

Risk Factors for Acute Symptomatic Seizures in Patients with Viral Encephalitis and Construction of a Predictive Model
-
摘要:
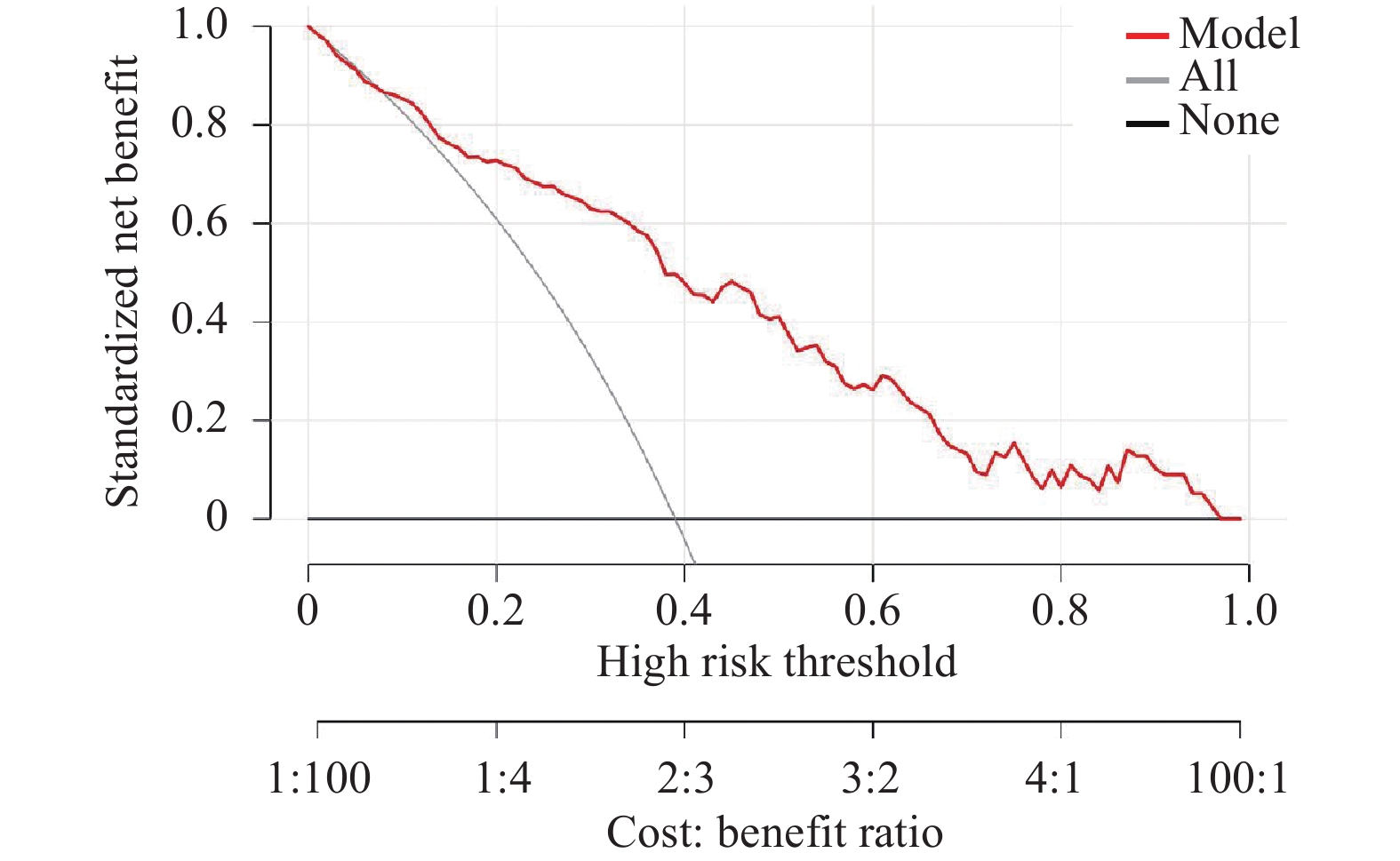
目的 探讨病毒性脑炎(viral encephalitis,VE)患者发生急性症状性癫痫发作(acute symptomatic seizure,ASS)的危险因素,并构建及验证可用于早期识别高危患者的风险预测模型。 方法 采用回顾性队列研究设计,收集2020年1月1日至2023年12月31日昆明医科大学第二附属医院符合纳入、排除标准的249例VE患者作为建模组。以住院期间是否发生ASS为结局指标。对建模组采用单因素Logistic回归初筛后,进一步使用LASSO回归(least absolute shrinkage and selection operator)结合10折交叉验证进行变量筛选,以筛选出的变量构建多因素Logistic回归模型,并基于此构建列线图(Nomogram)预测模型。通过受试者工作特征曲线下面积(area under curve,AUC)、校准曲线和决策曲线分析评估模型的区分度、校准度和临床实用性。另外取2024年1月1日至2024年9月1日昆明医科大学第二附属医院符合纳入、排除标准的60例VE患者作为验证组进行外部验证。 结果 多因素分析显示,血清Na+浓度降低(OR = 0.883,95%CI:0.789~0.989)、额叶或颞叶受累(OR = 2.387,95%CI:1.138~5.007)、EEG中重度异常(中度异常OR = 6.179,95%CI:2.030~18.806;重度异常 OR = 7.875,95%CI:1.081~57.393)及中重度意识障碍(GCS≤12;中度 OR = 4.282,95%CI:1.482~12.378;重度OR = 6.228,95%CI:1.099~35.289)是VE患者发生ASS的独立危险因素。基于此构建的预测模型在建模组的AUC为0.836(95%CI:0.782~0.891,灵敏度0.886,特异度0.565),在验证组的AUC为0.784(95%CI:0.665~0.904,灵敏度0.848,特异度0.711)。建模组Brier评分为0.145,校准斜率为1.023;验证组Brier评分为0.172,校准斜率为0.912。决策曲线分析显示,在阈值概率0.1~0.6范围内,模型获得的净获益均高于“全部干预”和“不干预”策略;当阈值概率处于0.15~0.40时,模型净获益优势最为显著,具有更高的临床决策参考价值。 结论 本研究成功构建并验证了一个包含四个易获临床指标的VE后ASS风险预测模型,该模型具有一定的预测效能,可为临床早期识别高风险患者、实施分层管理与干预提供一种直观、量化的评估工具。 -
关键词:
- 病毒性脑炎 /
- 急性症状性癫痫发作 /
- 危险因素 /
- Nomogram模型
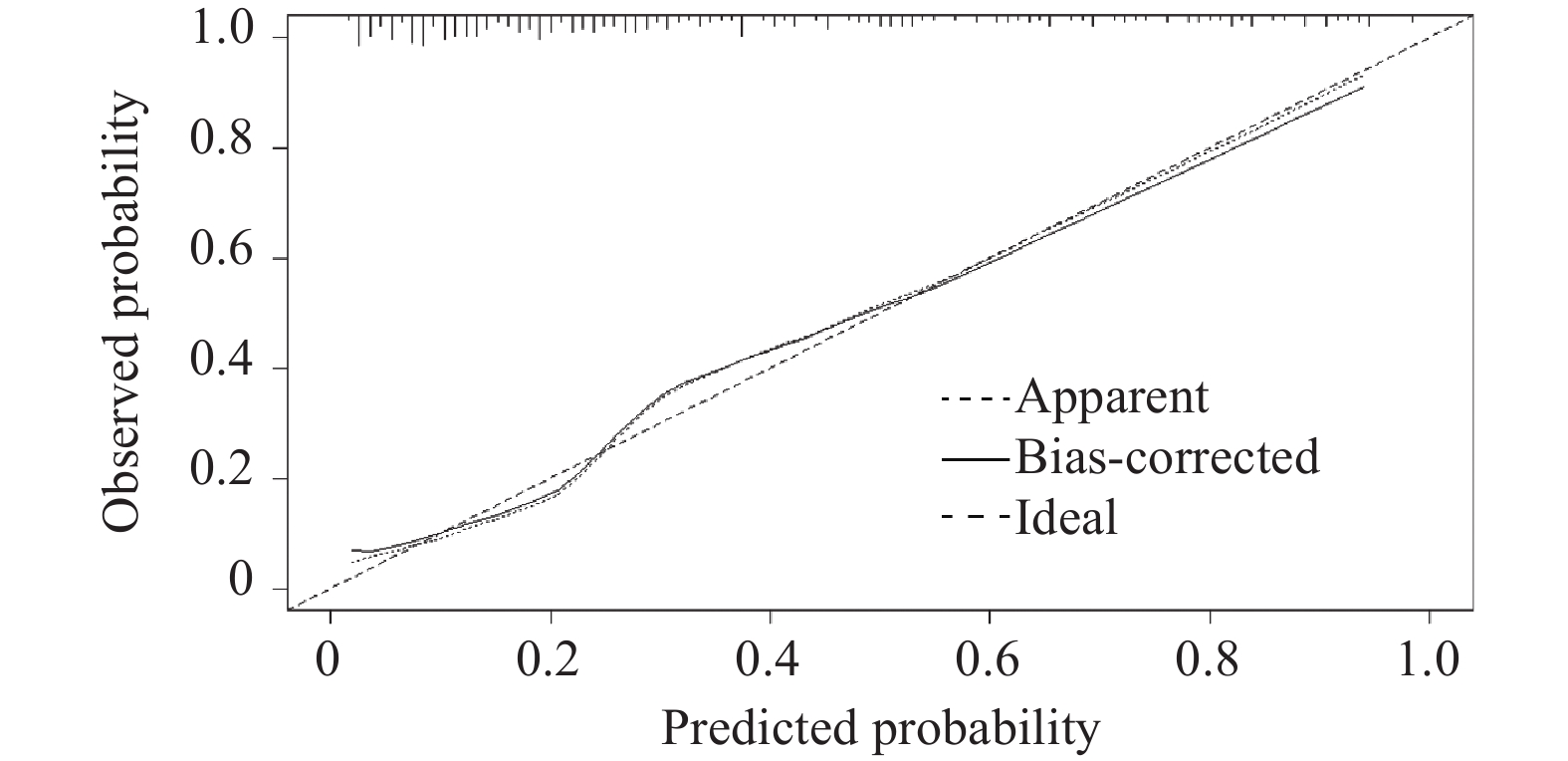
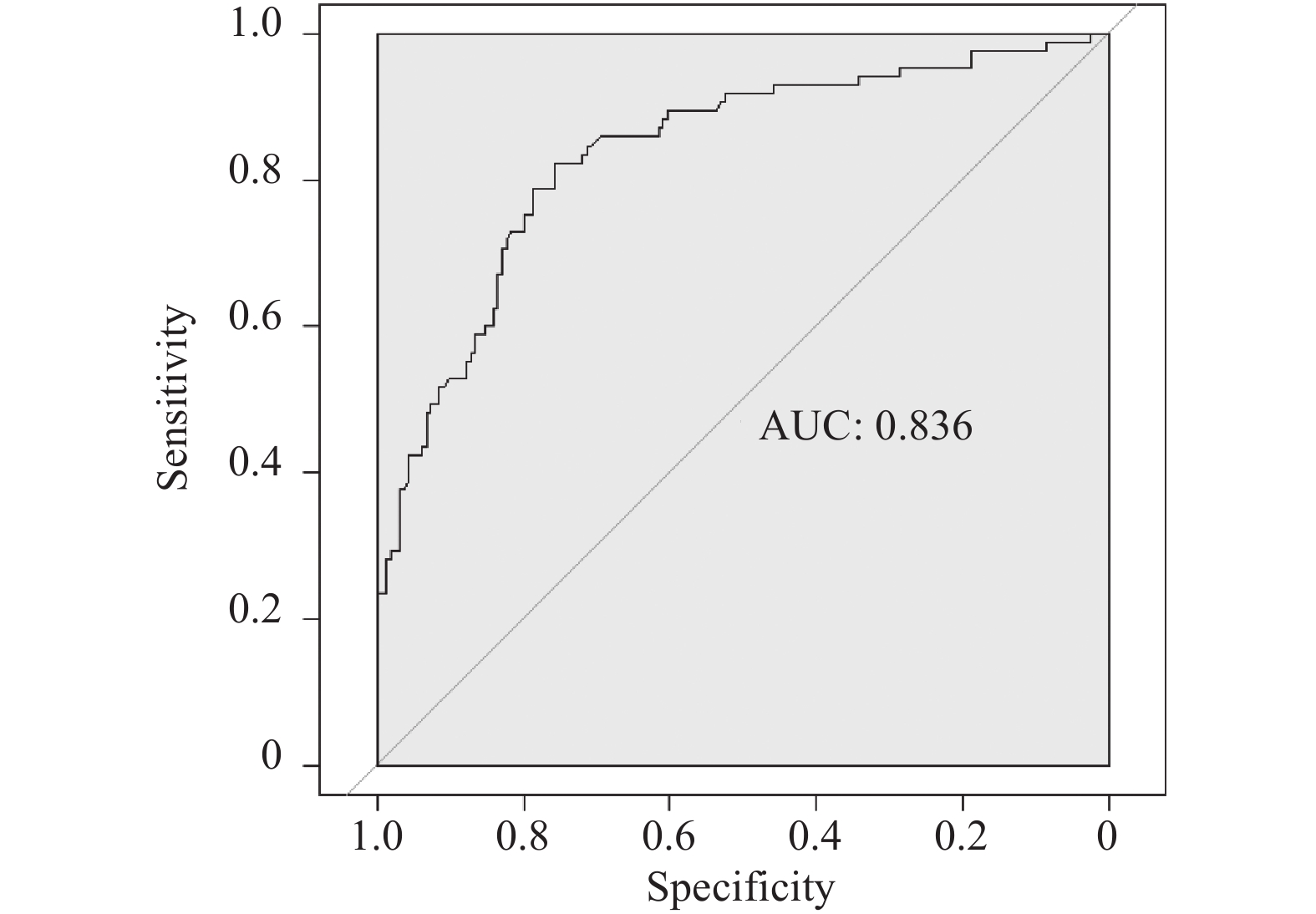
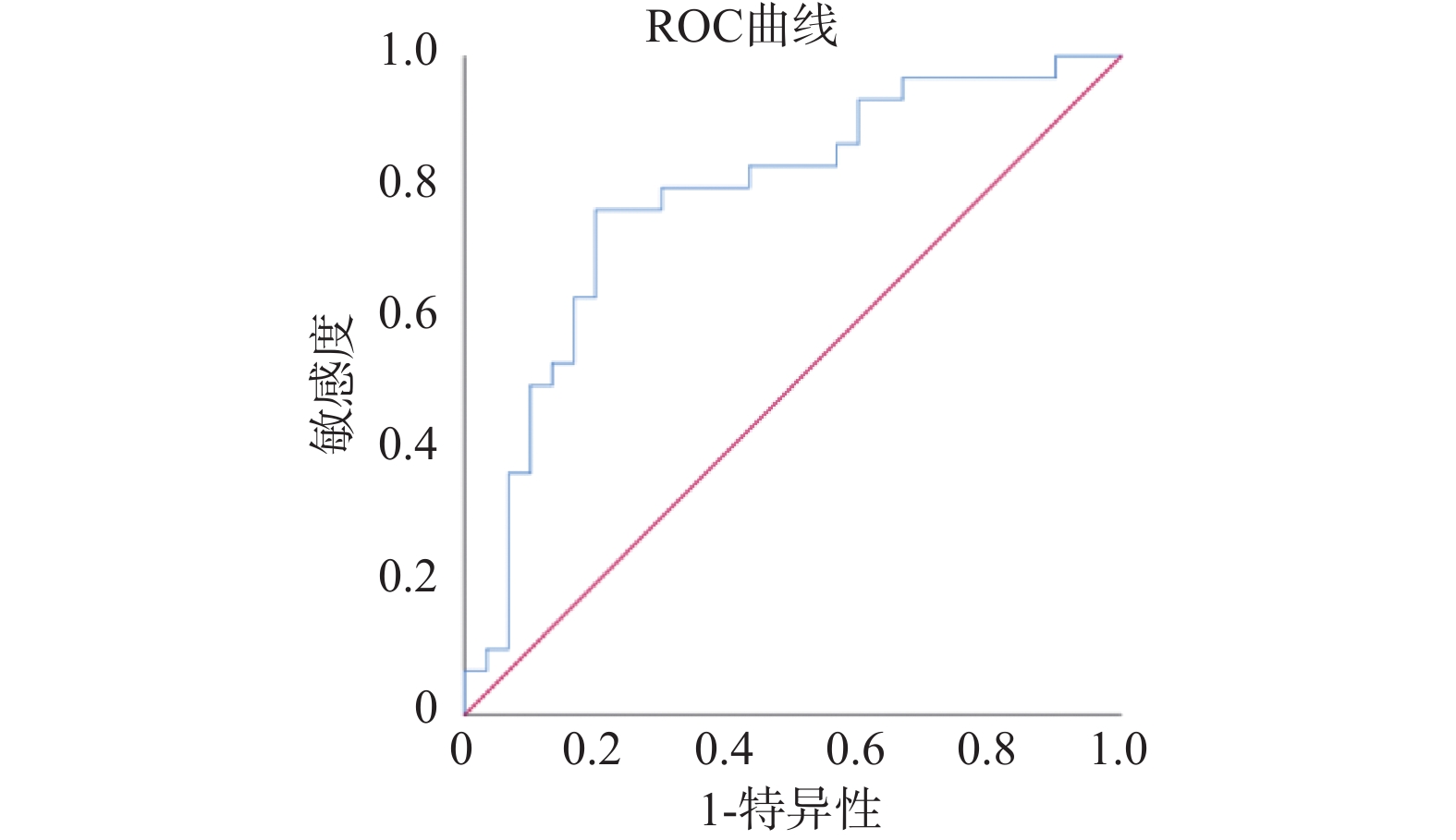
Abstract:Objective To investigate the risk factors for acute symptomatic seizures (ASS) in patients with viral encephalitis (VE), and to construct and validate a risk prediction model for early identification of high-risk patients. Methods A retrospective cohort study design was employed. Data from 249 VE patients admitted to a tertiary hospital in Yunnan Province between January 1, 2020, and December 31, 2023, who met the inclusion and exclusion criteria, were collected as the modeling cohort. The occurrence of ASS during hospitalization was set as the outcome indicator. Univariate logistic regression was used for initial screening of the modeling cohort. Subsequently, LASSO regression (least absolute shrinkage and selection operator) combined with 10-fold cross-validation was applied for variable selection. A multivariable logistic regression model was constructed using the selected variables, and a nomogram prediction model was developed based on this model. The discriminative ability, calibration, and clinical utility of the model were evaluated using the area under the receiver operating characteristic curve (AUC), calibration curve, and decision curve analysis. Additionally, an external validation was performed using 60 VE patients from another tertiary hospital in Yunnan Province between January 1, 2024, and September 1, 2024. Results Multivariate analysis showed that decreased serum sodium concentration (OR = 0.883, 95%CI: 0.789~0.989), frontal or temporal lobe involvement (OR = 2.387, 95%CI: 1.138~5.007), moderate to severe EEG abnormalities (moderate: OR = 6.179, 95%CI: 2.030~18.806; severe: OR = 7.875, 95%CI: 1.081~57.393), and moderate to severe disturbances of consciousness (GCS≤12; moderate: OR = 4.282, 95%CI: 1.482~12.378; severe: OR = 6.228, 95%CI: 1.099~35.289) were independent risk factors for ASS in VE patients. The predictive model constructed based on these factors showed an AUC of 0.836 (95%CI: 0.782~0.891, sensitivity 0.886, specificity 0.565) in the modeling cohort and an AUC of 0.784 (95%CI: 0.665~0.904, sensitivity 0.848, specificity 0.711) in the validation cohort. The Brier score was 0.145 and calibration slope was 1.023 in the modeling cohort; Brier score was 0.172 and calibration slope was 0.912 in the validation cohort. Decision curve analysis demonstrated that within the threshold probability range of 0.1–0.6, the net benefit provided by the model exceeded both the "treat all" and "treat none" strategies. When the threshold probability ranged from 0.15 to 0.40, the model's net benefit advantage was most pronounced, providing higher clinical decision-making value. Conclusion This study successfully established and validated a risk prediction model for ASS following VE that incorporates four readily obtainable clinical indicators. The model demonstrates predictive capability and provides an intuitive, quantitative assessment tool for early clinical identification of high-risk patients and implementation of stratified management and intervention. -
Key words:
- Viral encephalitis /
- Acute symptomatic seizure /
- Risk factors /
- Nomogram model
-
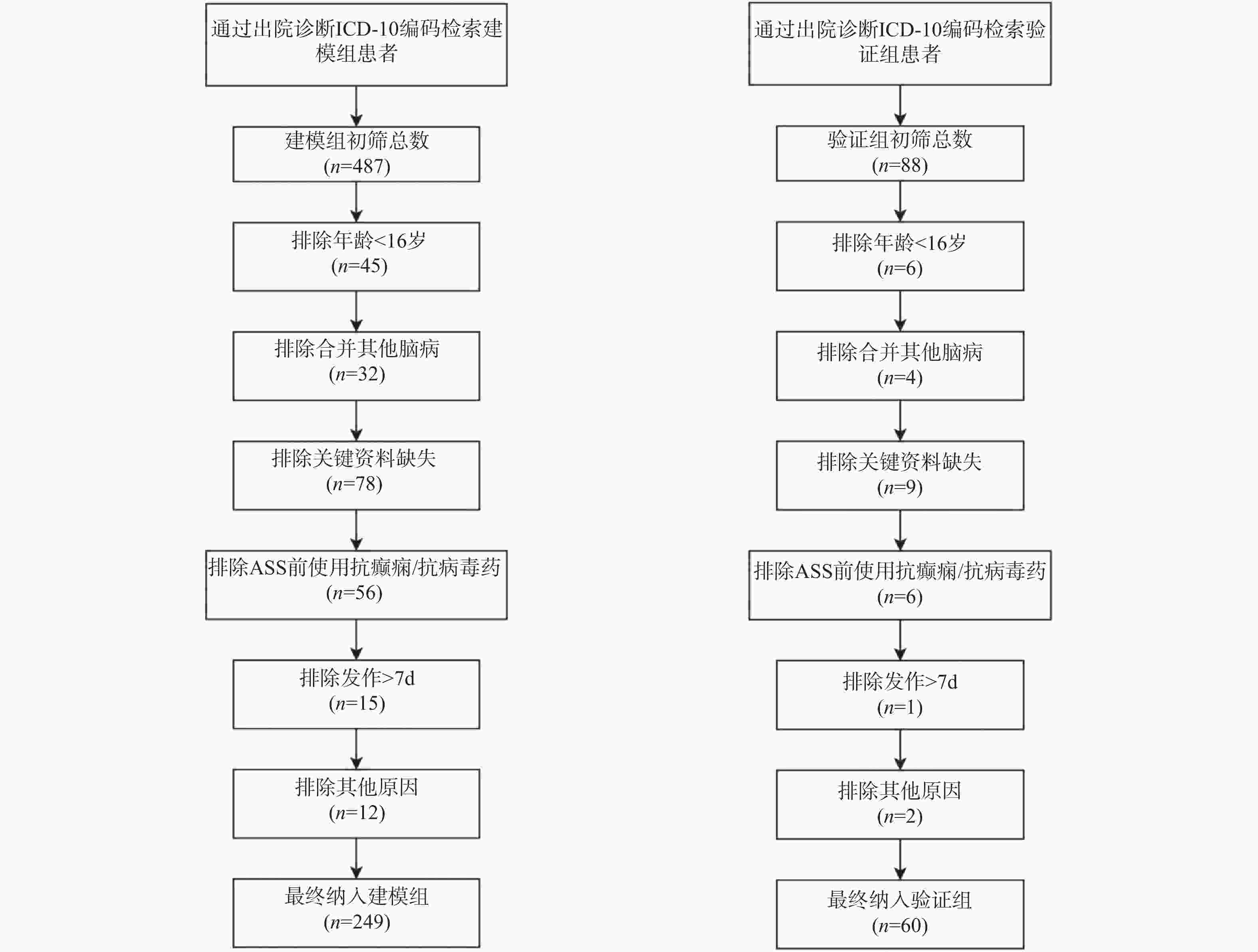
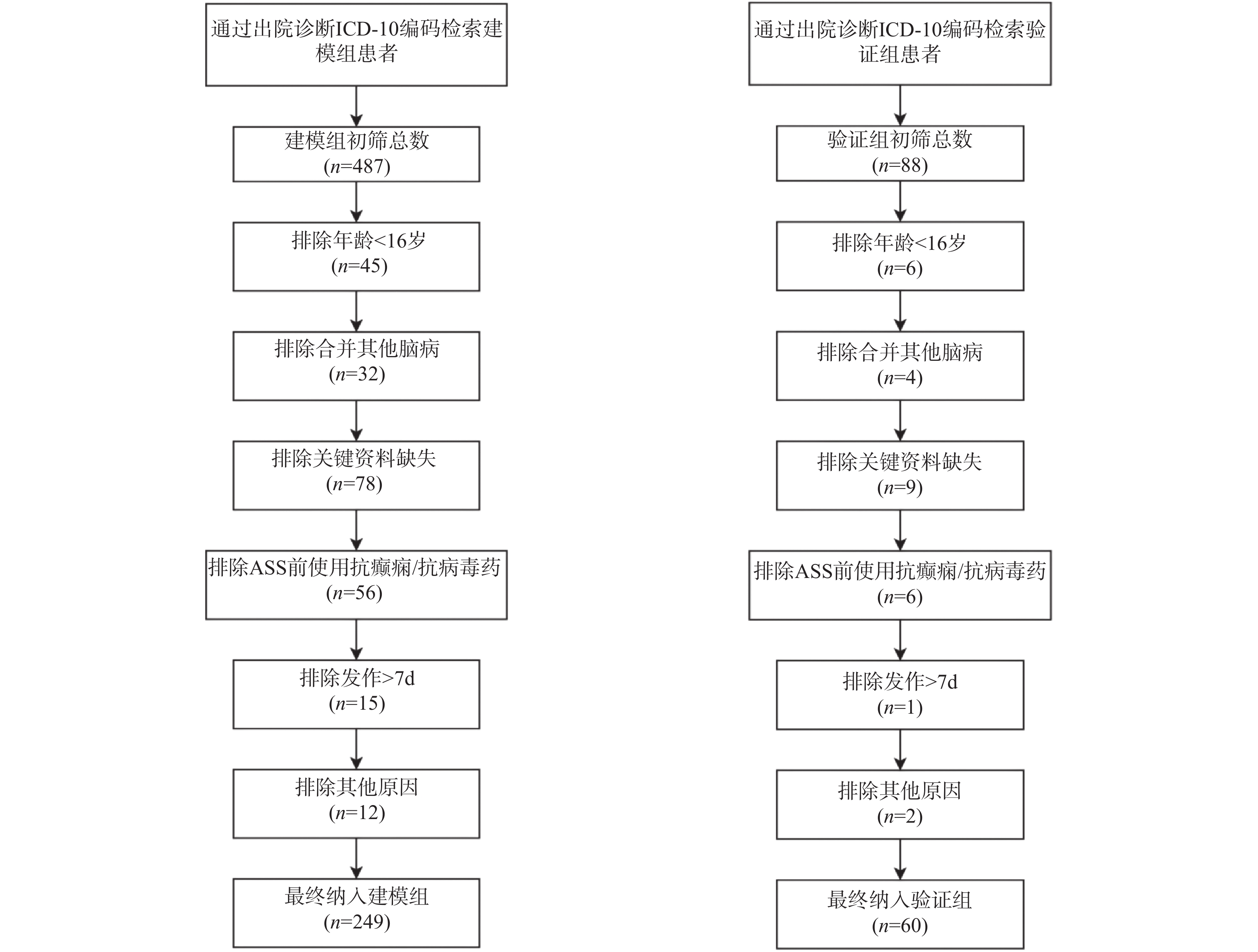
图 1 建模组(左)、验证组(右)筛选流程图
Figure 1. Screening flowchart of the modeling set (left) and validation set(right)
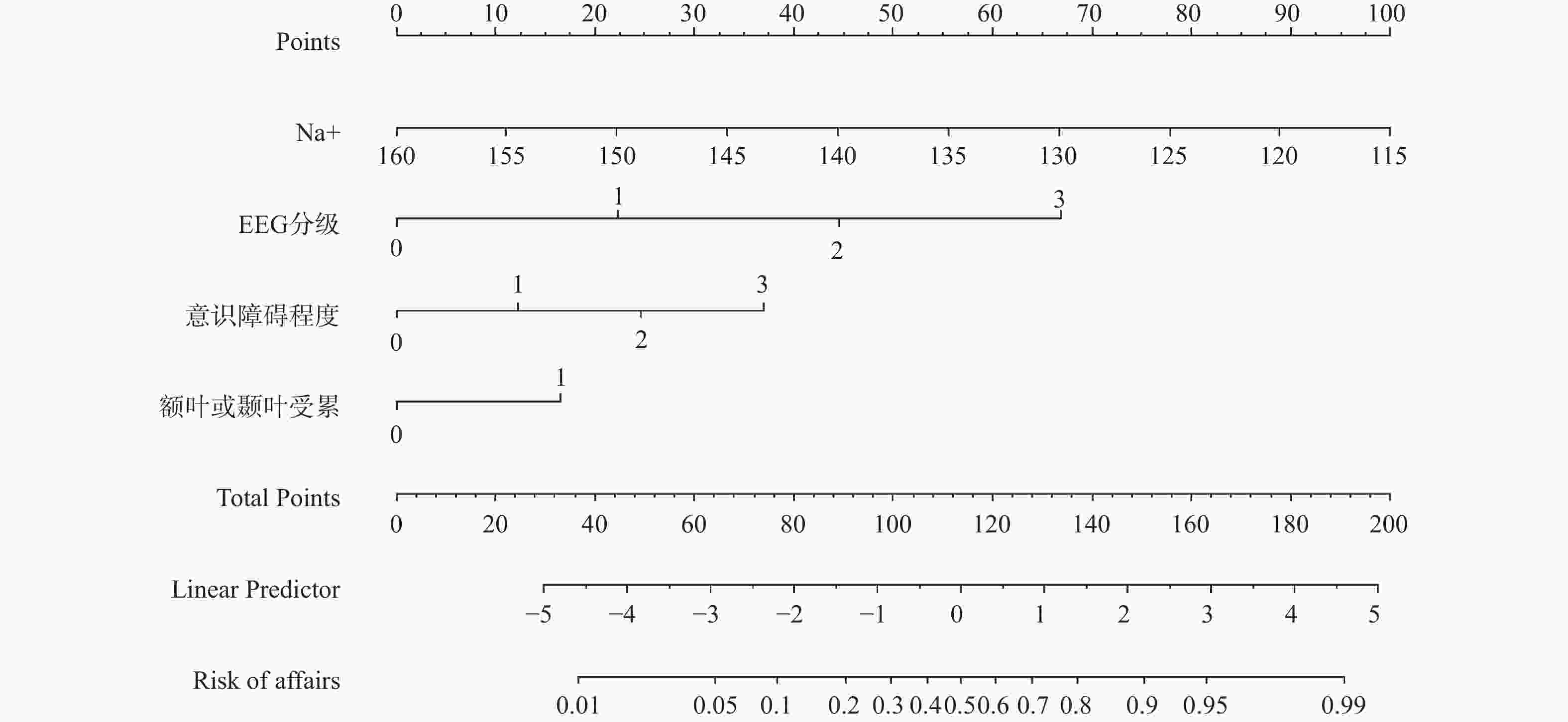
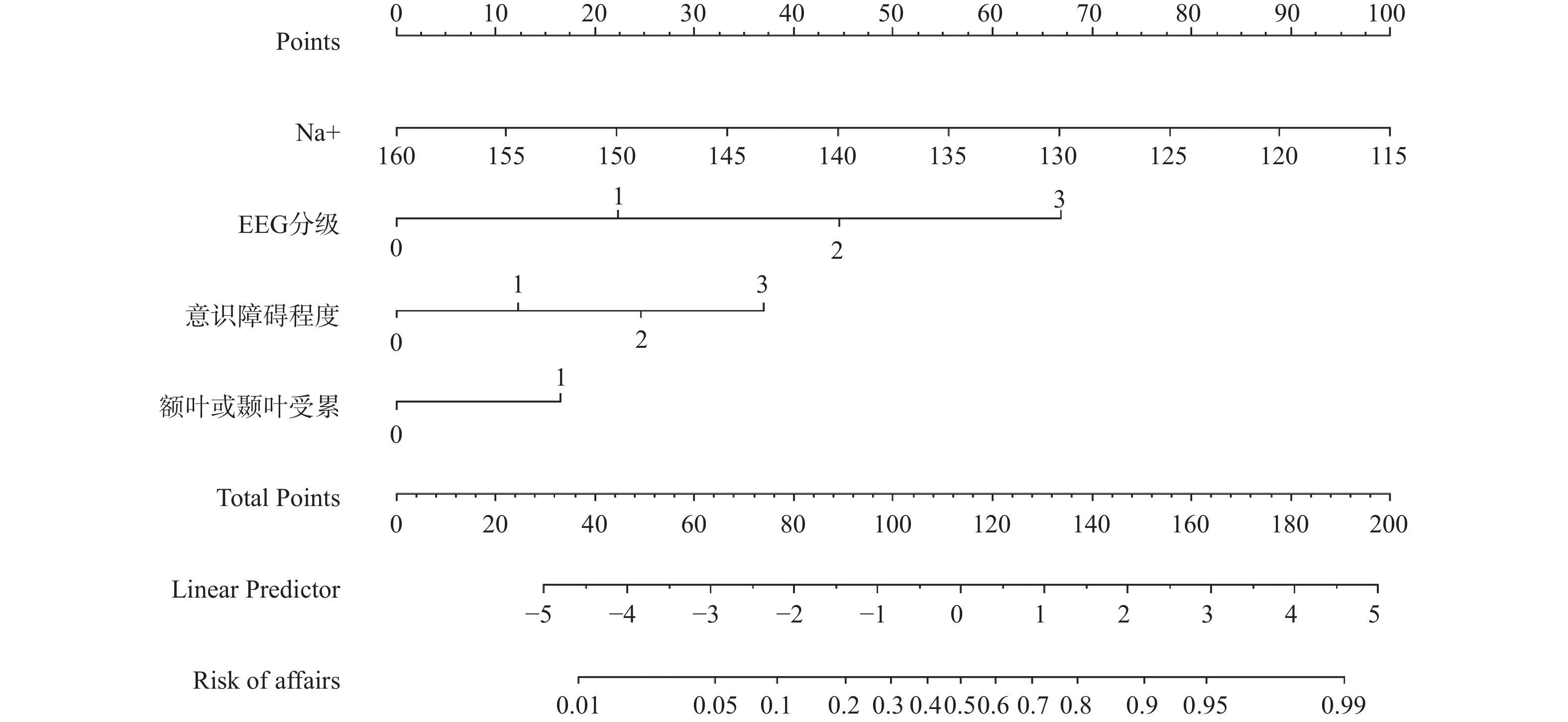
图 2 预测VE患者发生ASS风险的Nomogram模型
注:Na+浓度单位是mmol/L;EEG分级中0代表正常脑电图,1代表轻度异常脑电图,2代表中度异常脑电图,3代表重度异常脑电图;意识障碍程度中0代表意识正常(GCS=15),1代表轻度意识障碍(GCS=13~14),2代表中度意识障碍(GCS=9~12),3代表重度意识障碍/昏迷(GCS≤8);额叶或颞叶受累中0代表无受累,1代表有受累。
Figure 2. Nomogram for predicting the risk of acute symptomatic seizures (ASS) in patients with viral encephalitis (VE)
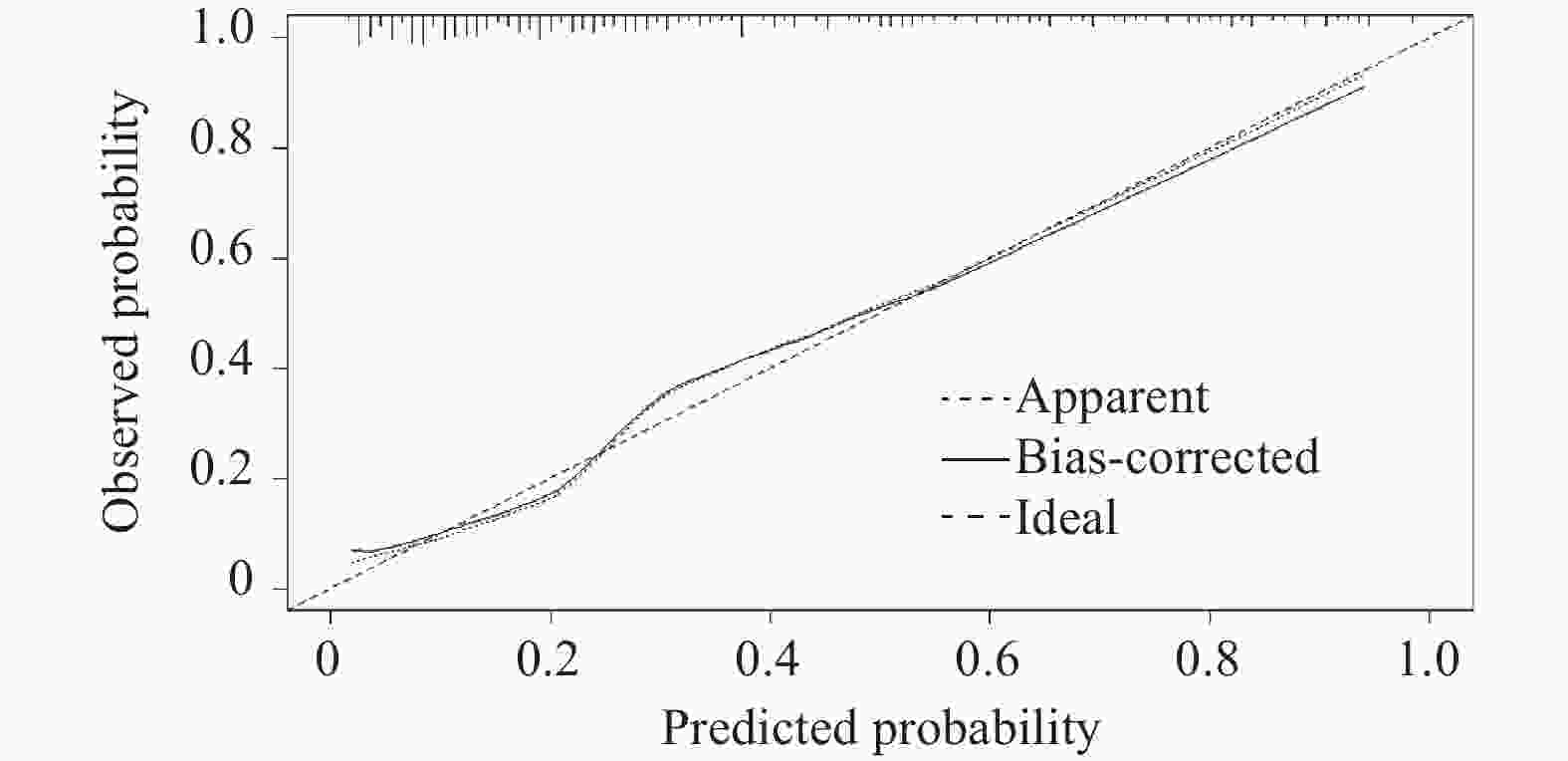
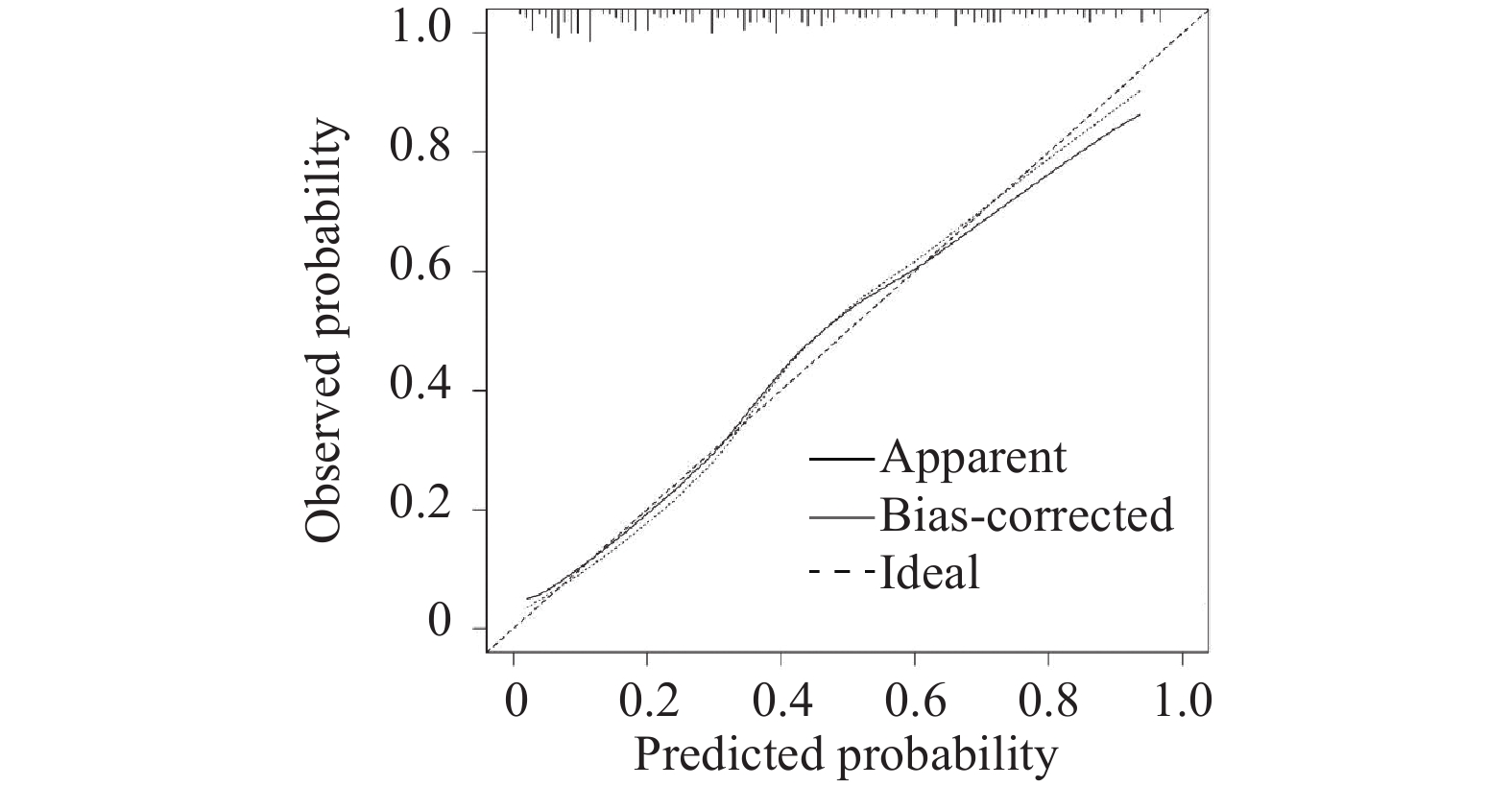
图 3 建模组Nomogram模型校准曲线图
Figure 3. Calibration curve of the nomogram in the modeling set
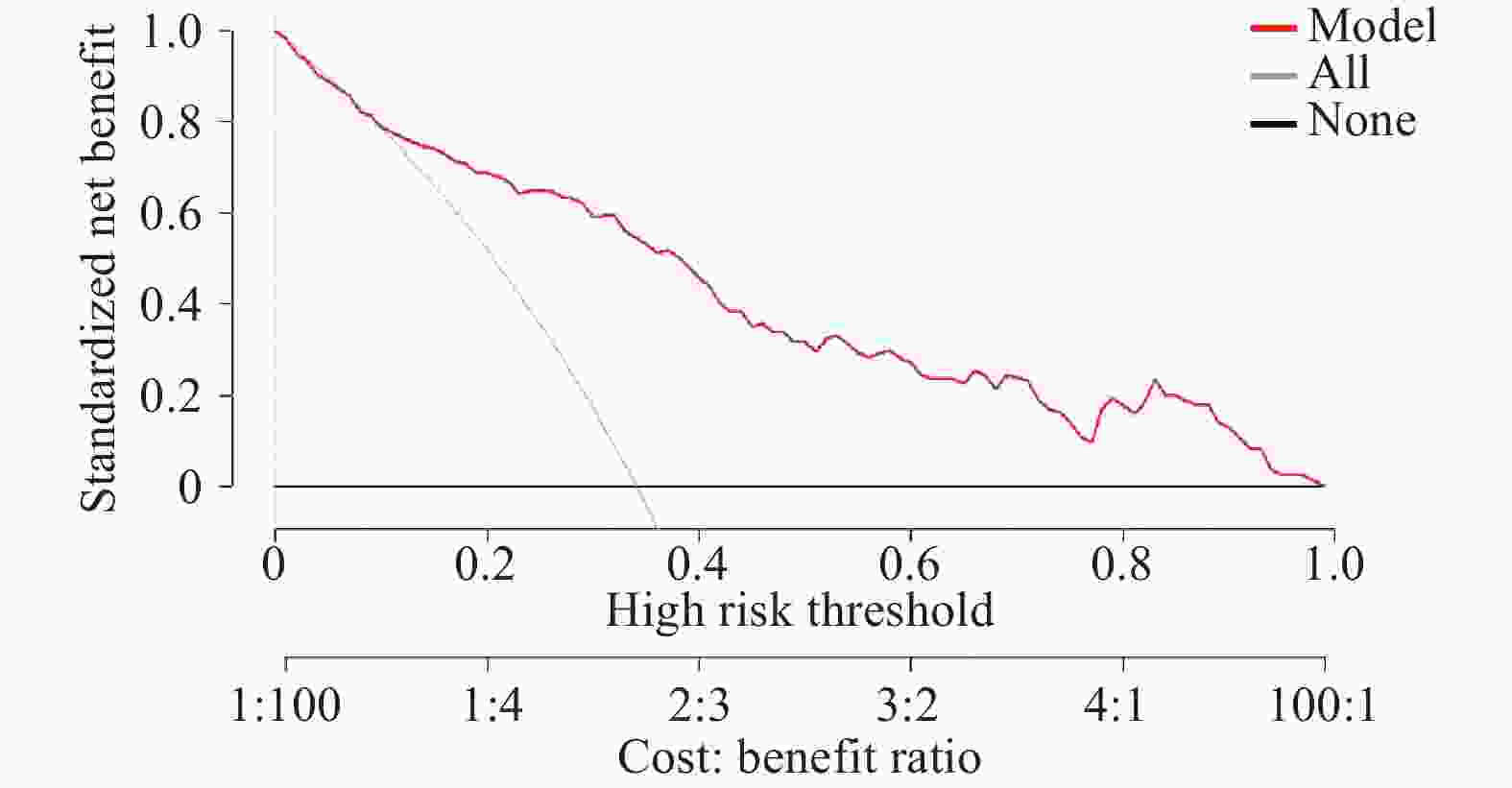
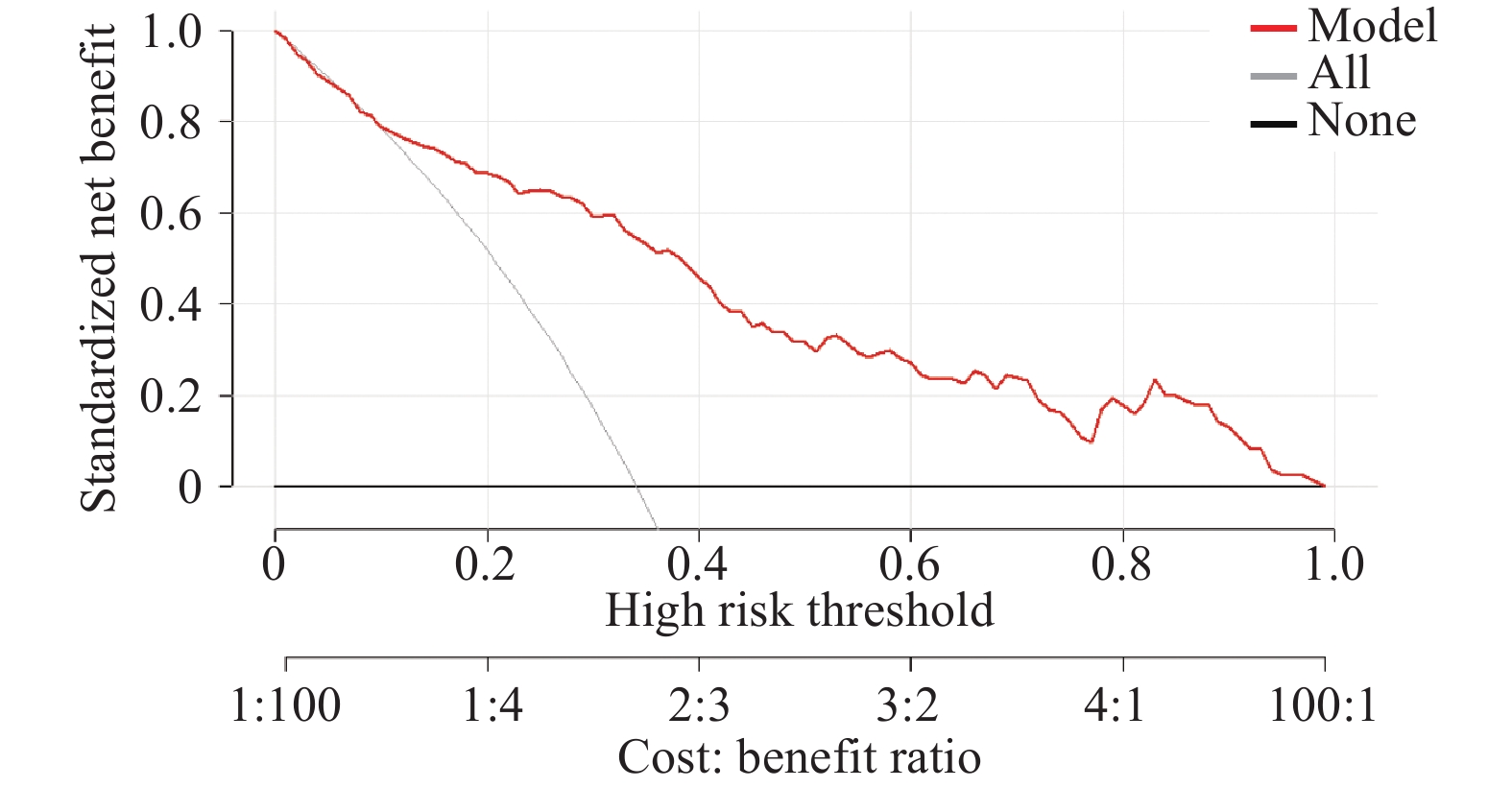
图 5 建模组Nomogram模型的决策曲线图
Figure 5. Decision curve analysis (DCA) of the nomogram in the modeling set
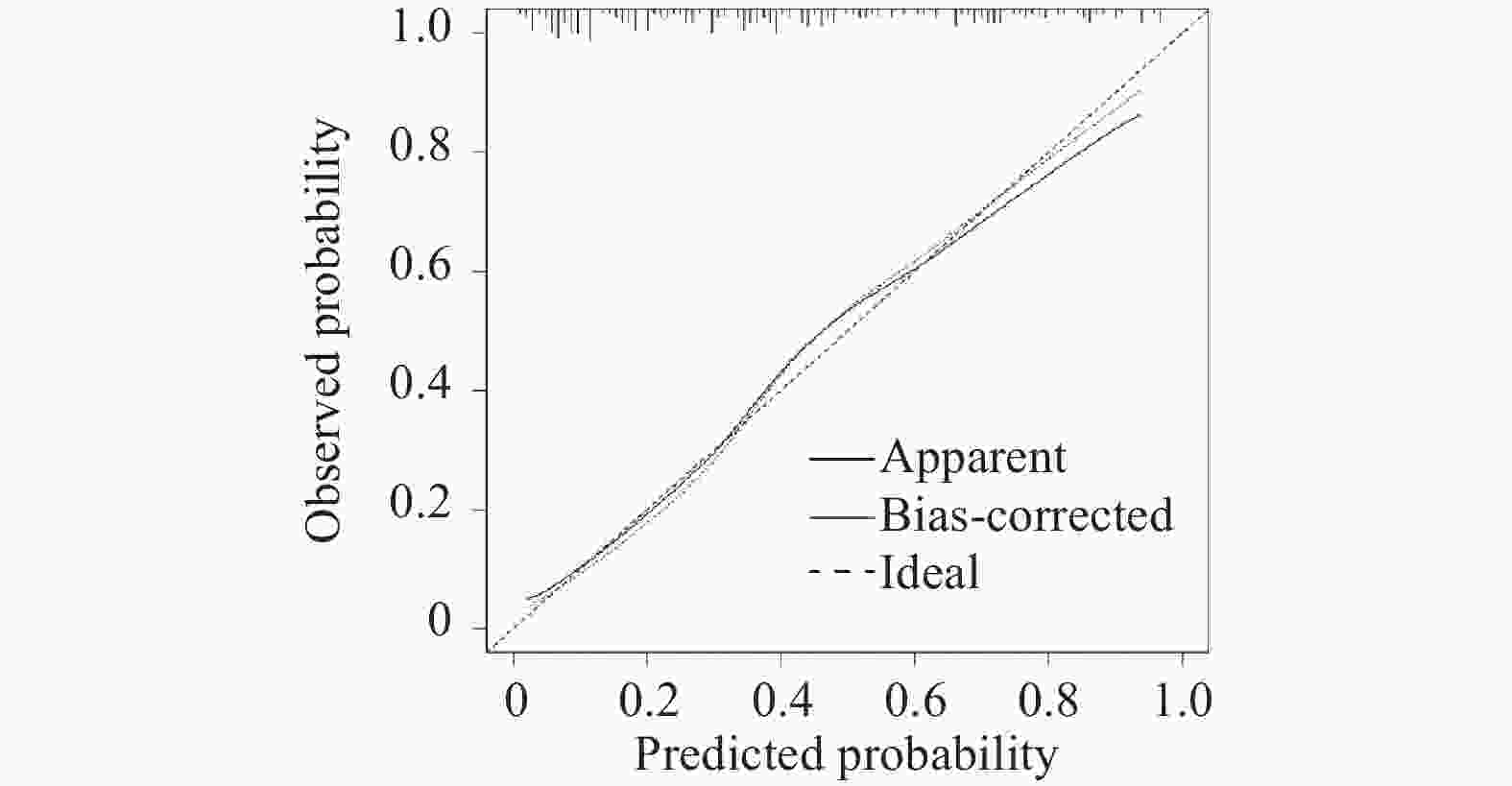
图 6 验证组的Nomogram模型校准曲线图
Figure 6. Calibration curve of the nomogram in the validation set
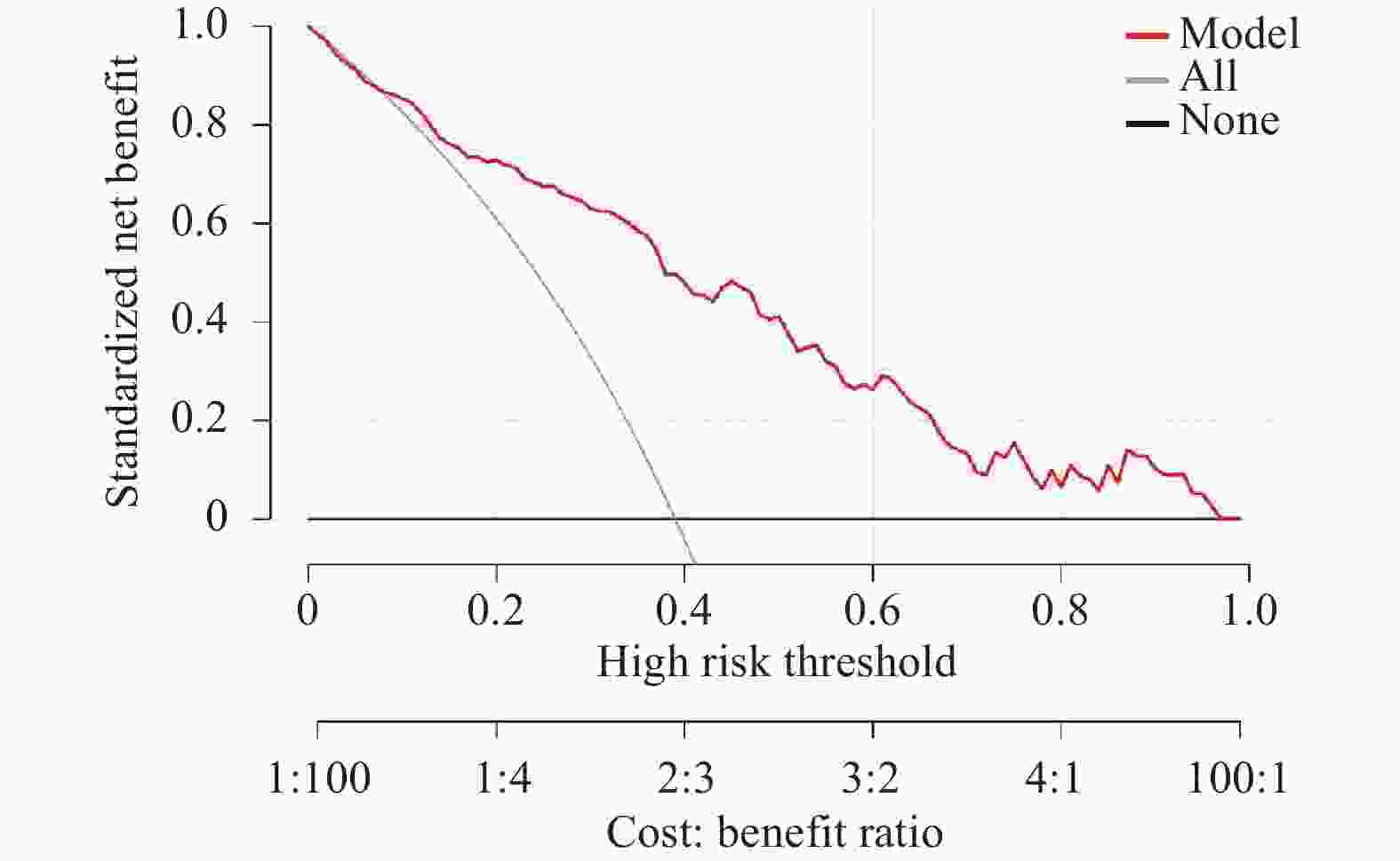
图 8 验证组的Nomogram模型决策曲线图
Figure 8. Decision curve analysis (DCA) of the nomogram in the validation set
表 2 建模组与验证组患者的基线特征比较[n(%)/($ \bar x \pm s $)/M(P25,P75)]
Table 2. Comparison of baseline characteristics between the modeling and validation sets[n(%)/($ \bar x \pm s $)/M(P25,P75)]
变量 建模组(n = 249) 验证组 (n = 60) P 年龄(岁) 42.5 ± 15.2 43.1 ± 14.8 0.782 男性 142 (57.0) 34 (56.7) 0.963 血清Na+(mmol/L) 138 (135,140) 137 (134,140) 0.612 额颞叶受累 98 (39.4) 24 (40.0) 0.928 中重度脑电图异常 113 (45.4) 26 (43.3) 0.781 中重度意识障碍 126 (50.6) 31 (51.7) 0.887 ASS发生率 85 (34.1) 20 (33.3) 0.90  下载: 导出CSV
下载: 导出CSV
表 1 VE发生ASS独立影响因素分析
Table 1. Analysis of independent risk factors for ASS in VE patients
项目 单因素 多因素 OR(95%CI) P OR(95%CI) P 有局灶性神经功能缺损 2.162(1.041,4.491) 0.039* 1.621(0.573,4.583) 0.363 有精神行为异常 6.810(2.880,16.099) <0.001* 2.047(0.539,7.772) 0.292 海马区受累 4.816(1.213,19.130) 0.025* 1.462(0.208,10.262) 0.703 天门冬氨酸转移酶(U/L) 1.008(1.001,1.016) 0.034* 1.003(0.993,1.013) 0.621 尿酸(umol/L) 1.003(1.001,1.004) 0.013* 1.003(1.000,1.006) 0.068 空腹血糖(mmol/L) 1.138(1.035,1.250) 0.007* 1.081(0.952,1.228) 0.23 K+浓度(mmol/L) 0.529(0.288,0.969) 0.039* 1.088(0.464,2.553) 0.847 Na+浓度(mmol/L) 0.884(0.821,0.952) 0.001* 0.883(0.789,0.989) 0.032* 血小板计数(×109/L) 0.996(0.993,1.000) 0.029* 0.996(0.991,1.002) 0.162 白细胞计数(×109/L) 1.146(1.050,1.250) 0.002* 1.024(0.892,1.177) 0.735 中性粒细胞计数(×109/L) 1.003(1.001,1.004) 0.013* 1.032(0.985,1.081) 0.187 额叶或颞叶受累 3.101(1.789,5.374) <0.001* 2.387(1.138,5.007) 0.021* 脑电图异常分级正常脑电图为参照 轻度异常脑电图 1.033(0.379,2.818) 0.949* 0.688(0.217,2.178) 0.525* 中度异常脑电图 6.889(2.598,18.266) <0.001* 6.179(2.030,18.806) 0.001* 重度异常脑电图 31.000(5.477,175.473) <0.001* 7.875(1.081,57.393) 0.042* 意识障碍程度意识正常(GCS=15)为参照 轻度意识障碍(GCS=13~14) 10.114(2.898,35.297) <0.001* 2.081(0.929,4.661) 0.075 中度意识障碍(GCS=9~12) 4.045(1.838,8.903) 0.001* 4.282(1.482,12.378) 0.007* 重度意识障碍(GCS≤8) 2.645(1.400,4.997) 0.003* 6.228(1.099,35.289) 0.039* *P < 0.05。
下载: 导出CSV
-
[1] Gundamraj V, Hasbun R. Viral meningitis and encephalitis: An update[J]. Curr Opin Infect Dis, 2023, 36(3): 177-185. doi: 10.1097/QCO.0000000000000922 [2] Mauritz M, Hirsch L J, Camfield P, et al. Acute symptomatic seizures: An educational, evidence-based review[J]. Epileptic Disord, 2022, 24(1): 26-49. doi: 10.1684/epd.2021.1376 [3] Beghi E, Carpio A, Forsgren L, et al. Recommendation for a definition of acute symptomatic seizure[J]. Epilepsia, 2010, 51(4): 671-675. doi: 10.1111/j.1528-1167.2009.02285.x [4] 马海燕, 张燕芳, 狄晴. 病毒性脑炎后癫痫的预后及其影响因素[J]. 临床神经病学杂志, 2016, 29(2): 120-123. [5] Löscher W, Howe C L. Molecular mechanisms in the genesis of seizures and epilepsy associated with viral infection[J]. Front Mol Neurosci, 2022, 15: 870868. doi: 10.3389/fnmol.2022.870868 [6] 吕海生. 儿童病毒性脑炎急性期发生症状性癫痫的相关因素分析[J]. 中国处方药, 2017, 15(5): 117-118. [7] 中华医学会. 临床诊疗指南-神经病学分册[M]. 北京: 人民卫生出版社, 2006: 24-29. [8] 刘晓燕. 临床脑电图学[M]. 2版. 北京: 人民卫生出版社, 2017: 87-88. [9] Fisher R S, Acevedo C, Arzimanoglou A, et al. ILAE Official Report: A practical clinical definition of epilepsy[J]. Epilepsia, 2014, 55(4): 475-482. doi: 10.1111/epi.12550 [10] Sellner J, Trinka E. Seizures and epilepsy in herpes simplex virus encephalitis: Current concepts and future directions of pathogenesis and management[J]. J Neurol, 2012, 259(10): 2019-2030. doi: 10.1007/s00415-012-6494-6 [11] Lim A K H, Paramaswaran S, Jellie L J, et al. A cross-sectional study of hyponatremia associated with acute central nervous system infections[J]. J Clin Med, 2019, 8(11): 1801. doi: 10.3390/jcm8111801 [12] Nardone R, Brigo F, Trinka E. Acute symptomatic seizures caused by electrolyte disturbances[J]. J Clin Neurol, 2016, 12(1): 21-33. doi: 10.3988/jcn.2016.12.1.21 [13] Sutton F, Barca D, Komoltsev I, et al. Testing blood and CSF in people with epilepsy: A practical guide[J]. Epileptic Disord, 2020, 22(4): 381-398. doi: 10.1684/epd.2020.1191 [14] 张高瓒. 继发于自身免疫性脑炎的急性症状性癫痫发作危险因素分析及列线图模型的构建[D]. 长春: 吉林大学, 2024. [15] Bonini F, McGonigal A, Trébuchon A, et al. Frontal lobe seizures: From clinical semiology to localization[J]. Epilepsia, 2014, 55(2): 264-277. doi: 10.1111/epi.12490 [16] Henning O, Heuser K, Larsen V S, et al. Temporal lobe epilepsy[J]. Tidsskriftet, 2023, 143(2): 10.4045. doi: 10.1093/med/9780199937837.003.0038 [17] Bradshaw M J, Venkatesan A. Herpes simplex virus-1 encephalitis in adults: Pathophysiology, diagnosis, and management[J]. Neurotherapeutics, 2016, 13(3): 493-508. doi: 10.1007/s13311-016-0433-7 [18] Theodore W H. Epilepsy and viral infections: Epilepsy and viral infections[J]. Epilepsy Curr, 2014, 14(2_suppl): 35-42. doi: 10.5698/1535-7511-14.s2.35 [19] Barker-Haliski M L, Heck T D, Dahle E J, et al. Acute treatment with minocycline, but not valproic acid, improves long-term behavioral outcomes in the Theiler’s virus model of temporal lobe epilepsy[J]. Epilepsia, 2016, 57(12): 1958-1967. doi: 10.1111/epi.13577 [20] Vezzani A, Fujinami R S, White H S, et al. Infections, inflammation and epilepsy[J]. Acta Neuropathol, 2016, 131(2): 211-234. doi: 10.1007/s00401-015-1481-5 [21] Rodriguez Ruiz A, Vlachy J, Lee J W, et al. Association of periodic and rhythmic electroencephalographic patterns with seizures in critically ill patients[J]. JAMA Neurol, 2017, 74(2): 181-188. doi: 10.3410/f.727123033.793545357 [22] Zafar S F, Subramaniam T, Osman G, et al. Electrographic seizures and ictal–interictal continuum (IIC) patterns in critically ill patients[J]. Epilepsy Behav, 2020, 106: 107037. doi: 10.1016/j.yebeh.2020.107037 [23] Jeremić M, Arsenijević M, Jovanović D, et al. Non-convulsive status epilepticus as an initial manifestation of herpes simplex virus encephalitis[J]. Epileptic Disord, 2021, 23(5): 749-753. doi: 10.1684/epd.2021.1320 [24] Wood G K, Babar R, Ellul M A, et al. Acute seizure risk in patients with encephalitis: Development and validation of clinical prediction models from two independent prospective multicentre cohorts[J]. BMJ Neurol Open, 2022, 4(2): e000323. doi: 10.1136/bmjno-2022-000323 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 49
- HTML全文浏览量: 39
- PDF下载量: 40
- 被引次数: 0
