

The Value of Leukocyte Ratios Combined with Nutritional Indicators in Evaluating Rehabilitation and Short-term Prognosis in Patients with AECOPD
-
摘要:
目的 探讨慢性阻塞性肺疾病急性加重期(acute exacerbation of chronic obstructive pulmonary disease,AECOPD)患者入院时白细胞比值与营养指标的相关性,及其与患者康复效果、短期预后的关联。 方法 选取2022年1月至2024年12月广州市南沙区人民医院收治的82例AECOPD患者(AECOPD组)及同期同院区既往曾因AECOPD住院治疗、目前病情处于基线稳态≥8周的慢性阻塞性肺疾病稳定期(stable chronic obstructive pulmonary disease,SCOPD)患者82例为对照组(SCOPD组)。收集并比较两组患者的一般资料、肺功能、入院时中性粒细胞-淋巴细胞比值(neutrophil-lymphocyte ratio,NLR)、血小板-淋巴细胞比值(platelet-lymphocyte ratio,PLR)、血清白蛋白(serum albumin,ALB)及前白蛋白(prealbumin,PA)水平。采用Pearson相关性分析指标间关联,通过多因素Logistic回归分析影响AECOPD患者康复效果及短期预后的独立因素。 结果 两组基线资料差异无统计学意义(P > 0.05),AECOPD组FEV1/FVC(53.87±8.96)、FEV1(45.29±11.67)% pred低于SCOPD组的(57.34±7.25)、(51.15±10.48)% pred,而年龄(68.76±7.24)岁高于SCOPD组的(65.38±7.19)岁,组间比较有统计学意义(P < 0.05)。AECOPD组NLR(5.14±1.15)、PLR(152.74±20.39)高于SCOPD组(3.20±0.73)、(127.38±14.22),ALB(32.18±6.04)g/L、PA(167.47±36.29)mg/L低于SCOPD组(37.45±5.12)g/L、(180.36±38.18)mg/L,组间比较差异有统计学意义(P < 0.05)。相关性分析显示,NLR与ALB(r = -0.443,P < 0.05)、PA(r = -0.157,P < 0.05)呈负相关,PLR与ALB(r = -0.379,P < 0.05)、PA(r = -0.263,P < 0.05)呈负相关。在进行多因素Logistic回归分析前,对纳入的自变量(年龄、NLR、PLR、ALB、PA)进行共线性诊断,采用方差膨胀因子(VIF)进行评估。结果显示,各变量的VIF值均<3(NLR:2.13,PLR:2.28,年龄:1.42,ALB:1.35,PA:1.28),提示不存在显著的多重共线性问题。多因素Logistic回归显示,年龄(OR = 2.449,95%CI:1.385~4.327)、NLR(OR = 2.066,95%CI:1.156~3.693)、PLR(OR = 2.233,95%CI:1.211~4.120)是康复的独立危险因素,ALB(OR = 0.409,95%CI:0.281~0.595)、PA(OR = 0.472,95%CI:0.423~0.526)是康复良好的保护因素;年龄(OR = 2.370,95%CI:1.351~4.158)、NLR(OR = 2.574,95%CI:1.153~5.750)、PLR(OR = 2.959,95%CI:1.134~7.721)是短期预后的危险因素,ALB(OR = 0.418,95%CI:0.276~0.632)、PA(OR = 0.453,95%CI:0.404~0.507)是短期预后的保护因素。 结论 AECOPD患者入院时NLR、PLR显著升高,ALB、PA显著降低,且炎症指标与营养指标呈显著负相关。NLR和PLR是AECOPD患者康复不佳和短期预后不良的独立危险因素,而ALB和PA是康复良好的保护因素。 Abstract:Objective To explore the correlation between leukocyte ratios and nutritional indicators at admission in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD), and their association with patient clinical outcomes and short-term prognosis. Methods A total of 82 patients with AECOPD admitted to Nansha District People's Hospital of Guangzhou from January 2022 to December 2024 (AECOPD group) and 82 patients with stable chronic obstructive pulmonary disease (SCOPD) who had been hospitalized for AECOPD at the same hospital and had baseline stability for ≥8 weeks (SCOPD group) were selected as controls. General data, pulmonary function, neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), serum albumin (ALB), and prealbumin (PA) levels at admission were collected and compared between the two groups. Pearson correlation analysis was used to analyze the correlations between indicators, and multivariate Logistic regression analysis was used to identify independent factors affecting the clinical outcomes and short-term prognosis of AECOPD patients. Results There was no statistically significant difference in the baseline data between the two groups (P > 0.05). FEV1/FVC (53.87 ± 8.96) and FEV1 (% pred) in the AECOPD group were lower than those in the SCOPD group (57.34 ± 7.25 and 51.15 ± 10.48 % pred), while age (68.76 ± 7.24 years) was higher than in the SCOPD group (65.38 ± 7.19 years), with statistically significant differences between groups (P < 0.05). NLR (5.14 ± 1.15) and PLR (152.74 ± 20.39) in the AECOPD group were higher than in the SCOPD group (3.20 ± 0.73 and 127.38 ± 14.22), while ALB (32.18 ± 6.04) g/L and PA (167.47 ± 36.29) mg/L were lower than in the SCOPD group (37.45 ± 5.12 g/L and 180.36 ± 38.18 mg/L), with statistically significant differences between groups (P<0.05). Correlation analysis showed that NLR was negatively correlated with ALB (r = -0.443, P < 0.05) and PA (r = -0.157, P < 0.05), and PLR was negatively correlated with ALB (r = -0.379, P < 0.05) and PA (r = -0.263, P < 0.05). Prior to multivariate logistic regression analysis, collinearity diagnosis of the included independent variables (age, NLR, PLR, ALB, PA) was performed using the variance inflation factor (VIF). The results showed that all variables had VIF values <3(NLR: 2.13, PLR: 2.28, age: 1.42, ALB: 1.35, PA: 1.28), suggesting no significant multicollinearity issues. Multivariate Logistic regression analysis showed that age (OR = 2.449, 95%CI: 1.385 ~ 4.327), NLR (OR = 2.066, 95%CI: 1.156 ~ 3.693), and PLR (OR = 2.233, 95%CI: 1.211 ~ 4.120) were independent risk factors for poor outcomes, while ALB (OR =0.409, 95%CI: 0.281 ~ 0.595) and PA (OR = 0.472, 95%CI: 0.423 ~ 0.526) were protective factors for good outcomes. Age (OR = 2.370, 95%CI: 1.351 ~ 4.158), NLR (OR = 2.574, 95%CI: 1.153 ~ 5.750), and PLR (OR = 2.959, 95%CI: 1.134 ~ 7.721) were risk factors for short-term prognosis, while ALB (OR =0.418, 95%CI: 0.276 ~ 0.632) and PA (OR = 0.453, 95%CI: 0.404 ~ 0.507) were protective factors for short-term prognosis. Conclusion At admission, AECOPD patients demonstrated significantly elevated NLR and PLR levels and significantly decreased ALB and PA levels, with inflammatory markers negatively correlated with nutritional indicators. NLR and PLR are independent risk factors for poor outcomes and adverse short-term prognosis in AECOPD patients, while ALB and PA are protective factors for good clinical outcomes. -
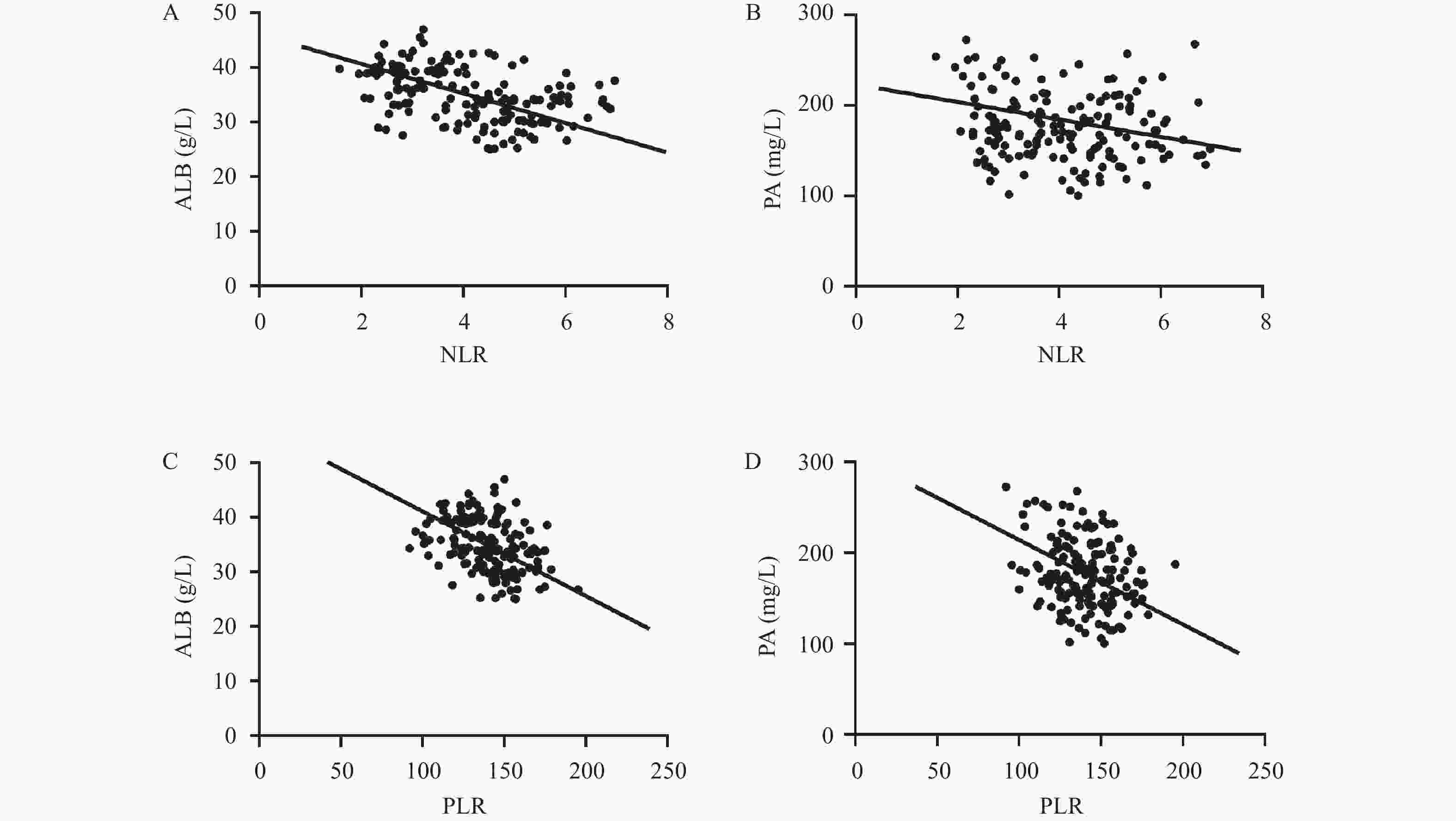
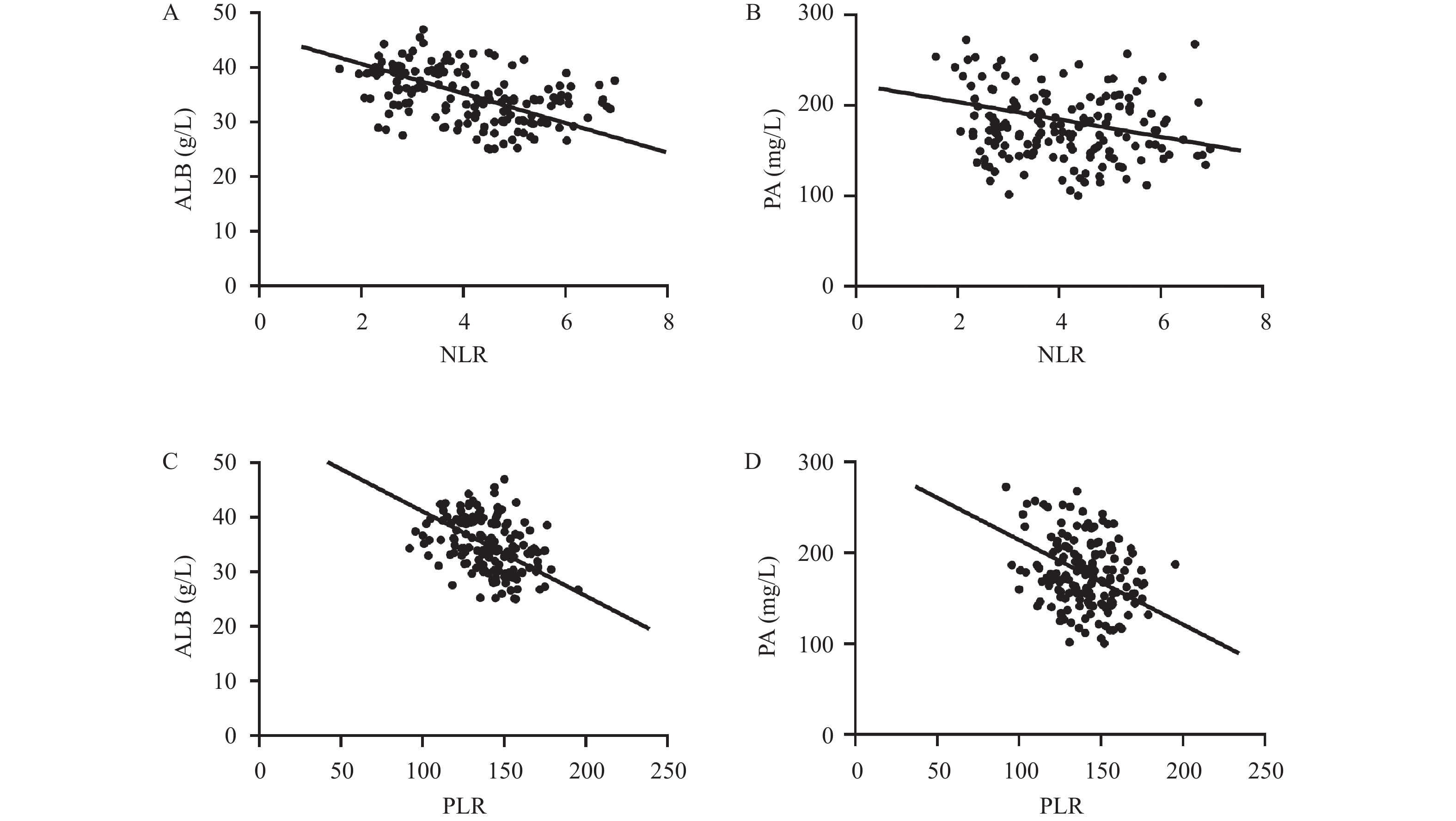
图 1 相关性分析
A:NLR与ALB相关性分析;B:NLR与PA相关性分析;C:PLR与ALB相关性分析;D:PLR与PA相关性分析。
Figure 1. Correlation analysis
表 1 两组患者一般资料比较[($\bar x \pm s $)/n(%)](1)
Table 1. Comparison of general characteristics between the two groups[($\bar x \pm s $)/n(%)](1)
组别 SCOPD组(n = 82) AECOPD组(n = 82) t/χ2 P 年龄(岁) 65.38 ± 7.19 68.76 ± 7.24 3.000 0.003* 性别 0.242 0.623 男 52(63.41) 55(67.07) 女 30(36.59) 27(32.93) 体质量指数(kg/m2) 21.18 ± 1.55 21.04 ± 1.49 0.590 0.556 COPD病程(年) 6.82 ± 2.37 7.04 ± 2.39 0.592 0.555 吸烟史 0.224 0.636 有 45(54.88) 48(58.54) 无 37(45.12) 34(41.46) 基础疾病史 高血压 35(42.68) 38(46.34) 0.222 0.637 糖尿病 18(21.95) 22(26.83) 0.529 0.467 冠心病 15(18.29) 17(20.73) 0.155 0.694  下载: 导出CSV
下载: 导出CSV
表 1 两组患者一般资料比较[($\bar x \pm s $)/n(%)](2)
Table 1. Comparison of general baseline data, pulmonary function and in-hospital intervention characteristics between the two groups[($\bar x \pm s $)/n(%)](2)
组别 SCOPD组(n = 82) AECOPD组(n = 82) t/χ2 P FEV1/FVC 57.34 ± 7.25 53.87 ± 8.96 2.726 0.007* FEV1% pred 51.15 ± 10.48 45.29 ± 11.67 3.383 <0.001* 糖皮质激素使用史 0.415 0.519 有 49(59.76) 53(64.63) 无 33(40.24) 29(35.37) 抗生素使用史 0.402 0.526 有 46(56.10) 50(60.98) 无 36(43.90) 32(39.02) 无创机械通气支持 0.621 0.431 有 14(17.07) 18(21.95) 无 68(82.93) 64(78.05) 个体化营养支持 0.284 0.594 有 20(24.39) 23(28.05) 无 62(75.61) 59(71.95) 高龄本身可导致肺组织弹性减退、呼吸肌力下降,进而使 FEV1/FVC 及 FEV1% pred降低,同时也可能影响 ALB、PA等营养指标水平,上述差异在后续多因素 Logistic 回归分析中已对年龄进行校正以控制混杂偏倚;*P < 0.05。
下载: 导出CSV
表 2 两组患者白细胞比值及营养指标比较($\bar x \pm s $)
Table 2. Comparison of leukocyte ratios and nutritional indicators between the two groups ($\bar x \pm s $)
组别 n NLR PLR ALB(g/L) PA(mg/L) SCOPD组 82 3.20 ± 0.73 127.38 ± 14.22 37.45 ± 5.12 180.36 ± 38.18 AECOPD组 82 5.14 ± 1.15 152.74 ± 20.39 32.18 ± 6.04 167.47 ± 36.29 t 12.900 9.238 6.027 2.216 P <0.001* <0.001* <0.001* 0.028* *P < 0.05。
下载: 导出CSV
表 3 康复良好与不良患者白细胞比值及营养指标比较($\bar x \pm s $)
Table 3. Comparison of leukocyte ratios and nutritional indicators between patients with favorable and unfavorable clinical outcomes ($\bar x \pm s $)
组别 n NLR PLR ALB(g/L) PA(mg/L) 康复良好组 52 4.84 ± 0.72 150.16 ± 15.28 33.25 ± 4.71 172.59 ± 21.24 康复不良组 30 5.67 ± 0.61 157.21 ± 15.90 30.32 ± 5.09 158.60 ± 19.57 t 5.307 2.751 2.634 2.955 P <0.001* 0.007* 0.010* 0.004* *P < 0.05。
下载: 导出CSV
表 4 多因素Logistic回归分析AECOPD患者康复效果影响因素
Table 4. Multivariate Logistic regression analysis of influencing factors for clinical outcomes in patients with AECOPD
影响因素 Β S.E. Wald P OR 95%CI NLR 0.725 0.281 6.657 0.033* 2.066 1.156~3.693 PLR 0.803 0.274 8.589 0.021* 2.233 1.211~4.120 ALB −0.892 0.191 21.837 <0.001* 0.409 0.281~0.595 PA −0.615 0.227 7.358 0.007* 0.542 0.347~0.845 年龄 0.896 0.358 9.756 0.002* 2.449 1.385~4.327 *P < 0.05。
下载: 导出CSV
表 5 短期预后良好与不良患者白细胞比值及营养指标比较($\bar x \pm s $)
Table 5. Comparison of leukocyte ratios and nutritional indicators between patients with good and poor short-term prognosis ($\bar x \pm s $)
组别 n NLR PLR ALB(g/L) PA(mg/L) 短期预后良好组 58 5.02 ± 0.82 150.42 ± 15.73 33.56 ± 5.11 171.74 ± 21.80 短期预后不良组 24 5.43 ± 0.79 158.35 ± 16.09 28.85 ± 5.94 157.15 ± 19.76 t 2.082 2.063 3.619 2.831 P 0.041* 0.042* <0.001* 0.006* *P < 0.05。
下载: 导出CSV
表 6 多因素Logistic回归分析AECOPD患者短期预后的影响因素
Table 6. Multivariate Logistic regression analysis of influencing factors for short-term prognosis in patients with AECOPD
影响因素 Β S.E. Wald P OR 95%CI NLR 0.945 0.312 9.174 0.020* 2.574 1.153~5.750 PLR 1.084 0.324 11.194 <0.001* 2.959 1.134~7.721 ALB −0.872 0.215 16.425 <0.001* 0.418 0.276~0.632 PA −0.643 0.234 7.592 0.006* 0.526 0.332~0.834 年龄 0.863 0.364 8.924 0.003* 2.370 1.351~4.158 *P < 0.05。
下载: 导出CSV
-
[1] 徐贤彪, 杨明芳, 李瑞丹, 等. 慢性阻塞性肺疾病急性加重期患者并发呼吸道合胞病毒感染的影响因素及与血清HSP70、KLF5、MIP-2水平的相关性[J]. 昆明医科大学学报, 2025, 46(11): 107-115. [2] Chen X, Liu S, Luo Y, et al. Systemic immune-inflammation index is associated with adverse outcomes in patients hospitalized for AECOPD: A multicenter cohort study[J]. Respiration, 2025, 104(9): 648-666. doi: 10.1159/000545267 [3] Luo L, Tang J, Du X, et al. Chronic obstructive pulmonary disease and the airway microbiome: A review for clinicians[J]. Respir Med, 2024, 225: 107586. doi: 10.1016/j.rmed.2024.107586 [4] 游丕荣. 基于血常规白细胞比值的慢阻肺急性加重并发呼吸衰竭预测模型建立及验证[D]. 重庆: 重庆理工大学, 2024. [5] 孔梦影. 免疫球蛋白、NLR、PLR与COPD频繁加重表型及肺功能的相关性研究[D]. 合肥: 安徽医科大学, 2024. [6] 洪小婷, 程文, 张正国. 不同评分工具筛查老年慢性阻塞性肺疾病患者营养风险的价值及与TSF、Alb、PA和Hb的关系[J]. 临床肺科杂志, 2025, 30(4): 581-586. [7] Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2022 report [EB/OL]. (2021-11-15). https://goldcopd.org/gold-reports/. [8] Vittinghoff E, McCulloch C E. Relaxing the rule of ten events per variable in logistic and cox regression[J]. Am J Epidemiol, 2007, 165(6): 710-718. doi: 10.1093/aje/kwk052 [9] Miller M R, Hankinson J, Brusasco V, et al. Standardisation of spirometry[J]. Eur Respir J, 2005, 26(2): 319-338. doi: 10.1183/09031936.05.00034805 [10] 薛会红, 张湘燕, 张程, 等. AECA、VEGF、mMRC评分在慢阻肺疾病中相关性的研究[J]. 贵州医药, 2021, 45(2): 171-173. [11] 陈丽红, 肖曲香. 联合检测WBC、NLR、PLR、NEU%对急性加重期慢阻肺的预测价值[J]. 安徽医专学报, 2025, 24(4): 75-77. [12] Fricker M, Lokwani R. COPD: The role of neutrophils in inflammation, pathophysiology, and as drug targets[J]. Clin Sci, 2025, 139(20): CS20255452. [13] Yao C, Wang L, Shi F, et al. Optimized combination of circulating biomarkers as predictors of prognosis in AECOPD patients complicated with heart failure[J]. Int J Med Sci, 2021, 18(7): 1592-1599. doi: 10.21203/rs.3.rs-28752/v1 [14] 喻瑞, 黎友伦. NLR、PLR及RCI对慢性阻塞性肺疾病严重程度的预测价值[J]. 重庆医学, 2022, 51(11): 1902-1907. [15] Liao Q Q, Mo Y J, Zhu K W, et al. Platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), and eosinophil-to-lymphocyte ratio (ELR) as biomarkers in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD)[J]. Int J Chronic Obstr Pulm Dis, 2024, 19: 501-518. doi: 10.2147/COPD.S447519 [16] Guo J, Zhou L S, Lv X, et al. Mechanisms of LouDan LiFei granule attenuate inflammatory injury in AECOPD: A network pharmacology and experimental validation[J]. Phytomedicine, 2025, 142: 156719. doi: 10.1016/j.phymed.2025.156719 [17] 张森, 卢月梅, 梁松荣. 肺癌合并慢性阻塞性肺疾病营养风险筛查应用及干预效果[J]. 吉林医学, 2023, 44(6): 1631-1633. [18] 杨波, 王勇生, 杨万春. 慢性阻塞性肺疾病患者血清25羟维生素D、骨密度、营养指标变化的相关临床研究[J]. 中国现代医药杂志, 2021, 23(10): 11-15. [19] Wang L, Rui W, Chen S, et al. Effect of enteral and parenteral nutrition support on pulmonary function in elderly patients with chronic obstructive pulmonary disease complicated by respiratory failure[J]. Comput Math Meth Med, 2022, 2022: 4743070. doi: 10.1155/2023/9878450 [20] 吴彩葵, 廖少琼. 白蛋白、血清前白蛋白、胆碱酯酶与脑卒中长期卧床患者营养状况的相关性分析[J]. 中国当代医药, 2025, 32(5): 57-60. [21] Man M A, Rajnoveanu R M, Motoc N S, et al. Neutrophil-to-lymphocyte ratio, platelets-to-lymphocyte ratio, and eosinophils correlation with high-resolution computer tomography severity score in COVID-19 patients[J]. PLoS One, 2021, 16(6): e0252599. doi: 10.1371/journal.pone.0252599 [22] Shao S, Zhang Z, Feng L, et al. Association of blood inflammatory biomarkers with clinical outcomes in patients with AECOPD: An 8-year retrospective study in Beijing[J]. Int J Chronic Obstr Pulm Dis, 2023, 18: 1783-1802. doi: 10.2147/COPD.S416869 [23] 岳杰, 顾玉旗. 循环血PCT、NLR、AGR水平及FEV1%pred与慢阻肺患者急性加重期的关联研究[J]. 辽宁医学杂志, 2024, 38(5): 39-42. [24] Nyman F. Health care of the disadvantaged: Chronic obstructive pulmonary disease in later life[J]. Front Public Health, 2023, 11: 1304494. doi: 10.3389/fpubh.2023.1304494 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 163
- HTML全文浏览量: 100
- PDF下载量: 60
- 被引次数: 0
