

Risk Factors for Catheter-related Fungal Infections in Burn Patients and Their Correlation with TLR4 and NF-κB
-
摘要:
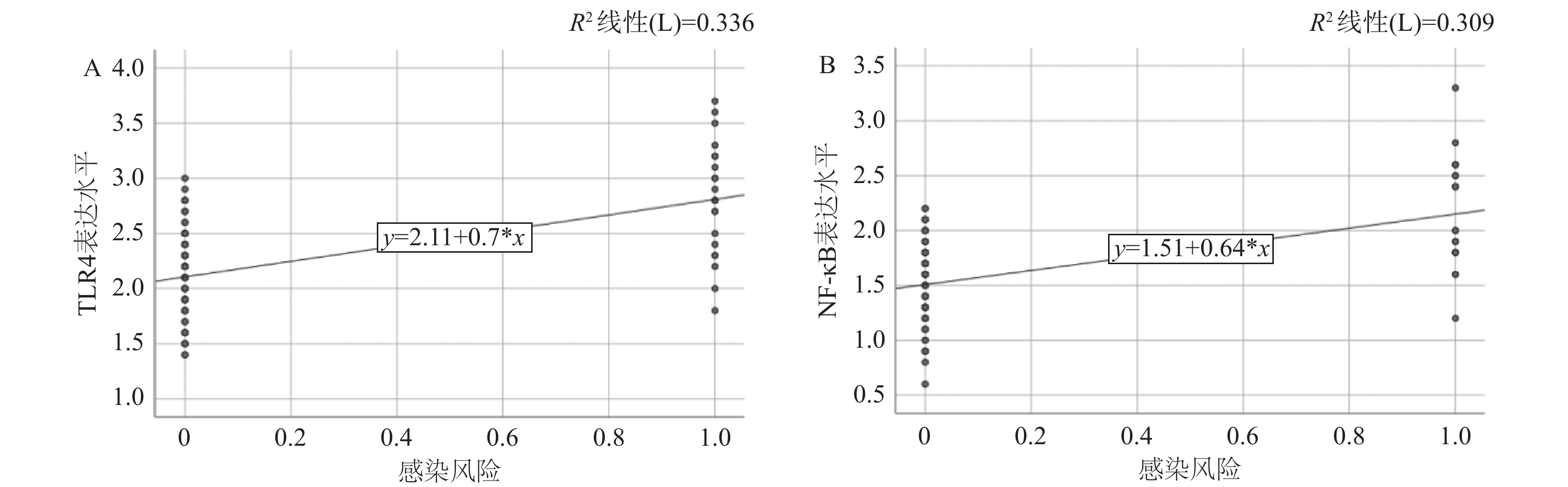
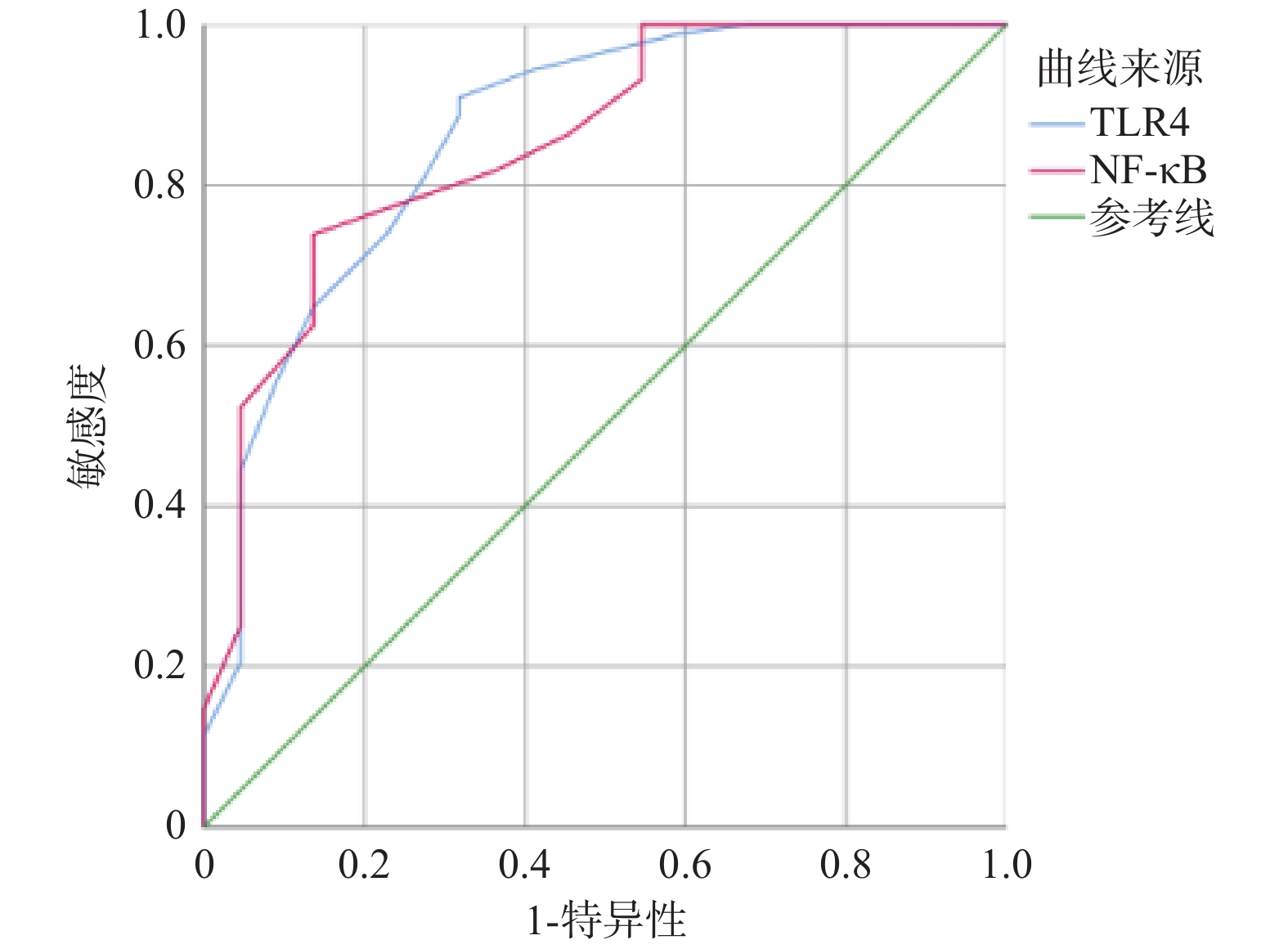
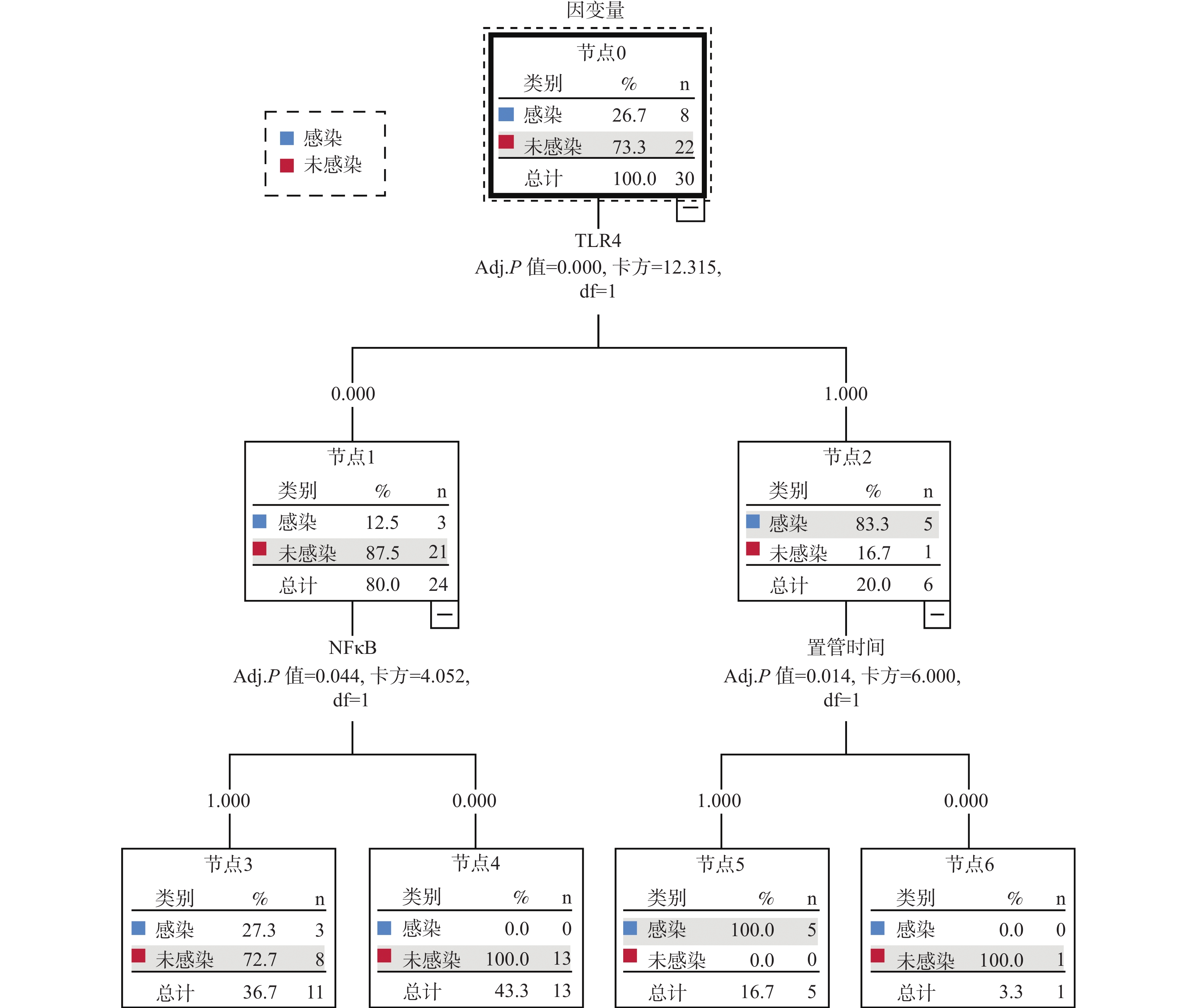
目的 探究烧伤患者导管相关性真菌血流感染的危险因素及其与Toll样受体4(toll-like receptor 4,TLR4),核因子κB(nuclear factor kappa-B,NF-κB)的相关性。 方法 回顾性分析2021年3月至2025年2月间空军军医大学第一附属医院烧伤与皮肤外科收治的110例接受导管置入的烧伤患者临床资料。根据是否发生导管相关性真菌血流感染分为感染组(n = 22)和未感染组(n = 88)。采用Pearson相关系数分析TLR4和NF-κB与烧伤患者导管相关性真菌感染的相关性,绘制ROC曲线取TLR4和NF-κB佳截断值,采用Logistic回归模型分析危险因素,并构建决策树模型。 结果 Pearson相关性分析显示,TLR4和NF-κB均与烧伤患者导管相关性真菌感染呈显著性正相关(r = 0.579,P < 0.001;r = 0.556,P < 0.001)。ROC分析显示,TLR4、NF-κB预测烧伤患者发生导管相关性真菌感染的最佳截断值分别为2.65、1.75。多因素Logistic回归显示,糖尿病、烧伤面积、置管时间、TLR4、NF-κB是烧伤患者导管相关性真菌感染的独立危险因素(P < 0.05)。决策树模型显示:TLR4是最重要的预测因子,模型的分类准确率为90.00%。 结论 糖尿病、烧伤面积、置管时间、TLR4、NF-κB是烧伤患者导管相关性真菌感染的独立危险因素。 Abstract:Objective To investigate the risk factors for catheter-related fungal bloodstream infections in burn patients and their correlation with toll-like receptor 4 (TLR4) and nuclear factor-kappa B (NF-κB). Methods A retrospective analysis was conducted on clinical data of 110 burn patients who underwent catheter placement admitted to the Department of Burns and Plastic Surgery, First Affiliated Hospital of Air Force Medical University from March 2021 to February 2025. Patients were divided into infection group (n = 22) and non-infection group (n = 88) based on whether catheter-related fungal bloodstream infection occurred. Pearson correlation coefficient analysis was used to analyze the correlation between TLR4 and NF-κB and catheter-related fungal infection in burn patients. ROC curve were constructed to determine optimal cutoff values for TLR4 and NF-κB. Logistic regression model was used to analyze the risk factors and a decision tree model was established. Results Pearson correlation analysis showed that both TLR4 and NF-κB were positively correlated with catheter-related fungal infection in burn patients (r = 0.579, P < 0.001; r = 0.556, P < 0.001). ROC analysis showed that the optimal cut-off values of TLR4 and NF-κB for predicting catheter-related fungal infection in burn patients were 2.65 and 1.75, respectively. Multivariate Logistic regression analysis showed that diabetes mellitus, burn area, catheterization duration, TLR4 and NF-κB were independent risk factors for catheter-related fungal infection in burn patients (P < 0.05). Decision tree modeling revealed that TLR4 was the most important predictor, with a classification accuracy rate of 90.00%. Conclusion Diabetes, burn area, catheterization duration, TLR4, and NF-κB are independent risk factors for catheter-related fungal infections in burn patients. -
Key words:
- Burns /
- Catheter-related fungal infection /
- Prevention /
- Risk factors /
- Toll-like receptor 4 /
- Nuclear factor-kappa B
-
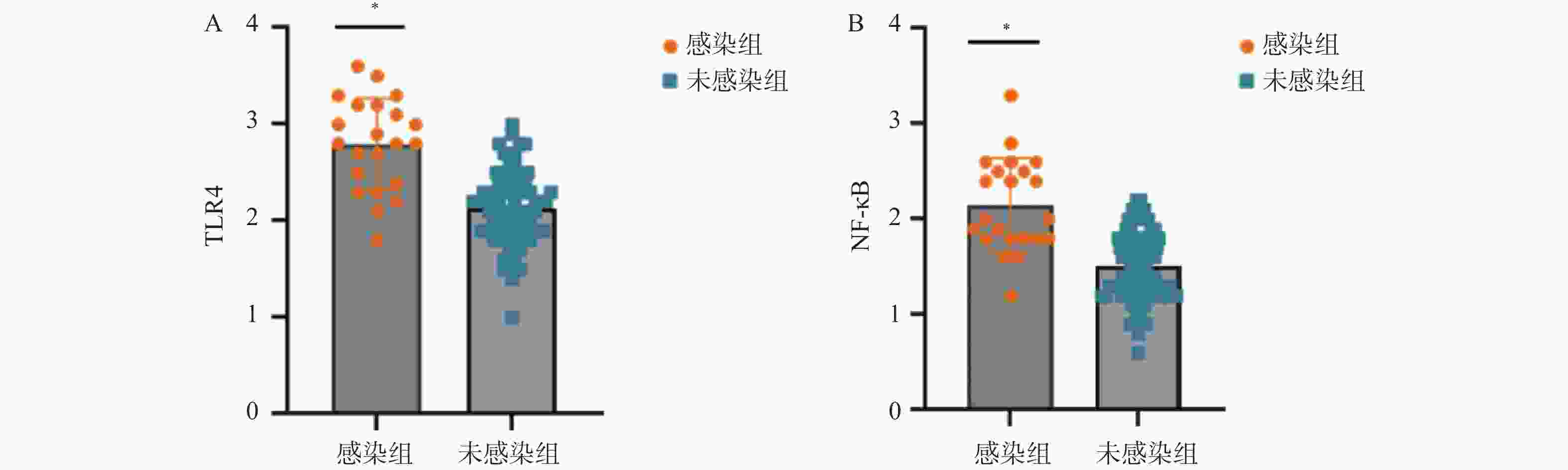
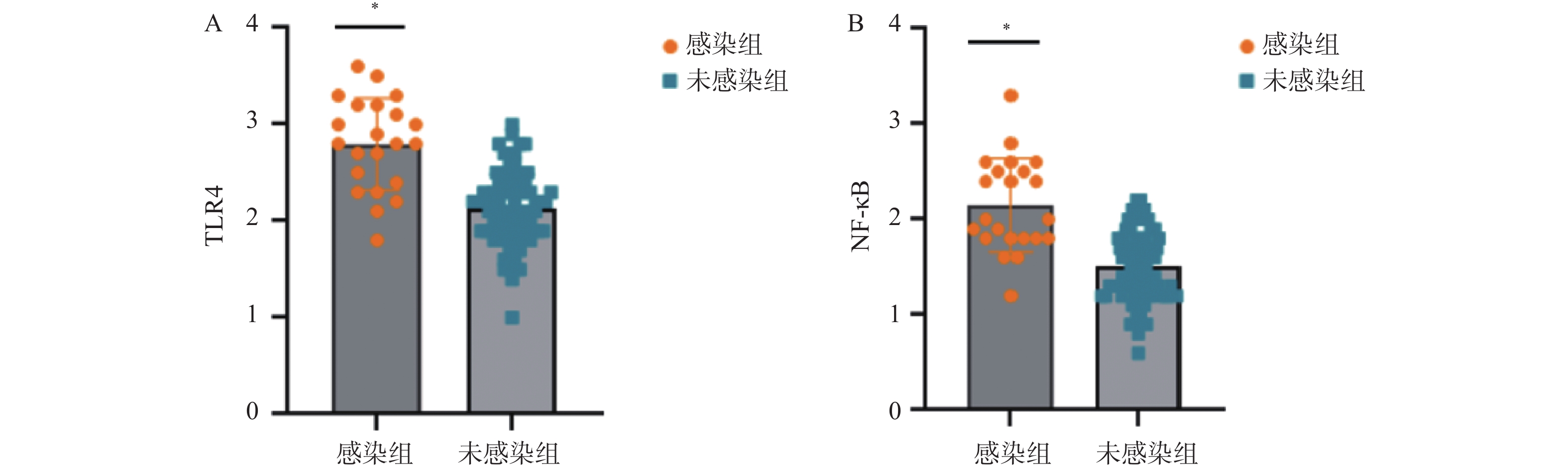
图 2 两组TLR4、NF-κB表达水平
A:两组TLR4表达水平对比;B:两组NF-κB表达水平对比;*P < 0.05。
Figure 2. TLR4 and NF-κB expression levels in two groups
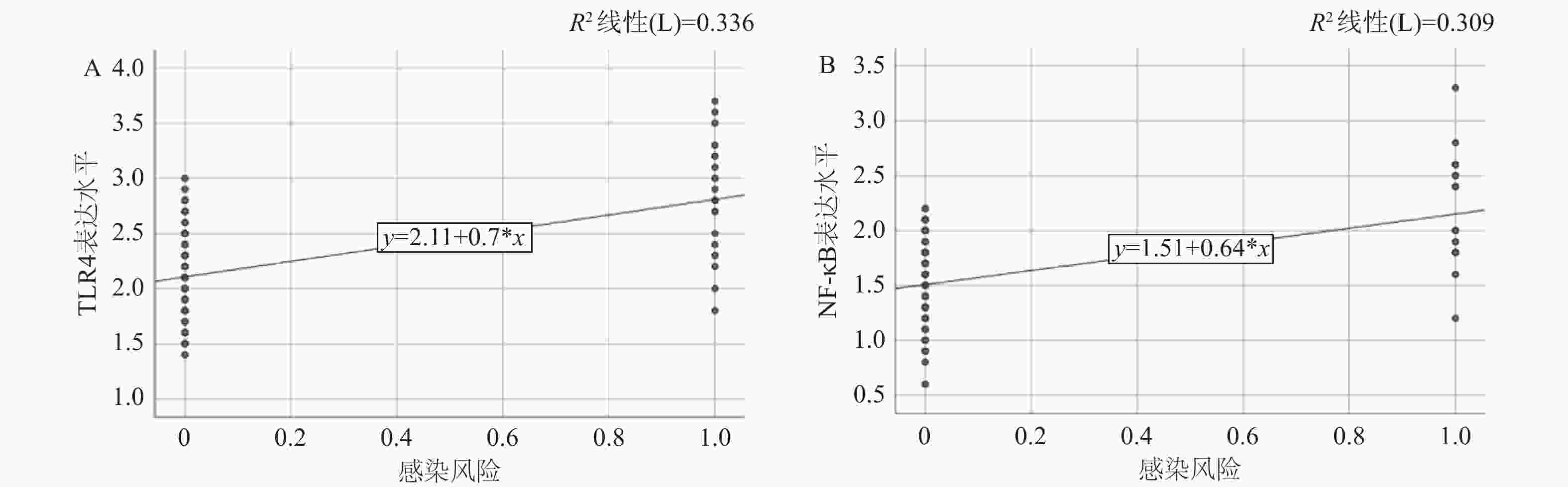
图 3 TLR4、NF-κB与烧伤患者导管相关性真菌感染的相关性
A:TLR4表达水平与感染相关性;B:NF-κB表达水平与感染相关性。
Figure 3. Correlation between TLR4,NF-κB and catheter-related fungal infection in burn patients
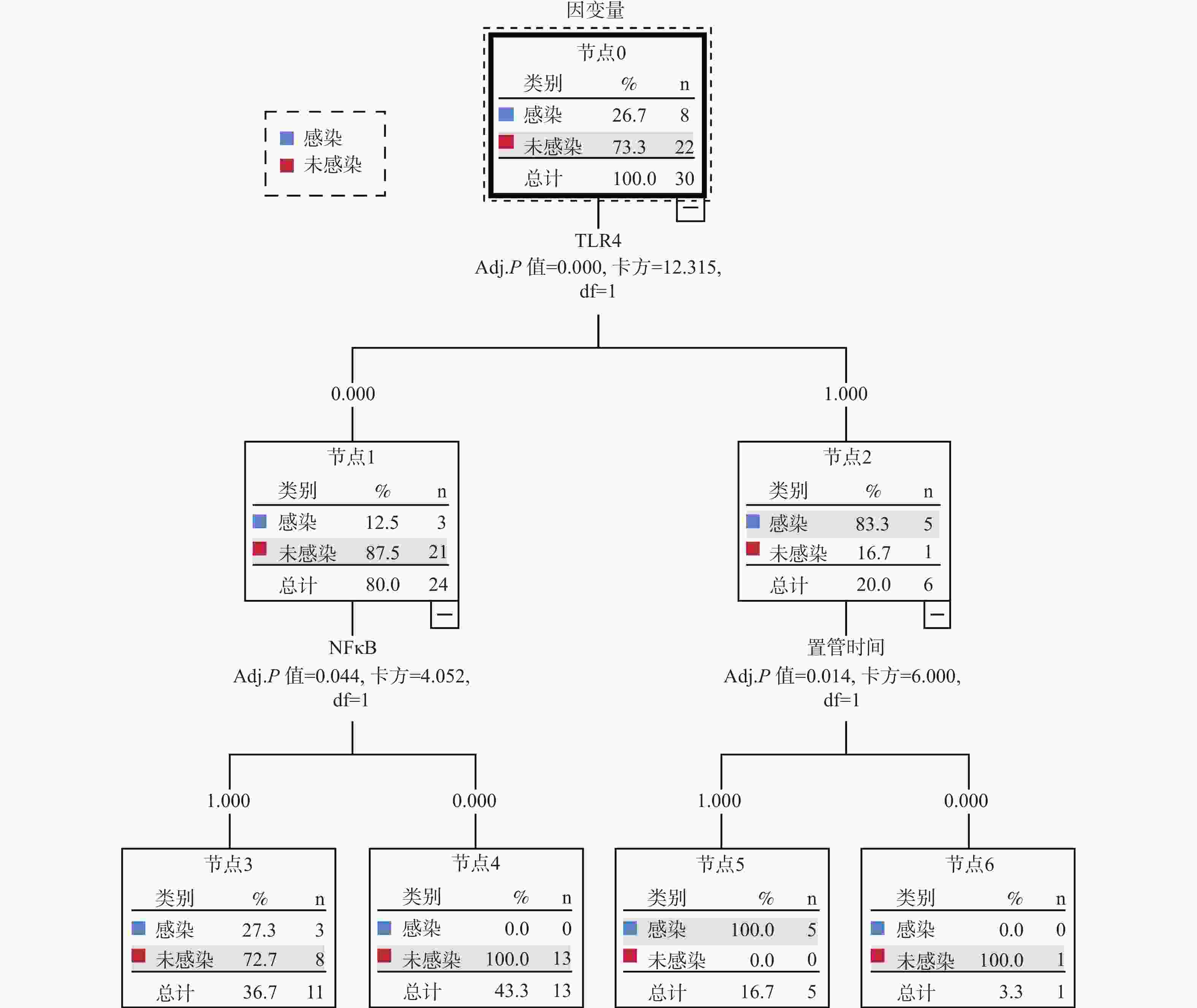
图 5 烧伤患者导管相关性真菌感染的决策树模型
Figure 5. Decision tree model of catheter-related fungal infection in burn patients
表 1 TLR4、NF-κB预测烧伤患者导管相关性真菌感染效能
Table 1. Efficacy of TLR4 and NF-κB in predicting catheter-related fungal infection in burn patients
因素 AUC P 95%CI 最佳截断值 灵敏度 特异度 TLR4 0.862 0.048* 0.768~0.956 2.650 0.682 0.909 NF-κB 0.851 0.046* 0.760~0.941 1.750 0.864 0.739 *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 烧伤患者导管相关性真菌感染的单因素分析[n(%)]
Table 2. Univariate factor analysis of catheter-related fungal infection in burn patients [n(%)]
项目 感染组(n = 22) 未感染组(n = 88) χ2 P 性别 0.156 0.693 男 13(59.09) 56(63.64) 女 9(40.91) 32(36.36) 年龄(岁) 3.128 0.077 ≥60 10(45.45) 23(26.14) <60 12(54.55) 65(73.86) 高血压 2.724 0.099 是 10(45.45) 24(27.27) 否 12(54.55) 64(72.73) 糖尿病 9.429 0.002* 是 13(59.09) 22(25.00) 否 9(40.91) 66(75.00) 贫血 1.069 0.301 是 4(18.18) 9(10.23) 否 18(81.82) 79(89.77) 烧伤面积(%) 6.950 0.008* ≥30 14(63.64) 29(32.95) <30 8(36.36) 59(67.05) 住院时间(d) 0.293 0.589 ≥14 4(18.18) 12(13.64) <14 18(81.82) 76(86.36) 置管时间(d) 12.650 <0.001* ≥7 17(77.27) 31(35.23) <14 5(22.73) 57(64.77) 置管静脉 0.948 0.814 股静脉 3(13.64) 15(17.05) 锁骨下静脉 12(54.55) 39(44.32) 贵要静脉 2(9.09) 13(14.77) 颈内静脉 5(22.73) 21(23.86) TLR4表达水平 37.161 <0.001* ≥2.65 15(68.18) 8(9.09) <2.65 7(31.82) 80(90.91) NF-κB表达水平 27.047 <0.001* ≥1.75 19(86.36) 23(26.14) <1.75 3(13.64) 65(73.86) *P < 0.05。
下载: 导出CSV
表 3 自变量赋值说明
Table 3. Assignment of independent variables
自变量 变量说明 赋值 糖尿病 分类变量 否=0,是=1 烧伤面积 分类变量 <30%=0,≥30%=1 置管时间 分类变量 <14 d=0,≥14 d=1 TLR4 分类变量 <2.65=0,≥2.65=1 NF-κB 分类变量 <1.75=0,≥1.75=1
下载: 导出CSV
表 4 烧伤患者导管相关性真菌感染因素共线性检验
Table 4. Colinearity test of catheter-related fungal infection factors in burn patients
变量 标注化系数Beta t P 容差 VIF 常量 / −2.827 0.006* / / 糖尿病 0.170 2.451 0.016* 0.908 1.102 烧伤面积 0.112 1.643 0.103 0.948 1.054 置管时间 0.175 2.522 0.013* 0.908 1.102 TLR4 0.446 6.359 <0.001* 0.887 1.127 NF-κB 0.289 4.032 <0.001* 0.849 1.178 *P < 0.05。
下载: 导出CSV
表 5 烧伤患者导管相关性真菌感染的多因素分析
Table 5. Multivariate analysis of catheter-related fungal infection in burn patients
自变量 B SE Wald P OR 95%CI 糖尿病 2.332 0.990 5.549 0.018* 10.298 1.479~71.679 烧伤面积 1.907 0.949 4.034 0.045* 6.730 1.047~43.258 置管时间 2.207 0.922 5.725 0.017* 9.090 1.491~55.433 TLR4 4.541 1.253 13.126 <0.001* 93.771 8.039~ 1093.718 NF-κB 3.920 1.295 9.159 0.002* 50.409 3.981~ 638.3797 常量 −8.783 2.138 16.870 <0.001* 0.000 / *P < 0.05。
下载: 导出CSV
-
[1] Kovács R, Majoros L. Antifungal lock therapy: An eternal promise or an effective alternative therapeutic approach?[J]. Lett Appl Microbiol, 2022, 74(6): 851-862. doi: 10.1111/lam.13653 [2] Wang Y, Li Q, Shu Q, et al. Clinical epidemiology and a novel predicting nomogram of central line associated bloodstream infection in burn patients[J]. Epidemiol Infect, 2023, 151: e90. doi: 10.1017/S0950268823000766 [3] Pongrácz J, Szabó T, Juhász E, et al. Epidemiology, risk factors and mortality of fungal bloodstream infection: 14Years of experience at a teaching hospital[J]. Mycopathologia, 2025, 190(4): 55. doi: 10.1007/s11046-025-00965-3 [4] Spera A M, Folliero V, D’Amore C, et al. Nine-year surveillance of Candida bloodstream infections in a southern Italian tertiary hospital: Species distribution, antifungal resistance, and stewardship implications[J]. J Pers Med, 2026, 16(1): 17. doi: 10.3390/jpm16010017 [5] Afanou A K, Mundra S, Fjeld Estensmo E L, et al. Divergent TLR2 and TLR4 activation by fungal spores and species diversity in dust from waste sorting plants[J]. Appl Environ Microbiol, 2023, 89(3): e01734-e01722. [6] Guldenpfennig C, Teixeiro E, Daniels M. NF-kB’s contribution to B cell fate decisions[J]. Front Immunol, 2023, 14: 1214095. doi: 10.3389/fimmu.2023.1214095 [7] 李琰光, 昌帅磊, 谢江帆, 等. 危重烧伤并发侵袭性真菌感染患者的临床特征及死亡危险因素分析[J]. 中华烧伤与创面修复杂志, 2023(7): 618-624. [8] 梁显南, 颜帅, 吉家聪, 等. 四肢深度烧伤患者创面感染的病原菌分布、危险因素分析及血清促炎因子水平变化的临床意义[J]. 现代生物医学进展, 2022, 22(16): 3143-3147. [9] 中国医疗保健国际交流促进会烧伤医学分会, 《中华烧伤与创面修复杂志》编辑委员会. 烧伤侵袭性真菌感染诊断与防治实践指南(2024版)[J]. 中华烧伤与创面修复杂志, 2024, 40(7): 604-617. [10] 中华医学会重症医学分会. 血管内导管相关性血流感染预防与诊治指南(2025)[J]. 中华危重病急救医学, 2025, 37(3): 193-220. doi: 10.3760/cma.j.cn121430-20250301-00199 [11] Miller A, Vujcich E, Brown J. Effect of central line duration and other risk factors on central line-associated bloodstream infection in severe adult burns patients at a large tertiary referral burns centre: A 5-year retrospective study[J]. Eur Burn J, 2022, 3(1): 18-26. doi: 10.3390/ebj3010003 [12] Hou T, Bell W R, Mesa H. Invasive fungal infections of the head and neck: A tertiary hospital experience[J]. Pathogens, 2024, 13(7): 530. doi: 10.3390/pathogens13070530 [13] Dudoignon E, Chevret S, Tsague S, et al. Risk factors and outcome associated with fungal infections in patients with severe burn injury: 10-year retrospective IFI-BURN study[J]. Clin Infect Dis, 2024, 79(3): 682-689. doi: 10.1093/cid/ciae337 [14] 刘薇, 程翔, 梁玉龙, 等. 不同烧伤面积患者创面感染病原菌分布及其耐药性[J]. 中国感染控制杂志, 2022, 21(1): 30-36. [15] 俞国军, 王莽元, 张为民, 等. Stanford A型主动脉夹层患者术后血流感染病原菌分布及其影响因素的Logistic回归分析[J]. 现代生物医学进展, 2024, 24(9): 1668-1671+1667. doi: 10.13241/j.cnki.pmb.2024.09.013 [16] Wu H, Li C, Wang Y, et al. Transcriptomics reveals effect of Pulsatilla decoction butanol extract in alleviating vulvovaginal candidiasis by inhibiting neutrophil chemotaxis and activation via TLR4 signaling[J]. Pharmaceuticals, 2024, 17(5): 594. doi: 10.3390/ph17050594 [17] Tang D, Cao X, Yuan B, et al. Correlation analysis between IL-1R/TLRs pathway and superficial dermatomycosis[J]. Eur J Med Res, 2025, 30(1): 191. doi: 10.1186/s40001-025-02434-5 [18] 刘燕, 马清昌, 徐伟, 等. TLR4、TREM1在烧伤感染患者血清中的表达水平及其诊断价值[J]. 广东医学, 2022, 43(2): 208-212. doi: 10.13820/j.cnki.gdyx.20212276 [19] 韩燕梅, 崔萍, 柏慧. 老年急性脑梗死患者肺部感染的病原学特征及与TLR4/NF-κB信号通路的相关性[J]. 中国实用医刊, 2023, 50(20): 43-46. doi: 10.3760/cma.j.cn115689-20230614-02385 [20] 高峰, 王兵, 赵瑞苓, 等. TLR4/MyD88/NF-κB通路在真菌性角膜炎中的表达和作用[J]. 中华医院感染学杂志, 2022, 32(2): 237-241. doi: 10.11816/cn.ni.2022-210464 [21] 王芳, 余锋, 姚豪杰, 等. 导管相关性真菌血流感染病原菌生物膜形成及预后影响因素[J]. 中华医院感染学杂志, 2022, 32(3): 408-411. doi: 10.11816/cn.ni.2022-210582 [22] 张成, 龚雅利, 罗小强, 等. 重度烧伤患者真菌血流感染的病原学特征分析[J]. 中华烧伤杂志, 2020(1): 37-41. [23] Li X, Yu B, Li H, et al. Drug clues for the treatment of fungal catheter-related bloodstream infection with antifungal lock therapy[J]. Drug Des Dev Ther, 2025, 19: 683-701. doi: 10.2147/DDDT.S501664 [24] Cornely O A, Sprute R, Bassetti M, et al. Global guideline for the diagnosis and management of candidiasis: An initiative of the ECMM in cooperation with ISHAM and ASM[J]. Lancet Infect Dis, 2025, 25(5): e280-e293. doi: 10.1016/S1473-3099(24)00749-7 [25] Bing J, Du H, Guo P, et al. Candida auris-associated hospitalizations and outbreaks, China, 2018–2023[J]. Emerg Microbes Infect, 2024, 13(1): 2302843. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 210
- HTML全文浏览量: 135
- PDF下载量: 98
- 被引次数: 0
