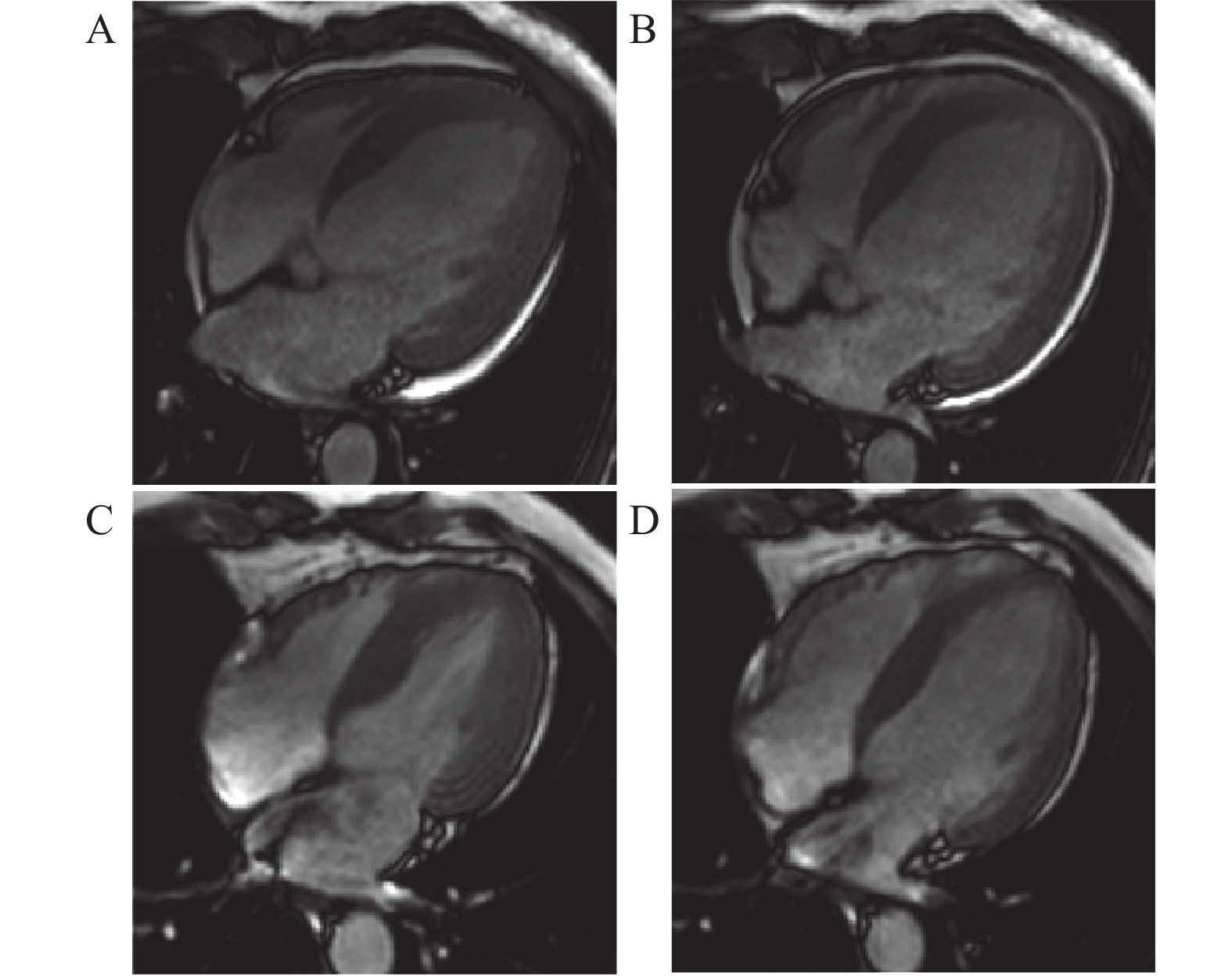
图 2 LVRR组CMR典型病例展示
A:治疗前四腔心电影序列收缩末期图像;B:治疗前四腔心电影序列舒张末期图像;C:治疗后四腔心电影序列收缩末期图像;D:治疗后四腔心电影序列舒张末期图像。
Figure 2. LVRR Group CMR Typical Case Presentation
表 1 心脏磁共振扫描参数
Table 1. Cardiac magnetic resonance scan parameters
参数 序列 TR(ms) TE(ms) FOV(mm) 体素 翻转角(°) 层厚(mm) 层间距(mm) 电影序列 SSFP 42 1.4 330×330 160×172 60 8 2 LGE PSIR 636 3.1 330×330 200×152 25 8 2 TR:重复时间;TE:回波时间;SSFP:稳态自由进动序列;PSIR:相位敏感反转恢复序列。  下载: 导出CSV
下载: 导出CSV
表 2 LVRR组及非LVRR组治疗前后的CMR比较[($\bar x \pm s $)/M(Q1,Q3)]
Table 2. Comparison of baseline and follow-up CMR parameters in the LVRR and non-LVRR groups [($\bar x \pm s $)/M(Q1,Q3)]
项目 组别 治疗前 治疗后 t/Z P 室间隔厚度 (mm) LVRR组(n = 22) 11.1 ± 3.1 11.3 ± 3.9 −0.217 0.830 非LVRR组(n = 19) 9.8 ± 2.2 9.1 ± 1.8 1.263 0.223 左心室侧壁厚度 (mm) LVRR组(n = 22) 8.8 ± 2.5 7.6 ± 2.4 2.632 0.016* 非LVRR组(n = 19) 6.5 ± 1.6 6.0 ± 1.3 1.265 0.222 LAAPD (mm) LVRR组(n = 22) 35.5 ± 7.4 33.0 ± 6.2 1.586 0.128 非LVRR组(n = 19) 40.1 ± 8.3 38.3 ± 5.7 1.043 0.311 左心房横径 (mm) LVRR组(n = 22) 50.1 ± 9.0 40.1 ± 6.7 4.358 <0.001* 非LVRR组(n = 19) 51.3 ± 8.9 46.2 ± 8.1 2.503 0.022* 右心房横径 (mm) LVRR组(n = 22) 46.2 ± 7.8 41.5 ± 7.9 1.874 0.023* 非LVRR组(n = 19) 46.8 ± 8.5 42.4 ± 6.8 2.091 0.051 LVEDV (mL) LVRR组(n = 22) 296.0 ± 97.0 201.0 ± 106.2 4.950 <0.001* 非LVRR组(n = 19) 260.5 ± 77.1 247.3 ± 88.8 1.132 0.272 LVESV (mL) LVRR组(n = 22) 234.7 ± 91.9 115.4 ± 101.9 5.678 <0.001* 非LVRR组(n = 19) 205.7 ± 77.2 180.5 ± 89.0 1.802 0.088 SV (mL) LVRR组(n = 22) 61.3 ± 23.7 85.6 ± 17.8 −3.929 0.001* 非LVRR组(n = 19) 54.8 ± 18.1 66.8 ± 24.8 −2.162 0.044* LVEF LVRR组(n = 22) 22.4 ± 10.8 48.2 ± 14.1 −6.972 <0.001* 非LVRR组(n = 19) 22.6 ± 9.2 29.7 ± 13.0 −2.810 0.012* 心肌质量 (g) LVRR组(n = 22) 170.5 ± 57.2 129.3 ± 43.3 5.945 <0.001* 非LVRR组(n = 19) 121.6 ± 34.5 119.9 ± 38.2 0.396 0.696 LVEDVi (mL/m2) LVRR组(n = 22) 160.9 ± 46.3 118.4 ± 66.9 3.567 0.002* 非LVRR组(n = 19) 154.9 ± 41.3 144.7 ± 50.0 1.601 0.127 LVESVi (mL/m2) LVRR组(n = 22) 127.0 ± 45.6 66.8 ± 57.2 5.203 <0.001* 非LVRR组(n = 19) 122.2 ± 42.0 105.5 ± 50.4 2.229 0.039* SVi (mL/m2) LVRR组(n = 22) 33.9 ± 12.8 47.3 ± 10.0 −4.387 <0.001* 非LVRR组(n = 19) 32.7 ± 9.9 39.2 ± 13.8 −2.040 0.056 心肌质量指数 (g/m2) LVRR组(n = 22) 91.8 ± 25.6 69.8 ± 20.3 5.542 <0.001* 非LVRR组(n = 19) 72.1 ± 16.4 69.5 ± 17.0 0.999 0.331 GRS LVRR组(n = 22) 7.5 (6.3,9.6) 24.1 (14.3,27.7) −3.912 <0.001* 非LVRR组(n = 19) 7.9 (6.1,11.3) 11.3 (7.4,16.3) −3.099 0.002* GCS LVRR组(n = 22) −6.2 (−7.6,−5.2) −15.7 (−17.1,−10.8) −3.977 <0.001* 非LVRR组(n = 19) −6.3 (−8.7,−5.0) −8.1 (−11.2,−6.1) −2.999 0.003* GLS LVRR组(n = 22) −5.7 (−7.1,−3.9) −12.7 (−13.7,−8.2) −4.107 <0.001* 非LVRR组(n = 19) −6.4 (−8.2,−4.4) −7.9 (−11.7,−6.5) −2.417 0.016* LGE% LVRR组(n = 22) 0.8 (0.0,1.4) 0.9 (0.0,1.8) −2.145 0.032* 非LVRR组(n = 19) 2.6 (0.9,10.0) 2.8 (0.5,10.3) −0.804 0.421 *P < 0.05。
下载: 导出CSV
表 3 非LVRR组与LVRR组临床资料比较[n(%)/($\bar x \pm s $)/M(Q1,Q3)]
Table 3. Comparison of clinical characteristics between LVRR and non-LVRR groups [n(%)/($\bar x \pm s $)/M(Q1,Q3)]
项目 非LVRR组(n = 34) LVRR组(n = 31) t/Z/χ2 P 年龄(岁) 50.0 ± 14.0 46.0 ± 14.0 1.187 0.240 性别(男性) 19(55.9) 22(71.0) 1.584 0.208 高血压史 14(41.2) 18(58.1) 1.850 0.174 收缩压(mmHg) 118.0 ± 22.0 123.0 ± 19.0 −0.999 0.322 舒张压(mmHg) 77.0 ± 14.0 80.0 ± 15.0 −0.660 0.512 BSA(m2) 1.7 ± 0.2 1.8 ± 0.2 −1.920 0.059 BNP(pg/mL) 847.0(206.5, 1593.7 )516.0(138.9,980.2) −1.865 0.062 NT-ProBNP(pg/mL) 1254.5 (464.0,6502.0 )1166.0 (402.0,2356.0 )−1.169 0.242 肌酐(μmol/L) 86.3 ± 23.1 102.7 ± 30.1 −2.475 0.016* 心率(次/min) 83.0 ± 12.0 82.0 ± 11.0 0.280 0.780 房颤 6(17.6) 0(0.0) − 0.025* 左束支传导阻滞 6(17.6) 4(12.9) 0.280 0.596 *P < 0.05。
下载: 导出CSV
表 6 非LVRR组与LVRR组超声心动图比较($\bar x \pm s $)
Table 6. Comparison of echocardiographic parameters between LVRR and non-LVRR groups ($\bar x \pm s $)
项目 非LVRR组(n = 34) LVRR组(n = 31) t P LVEDD(mm) 61.0 ± 8.0 64.0 ± 9.0 −1.363 0.178 LVEDV(mL) 217.0 ± 83.0 230.0 ± 85.0 −0.632 0.530 LVESV(mL) 131.0 ± 54.0 153.0 ± 67.0 −1.436 0.156 LVEF(%) 34.0 ± 11.0 34.0 ± 8.0 −0.050 0.960
下载: 导出CSV
表 4 非LVRR组与LVRR组用药情况比较n(%)
Table 4. Comparison of medications between LVRR and non-LVRR groups n(%)
项目 非LVRR组(n = 34) LVRR组(n = 31) Z/χ2 P ARNI起始剂量 12.743 0.006* 25(mg/bid) 16(47.1) 6(19.4) 50(mg/bid) 15(44.1) 16(51.6) 100(mg/bid) 3(8.8) 9(29.0) β受体阻滞剂 31(91.2) 31(100.0) − 0.240 盐皮质激素受体拮抗剂 32(94.1) 26(83.9) − 0.244 利尿剂 26(76.5) 27(87.1) 1.216 0.270 *P < 0.05。
下载: 导出CSV
表 5 非LVRR组与LVRR组CMR比较[($\bar x \pm s $)/M(Q1,Q3)]
Table 5. Comparison of CMR between LVRR and non-LVRR groups [($\bar x \pm s $)/M(Q1,Q3)]
项目 非LVRR组(n = 34) LVRR组(n = 31) t/Z P 室间隔厚度(mm) 9.3 ± 2.7 10.9 ± 3.1 −2.194 0.032* 左心室侧壁厚度(mm) 6.4 ± 1.6 8.0 ± 2.5 −3.034 0.004* LAAPD(mm) 40.9 ± 9.0 35.0 ± 7.5 2.875 0.005* 左心房横径(mm) 51.2 ± 10.3 49.6 ± 9.5 0.635 0.528 右心房横径(mm) 45.1 ± 8.1 45.4 ± 7.2 −0.170 0.865 LVEDV(mL) 261.6 ± 86.9 274.8 ± 90.8 −0.600 0.551 LVESV(mL) 206.6 ± 86.1 215.9 ± 85.9 −0.433 0.666 SV(mL) 55.0 ± 18.1 59.0 ± 23.3 −0.773 0.442 LVEF(%) 23.0 ± 9.5 23.0 ± 10.7 −0.024 0.981 心肌质量(g) 123.1 ± 42.6 157.3 ± 55.3 −2.810 0.007* LVEDVi(mL/m2) 156.5 ± 45 154.2 ± 41.8 0.213 0.832 LVESVi(mL/m2) 123.2 ± 45.4 120.4 ± 41.3 0.259 0.796 SVi(mL/m2) 33.3 ± 10.8 33.8 ± 13.4 −0.167 0.868 心肌质量指数(g/m2) 73.2 ± 19.5 87.6 ± 24.3 −2.634 0.011* GRS(%) 8.0(6.1,11.3) 8.0(6.3,12.8) −0.158 0.875 GCS(%) −6.3(−8.7,−5.0) −6.4(−9.4,−5.2) −0.184 0.854 GLS(%) −6.1(−9.0,−4.4) −6.0(−7.9,−3.9) −0.348 0.728 LGE%(%) 3.3(1.2,10.0) 0.8(0.0,1.4) −3.700 <0.001* *P < 0.05。
下载: 导出CSV
表 7 单因素及多因素Logistic回归分析
Table 7. Univariate and multivariate Logistic regression analysis
项目 单因素分析 多因素分析 P OR(95%CI) P OR(95%CI) 房颤 0.999 / 肌酐 0.022* 1.024(1.003~1.045) ARNI起始剂量 0.009* 2.739(1.290~5.831) 0.013* 3.253(1.277~8.285) 室间隔厚度 0.037* 1.212(1.011~1.454) 左心室侧壁厚度 0.007* 1.440(1.106~1.877) 心肌质量指数 0.015* 1.031(1.006~1.056) LAAPD 0.010* 0.913(0.852~0.979) 0.009* 0.883(0.804~0.969) LGE% 0.008* 0.767(0.629~0.934) 0.020* 0.789(0.647~0.963) *P < 0.05。
下载: 导出CSV
-
[1] 中华医学会心血管病学分会, 中国医师协会心血管内科医师分会, 中国医师协会心力衰竭专业委员会, 等. 中国心力衰竭诊断和治疗指南2024[J]. 中华心血管病杂志, 2024, 52(3): 235-275. [2] Hao G, Wang X, Chen Z, et al. Prevalence of heart failure and left ventricular dysfunction in China: The China hypertension survey, 2012–2015[J]. Eur J Heart Fail, 2019, 21(11): 1329-1337. doi: 10.1002/ejhf.1629 [3] Wang H, Li Y, Chai K, et al. Mortality in patients admitted to hospital with heart failure in China: A nationwide cardiovascular association database-heart failure centre registry cohort study[J]. Lancet Glob Health, 2024, 12(4): e611-e622. doi: 10.1016/S2214-109X(23)00605-8 [4] 张健, 邹长虹. 扩张型心肌病患者左心室逆重构[J]. 中华心血管病杂志, 2016, 44(4): 287-291. [5] Klem I, Klein M, Khan M, et al. Relationship of LVEF and myocardial scar to long-term mortality risk and mode of death in patients with nonischemic cardiomyopathy[J]. Circulation, 2021, 143(14): 1343-1358. doi: 10.1161/CIRCULATIONAHA.120.048477 [6] McDonagh T A, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Eur Heart J, 2021, 42(36): 3599-3726. doi: 10.1093/eurheartj/ehab368 [7] Docherty K F, Vaduganathan M, Solomon S D, et al. Sacubitril/valsartan: Neprilysin inhibition 5 years after PARADIGM-HF[J]. JACC Heart Fail, 2020, 8(10): 800-810. [8] 中华医学会心血管病学分会心力衰竭学组, 中国医师协会心力衰竭专业委员会, 中华心血管病杂志编辑委员会. 中国心力衰竭诊断和治疗指南2018[J]. 中华心血管病杂志, 2018, 46(10): 760-789. [9] Mitchell C, Rahko P S, Blauwet L A, et al. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: Recommendations from the American society of echocardiography[J]. J Am Soc Echocardiogr, 2019, 32(1): 1-64. doi: 10.1016/j.echo.2018.06.004 [10] Kramer C M, Barkhausen J, Bucciarelli-Ducci C, et al. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update[J]. J Cardiovasc Magn Reson, 2020, 22(1): 17. doi: 10.1186/s12968-020-00607-1 [11] Li Z, Han D, Qi T, et al. Hemoglobin A1c in type 2 diabetes mellitus patients with preserved ejection fraction is an independent predictor of left ventricular myocardial deformation and tissue abnormalities[J]. BMC Cardiovasc Disord, 2023, 23(1): 49. doi: 10.1186/s12872-023-03082-5 [12] 高薇, 陈伟, 王钰, 等. CMR分层纵向应变对肥厚型心肌病心内膜下LGE预测价值初探[J]. 昆明医科大学学报, 2024, 45(8): 58-66. [13] Barison A, Aimo A, Ortalda A, et al. Late gadolinium enhancement as a predictor of functional recovery, need for defibrillator implantation and prognosis in non-ischemic dilated cardiomyopathy[J]. Int J Cardiol, 2018, 250: 195-200. doi: 10.1016/j.ijcard.2017.10.043 [14] Merlo M, Pyxaras S A, Pinamonti B, et al. Prevalence and prognostic significance of left ventricular reverse remodeling in dilated cardiomyopathy receiving tailored medical treatment[J]. J Am Coll Cardiol, 2011, 57(13): 1468-1476. doi: 10.1016/j.jacc.2010.11.030 [15] 唐婷, 胡凤丽, 孙伟, 等. 2023年ACC射血分数保留的心力衰竭患者管理指南解读[J]. 河北医科大学学报, 2024, 45(12): 1369-1373. [16] Kido K, Bianco C, Caccamo M, et al. Evaluating sacubitril/valsartan dose dependence on clinical outcomes in patients with heart failure with reduced ejection fraction[J]. Ann Pharmacother, 2021, 55(9): 1069-1075. doi: 10.1177/1060028020983522 [17] Chen W W, Jiang J, Gao J, et al. Efficacy and safety of low-dose sacubitril/valsartan in heart failure patients: A systematic review and meta-analysis[J]. Clin Cardiol, 2023, 46(3): 296-303. doi: 10.1002/clc.23971 [18] Schaper J, Speiser B. The extracellular matrix in the failing human heart[J]. Basic Res Cardiol, 1992, 87(Suppl 1): 303-309. [19] Abhayaratna W P, Seward J B, Appleton C P, et al. Left atrial size physiologic determinants and clinical applications[J]. J Am Coll Cardiol, 2006, 47(12): 2357-2363. [20] Claus P, Omar A M S, Pedrizzetti G, et al. Tissue tracking technology for assessing cardiac mechanics principles, normal values, and clinical applications[J]. JACC Cardiovasc Imag, 2015, 8(12): 1444-1460. doi: 10.1016/j.jcmg.2015.11.001 [21] Chen K, Chang L, Huang R, et al. Left atrial conduit strain derived from cardiac magnetic resonance is an independent predictor of left ventricular reverse remodeling in patients with nonischemic cardiomyopathy[J]. BMC Med Imag, 2024, 24(1): 2. doi: 10.1186/s12880-023-01162-8 [22] Mullens W, Abrahams Z, Francis G S, et al. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure[J]. J Am Coll Cardiol, 2009, 53(7): 589-596. doi: 10.1016/j.jacc.2008.05.068 [23] Priori S G, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC)[J]. Eur Heart J, 2015, 36(41): 2793-2867. doi: 10.1093/eurheartj/ehv316 [24] Papanastasiou C A, Bazmpani M A, Kokkinidis D G, et al. The prognostic value of right ventricular ejection fraction by cardiovascular magnetic resonance in heart failure: A systematic review and meta-analysis[J]. Int J Cardiol, 2022, 368: 94-103. doi: 10.1016/j.ijcard.2022.08.008 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 160
- HTML全文浏览量: 103
- PDF下载量: 52
- 被引次数: 0
