

Risk Factor Evaluation for Venous Thromboembolism during the Perioperative Period in Gynecology and Rationality Analysis of Anticoagulant Drug Use
-
摘要:
目的 评估妇科围术期静脉血栓栓塞症(venous thromboembolism,VTE)的高危因素并分析该院抗凝药物用药合理性。 方法 选取2023年1月至2024年12月期间在昆明市妇幼保健院妇科就诊的妇科手术患者183列病例资料,其中术后诊断VTE 29例,同期154例手术患者为非血栓组。运用独立样本t检验、Mann-Whitney U检验或χ2检验分析妇科围术期发生VTE的高危因素。运用Logistic回归分析妇科手术后并发VTE的危险因素并构建回归预测模型,绘制ROC曲线评估模型有效性。 结果 D-二聚体值高、开腹手术、血栓病史是妇科术后患者发生VTE的独立危险因素(OR > 1,P < 0.05)。回归构建预测模型AUC较Caprini和G-Caprini高,说明该预测模型有较好区分能力,且其分辨率优于G-Caprini 评分和Caprini 评分。医院VTE预防措施存在机械预防时限不足,出血中风险患者抗凝药物启动时间较晚等问题。 结论 本预测模型有一定临床推广价值,对于抗凝药物使用时机延迟等药物治疗相关问题,临床药师应协助医师评估患者出血风险和血栓风险后,共同制定精准抗凝方案。 Abstract:Objective To evaluate the high-risk factors for venous thromboembolism (venous thromboembolism, VTE) during the perioperative period in gynecology and analyze the rationality of anticoagulant drug use. Methods Clinical data of 183 gynecological surgical patients treated at Kunming Maternal and Child Health Hospital from January 2023 to December 2024 were collected. Among them, 29 diagnosed with postoperative VTE were classified as the VTE group and 154 diagnosed with no postoperative VTE during the same period were classified as the non-thrombosis group. Independent sample t-test, Mann–Whitney U test, or χ2 test were used to analyze high-risk factors for VTE during the perioperative period. Logistic regression analysis was employed to identify risk factors for VTE after the gynecological surgery and a predictive regression model was established. The ROC curve was plotted to evaluate the model’ s validity. Results Elevated D-dimer levels, open abdominal surgery, and history of thrombosis were independent risk factors for VTE in postoperative gynecological patients (OR >1, P < 0.05). The AUC of the regression-based predictive model was higher than that of the Caprini and G-Caprini scores, indicating that this model had the good discriminatory ability its resolution was better than G-Caprini and Caprini risk assessment tools. The identified issues in VTE prophylaxis at the hospital included the insufficient mechanical prevention time limit and delayed initiation of anticoagulant therapy in patients at moderate risk of bleeding. Conclusion This predictive model has certain clinical value for broader application. For issues related to drug therapy such as delayed use of anticoagulant drugs, clinical pharmacists should collaborate with physicians to assess patients’ bleeding and thrombosis risks, jointly develop precise anticoagulation regimens. -
Key words:
- Perioperative period /
- Thromboembolism /
- Risk assessment /
- Anticoagulant
-
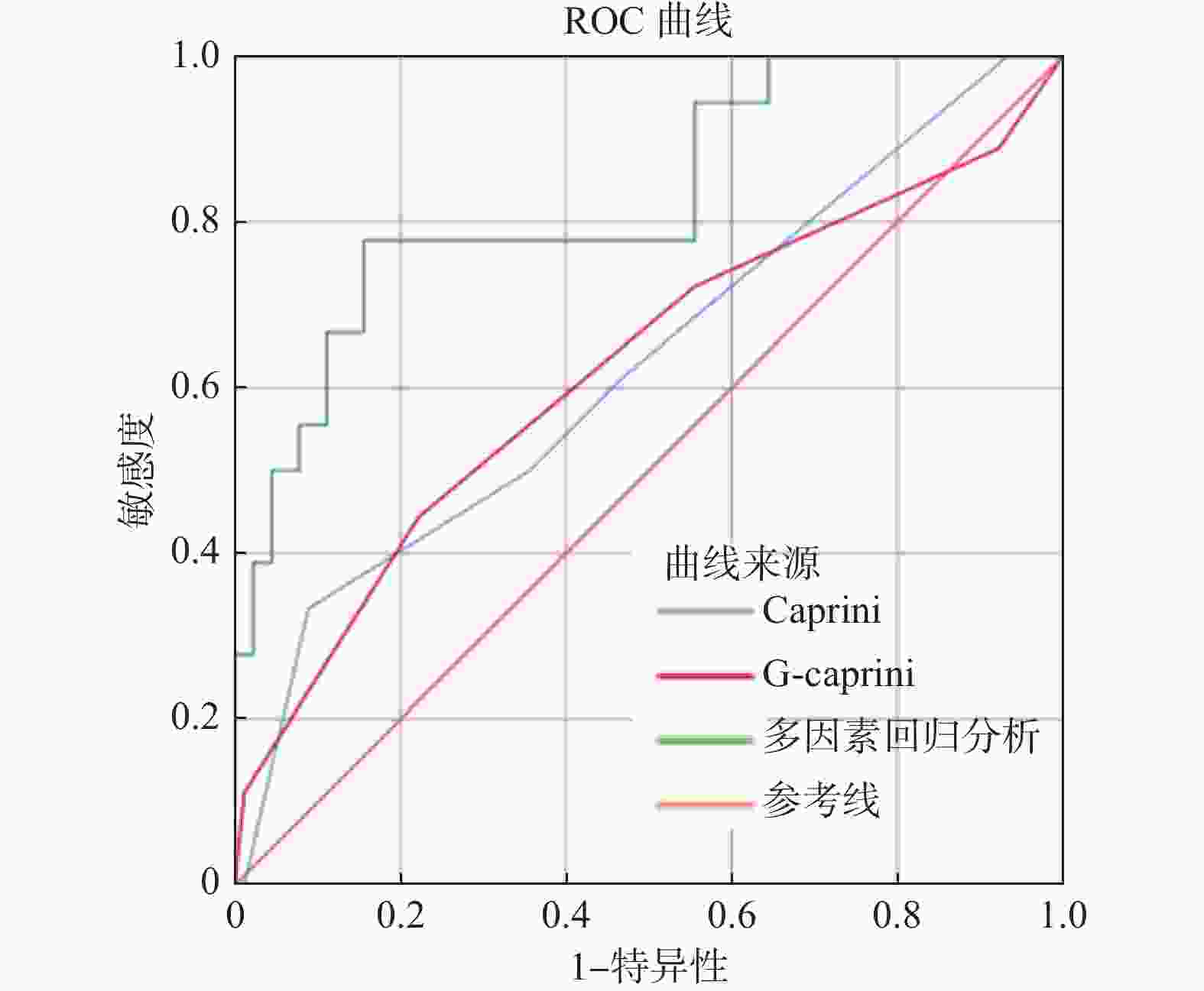
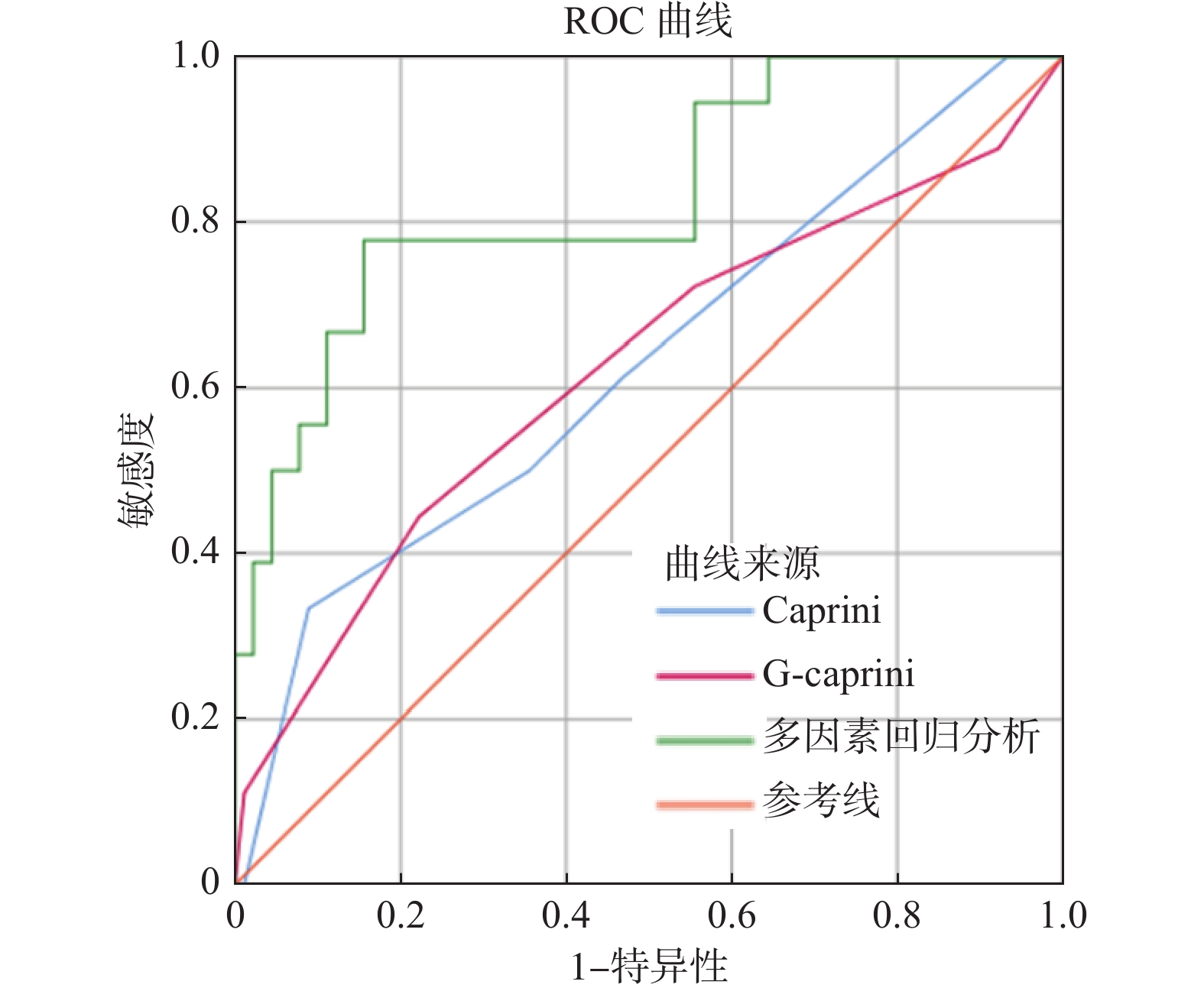
图 1 回归方程与VTE量表预测VTE的ROC曲线
Figure 1. Regression equation and ROC curve of VTE scale for predicting VTE
表 1 G-Caprini评估模型与Caprini评估模型有效性比较 [n(%)]
Table 1. Comparison of the validity of G-Caprini evaluation model and Caprini evaluation model[n(%)]
组别 分级 G-Caprini Caprini χ2 P 血栓组 低危 3(10.34) 0(0.00) 3.164 0.236 中危 7(24.14) 8(27.59) 0.090 0.764 高危及(或)极高危 19(65.52) 21(72.41) 0.322 0.570 非血栓组 低危 19(12.34) 1(0.65) 17.325 <0.001* 中危 63(40.91) 90(58.44) 9.468 0.002* 高危及(或)极高危 72(46.75) 63(40.91) 1.068 0.301 *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 妇科围术期患者并发VTE的危险因素[n(%)/($ \bar x \pm s $)/ M(P25,P75]
Table 2. Risk factors for venous thromboembolism (VTE) in gynecological patients during the postoperative period[n(%)/($ \bar x \pm s $)/ M(P25,P75]
危险因素 分组 t/χ2/Z P 非血栓(n=154) 血栓(n=29) 年龄(岁) 52.70±11.34 52.10±9.68 0.266 0.790 体重(kg) 60.01±9.09 62.97±7.38 −1.235 0.219 BMI( Kg/m2) 24.12±3.35 25.34±3.42 −1.423 0.157 D-二聚体值(mg/L) 1.31(0.81,2.54) 2.41(1.34,4.29) 2.486 0.013* 纤维蛋白原降解产物(mg/L) 6.70(2.80,12.60) 6.00(3.65,31.00) 0.476 0.634 血小板计数(109/L) 255.81±89.26 260.10±86.55 −0.239 0.812 凝血酶原时间(s) 12.28±1.08 12.33±1.09 −0.243 0.808 活化部分凝血活酶时间(s) 26.80±4.20 28.35±5.50 −1.675 0.096 纤维蛋白原(mg/dL) 4.04±2.76 3.05±0.97 1.777 0.078 手术时长(min) 235.40±153.62 285.72±203.43 −1.531 0.127 住院时间(d) 11.77±6.51 13.62±8.63 −1.327 0.186 是否恶性肿瘤患者 15.398 <0.001* 否 111(72.08) 10(34.48) 是 43(27.92) 19(65.52) 手术方式 23.604 <0.001* 开腹 8(5.19) 10(34.48) 腹腔镜术 146(94.81) 19(65.52) 是否高血压 0.004 0.951 否 116(75.32) 22(75.86) 是 38(24.68) 7(24.14) 是否糖尿病 0.861 0.584 否 141(91.56) 28(96.55) 是 13(8.44) 1(53.45) 是否静脉曲张 27.298 <0.001* 否 154(68.18) 24(48.28) 是 0(31.82) 5(51.72) 血栓病史 7.317 0.027* 否 150(97.40) 25(86.21) 是 4(2.60) 4(13.79) *P < 0.05。
下载: 导出CSV
表 3 妇科手术患者VTE危险因素的多因素Logistic 回归分析
Table 3. Multivariate Logistic regression analysis of VTE risk factors in gynecological surgery patients
危险因素 B SE Wald P OR 95%CI 年龄 −0.009 0.033 0.075 0.784 0.991 0.929~1.057 D-二聚体值 0.169 0.082 4.292 0.038* 1.185 1.009~1.391 恶性肿瘤患者 0.454 0.932 0.237 0.626 1.574 0.253~9.773 开腹手术 1.540 0.783 3.869 0.049* 4.665 1.005~21.646 静脉曲张 23.991 21431.327 0.000 0.999 26263912517.000 0.000~0.000 血栓病史 2.817 1.221 5.323 0.021* 16.720 1.528~182.972 手术时长 0.000 0.003 0.000 0.993 1.000 0.995~1.005 BMI 0.141 0.094 2.259 0.133 1.152 0.958~1.385 *P < 0.05。
下载: 导出CSV
表 4 不同评分模型曲线下方区域
Table 4. The areas under the curves of different scoring models
评分模型 AUC P 95%CI Caprini 0.628 0.086 0.481~0.776 G-caprini 0.623 0.102 0.466~0.779 多因素回归方程 0.830 <0.001* 0.720~0.941 *P < 0.05。
下载: 导出CSV
表 5 不同年龄段VTE预防情况及发生率比较[n(%)]
Table 5. Comparison of VTE prevention situations and incidence rates among different age groups [n(%)]
年龄(岁) n 采取预防措施人数及比例 发生VTE人数及
比例χ2 P 气压治疗 药物预防 气压+药物 ≤40 17 5(29.41) 8(47.06) 4(23.53) 3(10.34) 1.469 0.495 41~60 129 30(23.62) 66(51.97) 31(24.41) 20(68.97) 61~75 31 10(33.33) 5(16.67) 15(50.00) 6(20.69) ≥76 6 0(0.00) 5(83.33) 1(16.67) 0(0.00)
下载: 导出CSV
表 6 不同风险人群预防情况及VTE发生率比较[n(%)]
Table 6. Comparison of prevention measures and VTE incidence among different risk groups [n(%)]
评分方法 评分分值(分) n 采取预防措施人数及比例 发生VTE人数及
比例χ2 P 气压 药物 气压+药物 Caprini评分 ≤2 1 0(0.00) 1(100.00) 0(0.00) 0(0.00) 9.804 0.006* 3~4 98 23(23.47) 58(59.18) 17(17.35) 8(8.16) ≥5 84 17(20.73) 30(36.59) 35(42.68) 21(25.00) G-Caprini评分 0 22 6(27.27) 11(50.00) 5(22.73) 3(13.64) 7.584 0.078 1 70 19(27.54) 37(53.62) 13(18.84) 7(10.00) 2 59 12(20.34) 28(47.46) 19(32.20) 9(15.25) ≥3 32 3(9.68) 13(41.94) 15(48.39) 10(31.25) *P < 0.05。
下载: 导出CSV
表 7 不同VTE预防措施患者出血风险评估及VTE发生率比较[n(%)]
Table 7. Assessment of bleeding risk in patients with different VTE preventive measures [n(%)]
预防措施分层 n 出血高风险
人数及占比出血中风险
人数及占比出血低风险
人数及占比发生VTE
人数及占比χ2 P 药物 89 28(31.46) 61(68.64) 0(0.00) 7(7.87) 7.999 0.018* 气压 40 21(52.50) 19(47.50) 0(0.00) 10(25.00) 气压+药物 52 30(57.69) 22(42.31) 0(0.00) 11(21.15) *P < 0.05。
下载: 导出CSV
-
[1] 郎景和, 王辰, 瞿红, 等. 妇科手术后深静脉血栓形成及肺栓塞预防专家共识[J]. 中华妇产科杂志, 2017, 52(10): 649-653. doi: 10.3760/cma.j.issn.0529-567x.2017.10.001 [2] Insin P, Vitoopinyoparb K, Thadanipon K, et al. Prevention of venous thromboembolism in gynecological cancer patients undergoing major abdominopelvic surgery: A systematic review and network meta-analysis[J]. Gynecol Oncol, 2021, 161(1): 304-313. doi: 10.1016/j.ygyno.2021.01.027 [3] 赵晓鹏, 李丹妮, 白俊, 等. 妇科手术患者静脉血栓栓塞症的危险因素评估和改良评估模型建立[J]. 实用妇产科杂志, 2024, 40(1): 64-68. doi: 10.3969/j.issn.1003-6946.2024.1.syfckzz202401016 [4] 浙江省肺栓塞和深静脉血栓防治联盟. 浙江省医院静脉血栓栓塞症防治管理规范专家共识(第二版)[J]. 加速康复外科杂志, 2023, 6(3): 97-109. [5] 中国血栓性疾病防治指南专家委员会. 中国血栓性疾病防治指南[J]. 中华医学杂志, 2018, 98(36): 2861-2888 [6] 马军, 秦叔逵, 吴一龙, 等. 肿瘤相关静脉血栓栓塞症预防与治疗指南(2019版)[J]. 中国肿瘤临床, 2019, 46(13): 653-660. doi: 10.3969/j.issn.1000-8179.2019.13.765 [7] 刘凤林, 张太平. 中国普通外科围手术期血栓预防与管理指南[J]. 消化肿瘤杂志(电子版), 2016, 8(2): 57-62. doi: 10.3969/j.issn.1674-7402.2016.02.004 [8] 乔宇, 武明芬, 柳鑫, 等. 2021中国静脉血栓栓塞症防治抗凝药物的选用与药学监护指南[J]. 中国临床药理学杂志, 2021, 37(21): 2999-3016. [9] 陈丽宇, 肖娟, 吕仙忠, 等. 影响孕产妇下肢深静脉血栓预后的危险因素分析[J]. 山东大学学报(医学版), 2021, 59(7): 38-42. [10] 项汝霏. D-二聚体与FDP联合检测在创伤后深静脉血栓形成风险评估中的应用[J]. 浙江创伤外科, 2024, 29(11): 2162-2164. doi: 10.3969/j.issn.1009-7147.2024.11.052 [11] 方欢, 黄劲峰, 高伟祺, 等. 妇科手术围手术期发生静脉血栓栓塞症的影响因素分析[J]. 中华实用诊断与治疗杂志, 2024, 38(9): 941-946. [12] Alba A C, Agoritsas T, Walsh M, et al. Discrimination and calibration of clinical prediction models: Users' guides to the medical literature[J]. JAMA, 2017, 318(14): 1377-1384. doi: 10.1001/jama.2017.12126 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 880
- HTML全文浏览量: 723
- PDF下载量: 29
- 被引次数: 0
