

Construction and Validation of Nomogram Based on Contrast-enhanced Ultrasound for Predicting Platinum Chemotherapy Sensitivity in Breast Cancer Patients
-
摘要:
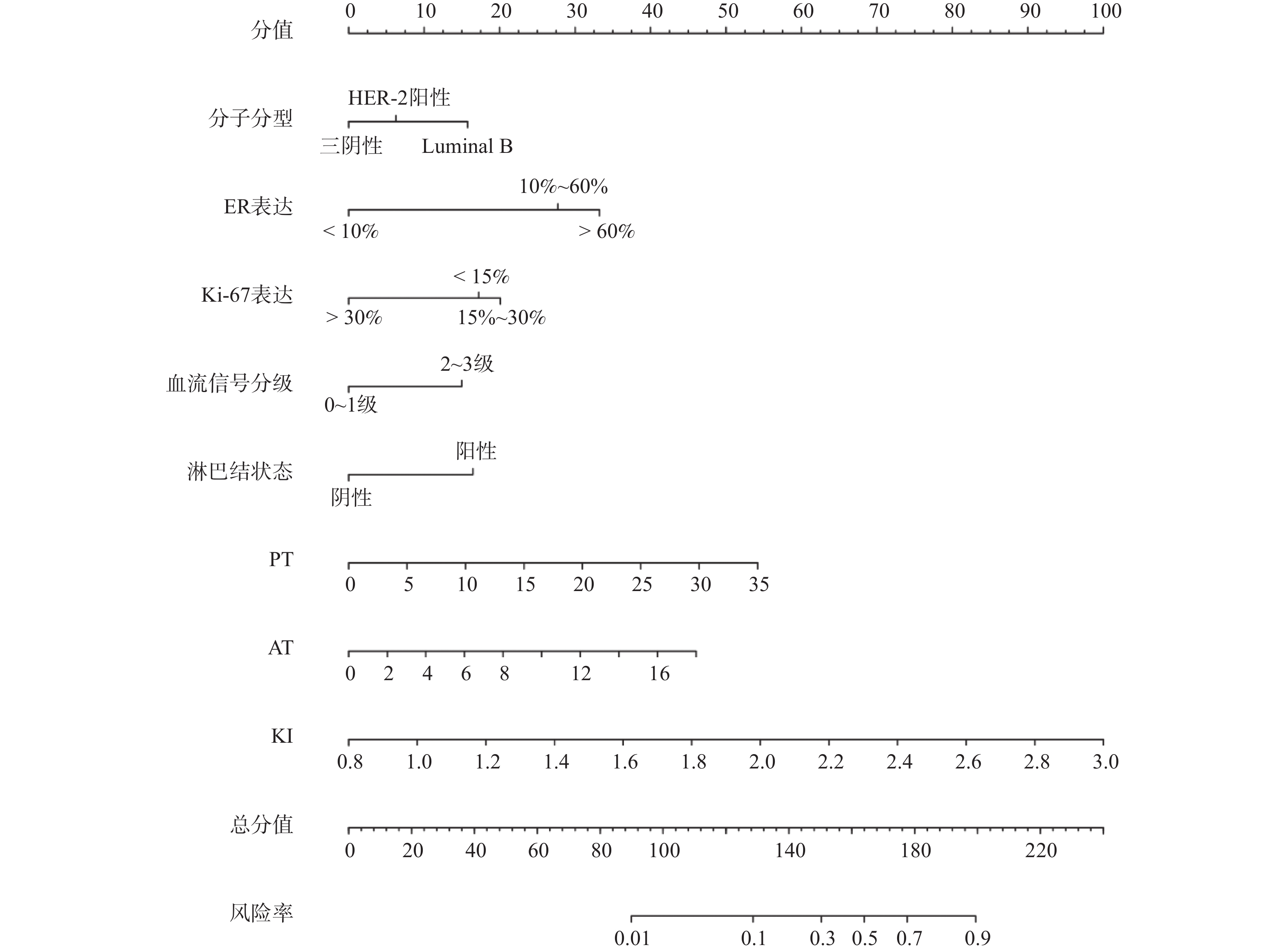
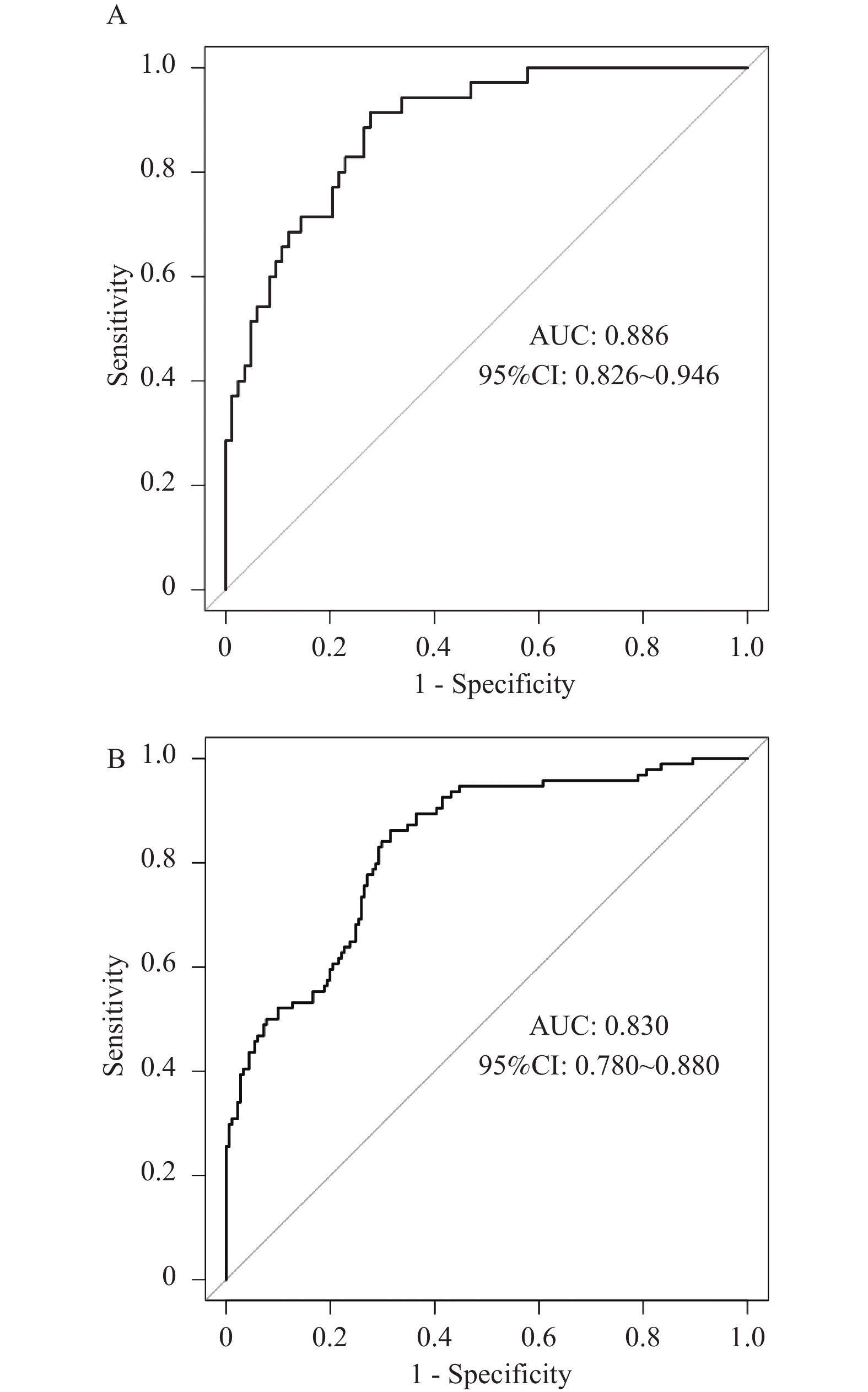
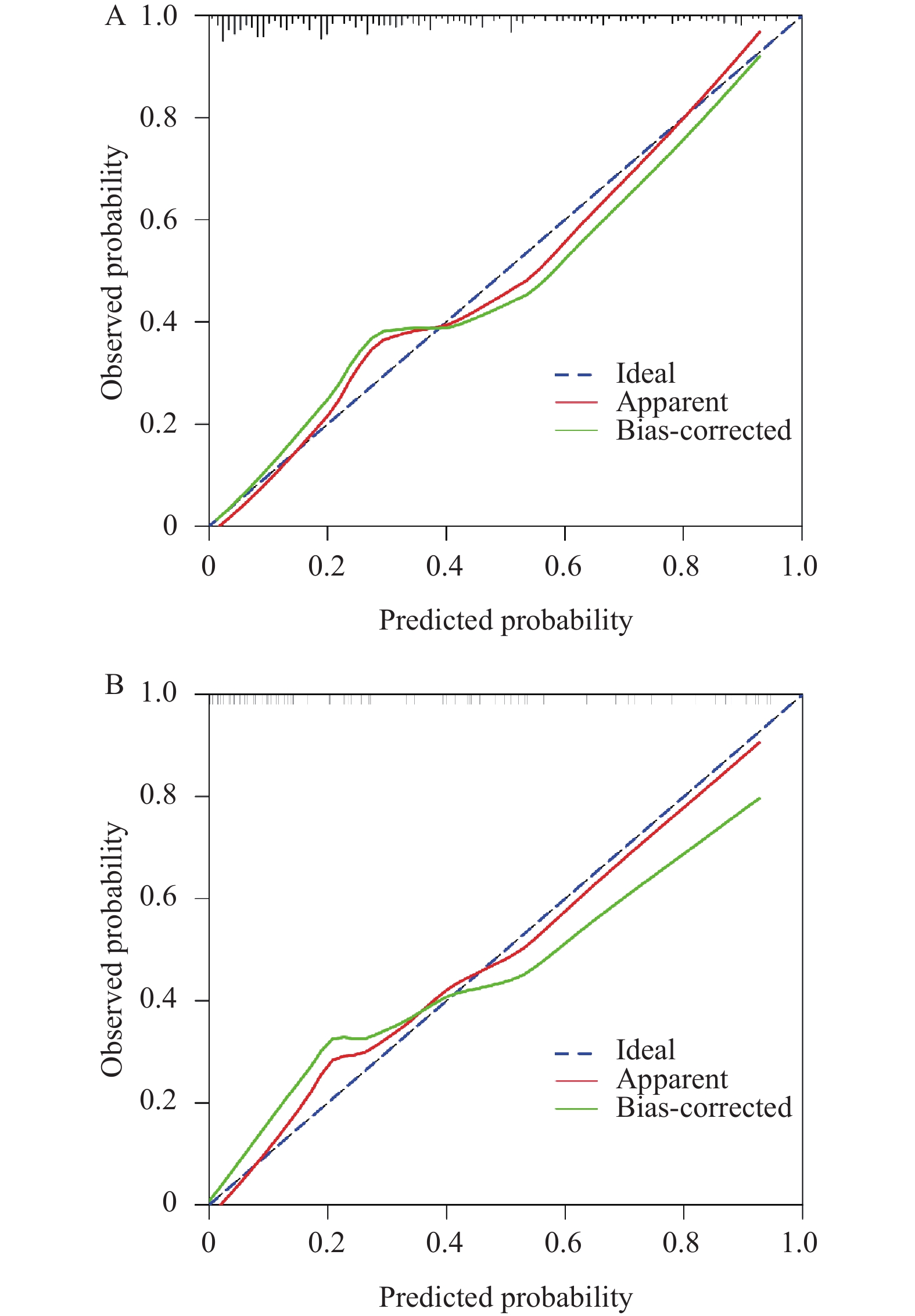
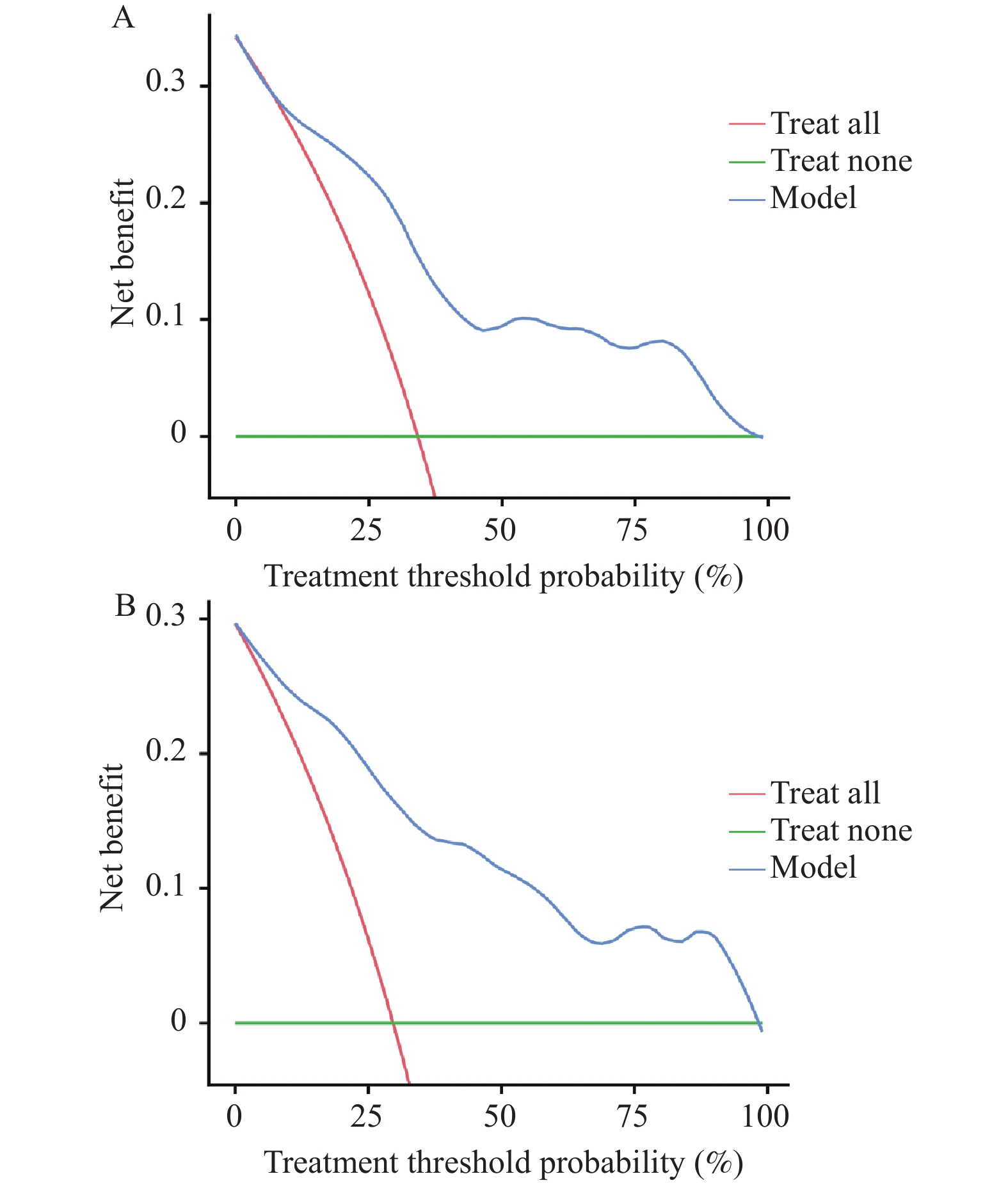
目的 探讨基于超声造影(contrast-enhanced ultrasound,CEUS)定量参数构建的列线图模型对乳腺癌患者铂类药物化疗敏感性的预测价值,为临床治疗提供参考。 方法 前瞻性选取广元市中心医院2021年1月至2024年12月收治的275例乳腺癌患者为建模队列,按7:3比例选取2025年1月至2025年7月118例乳腺癌患者为时间验证队列,均行铂类药物化疗,根据化疗后是否达到病理学完全缓解(pathologic complete response,pCR)分为铂类耐药组(未达到pCR,n = 94)、铂类敏感组(达到pCR,n = 181)。多因素Logistic回归分析乳腺癌患者铂类药物化疗敏感的影响因素,构建列线图预测模型;进行模型验证,以受试者工作特征(receiver operating characteristic,ROC)曲线、校准曲线、决策曲线(decision curve analysis,DCA)评估列线图模型的区分度、一致性及临床实用性。 结果 建模队列、时间验证队列临床资料比较均无明显差异(P > 0.05);建模队列中两组分子分型、ER表达、Ki-67表达、血流信号分级、淋巴结状态、峰值时间(peak time,TTP)、始增时间(arrival time,AT)、上升支斜率(wash-in rate,WiR)比较差异明显(P < 0.05);多因素Logistic回归分析结果显示,分子分型、ER表达、Ki-67表达、淋巴结状态、TTP、AT、WiR均是乳腺癌患者铂类药物化疗耐药的独立影响因素(P < 0.05);基于Logistic回归分析结果构建列线图预测模型。ROC曲线显示,预测乳腺癌患者铂类药物化疗耐药的列线图模型在建模队列中预测的曲线下面积(area under the curve,AUC)为0.886(95%CI:0.826~0.946),敏感度为92.55%、特异度为88.95%,在时间验证队列中预测的AUC为0.830(95%CI:0.780~0.880),敏感度为91.43%、特异度为86.75%,模型区分度良好;采用Hosmer-Lemeshow拟合优度检验显示P > 0.05,在建模队列、时间验证队列中校准曲线的Brier分数分别为0.122、0.141;DCA曲线提示,当阈概率在40%至80%范围内时,使用该列线图模型指导临床决策能提供比“全治”或“全不治”策略更高的净获益,临床实用性较高。 结论 整合了分子分型、ER、Ki-67、淋巴结状态及CEUS定量参数(TTP、AT、WiR)的列线图模型,对乳腺癌患者铂类药物化疗耐药风险具有良好的预测效能。 Abstract:Objective To explore the predictive value of a nomogram model based on quantitative parameters from contrast-enhanced ultrasound (CEUS) for platinum-based chemotherapy sensitivity in breast cancer patients, providing clinical reference for treatment decisions. Methods A prospective study enrolled 275 breast cancer patients treated at Guangyuan Central Hospital from January 2021 to December 2024 as the modeling cohort, with 118 breast cancer patients from January to July 2025 selected at a 7:3 ratio as the temporal validation cohort. All patients received platinum-based chemotherapy and were stratified based on achievement of pathologic complete response (pCR) following chemotherapy into platinum-resistant group (without pCR, n = 94) and platinum-sensitive group (with pCR, n = 181). Multivariate logistic regression was used to analyze the influencing factors of platinum-based chemotherapy sensitivity in breast cancer patients, and a nomogram prediction model was constructed. The discrimination, consistency and clinical practicability of the nomogram model were evaluated by receiver operating characteristic (ROC) curve, calibration curve and decision curve (DCA). Results Clinical characteristics showed no significant differences between the modeling and temporal validation cohorts(P > 0.05). In the modeling cohort, significant differences were observed between the two groups in molecular subtype, ER expression, Ki-67 expression, blood flow signal grade, lymph node status, peak time (TTP), arrival time (AT), and wash-in rate (WiR)(P < 0.05). Multivariate Logistic regression analysis showed that molecular subtype, ER expression, Ki-67 expression, lymph node status, TTP, AT and WiR were all independent influencing factors for platinum chemotherapy resistance in breast cancer patients (P < 0.05). Based on the results of Logistic regression analysis, a nomogram prediction model was constructed. ROC curve showed that the nomogram model for predicting platinum-based chemotherapy resistance had an area under the curve (AUC) of 0.886 (95%CI: 0.826~0.946)in the modeling cohort with sensitivity of 92.55% and specificity of 88.95%, and an AUC of 0.830 (95%CI: 0.780~0.880) in the temporal validation cohort with sensitivity of 91.43% and specificity of 86.75%, demonstrating good discrimination. The Hosmer-Lemeshow goodness-of-fit test showed P > 0.05, with Brier scores of 0.122 and 0.141 for calibration curves in the modeling and temporal validation cohorts, respectively. The DCA curve suggests that when the threshold probability ranges from 40% to 80%, using this nomogram model for clinical decision-making provides higher net benefit compared to "treat all" or "treat none" strategies, demonstrating good clinical utility. Conclusion A nomogram model integrating molecular subtype, ER, Ki-67, lymph node status, and CEUS quantitative parameters (TTP, AT, WiR) demonstrates good predictive efficacy for platinum-based chemotherapy resistance risk in breast cancer patients. -
Key words:
- Breast cancer /
- Contrast-enhanced ultrasound /
- Nomogram model /
- Chemotherapy /
- Platinum sensitive /
- Platinum resistance
-
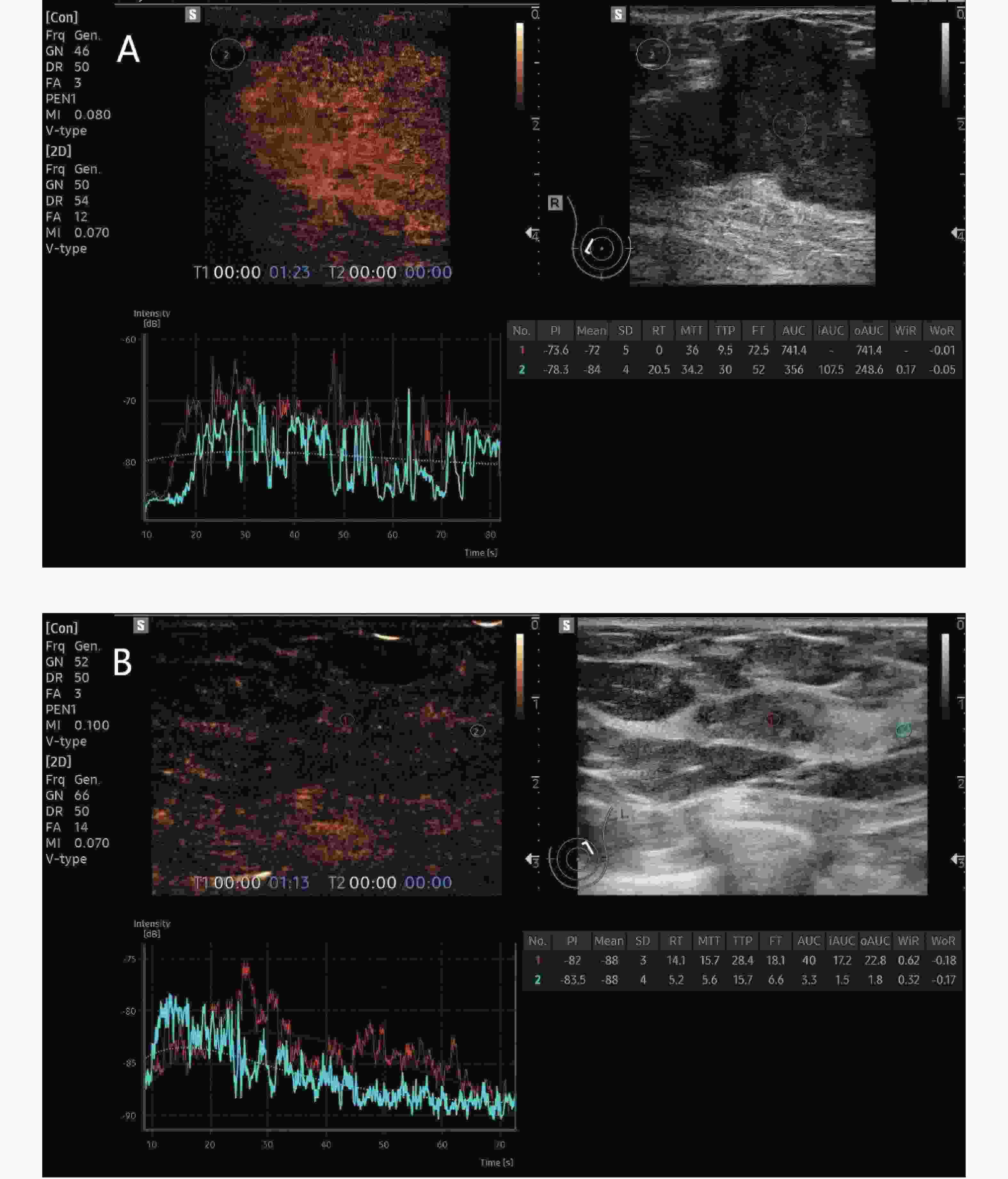
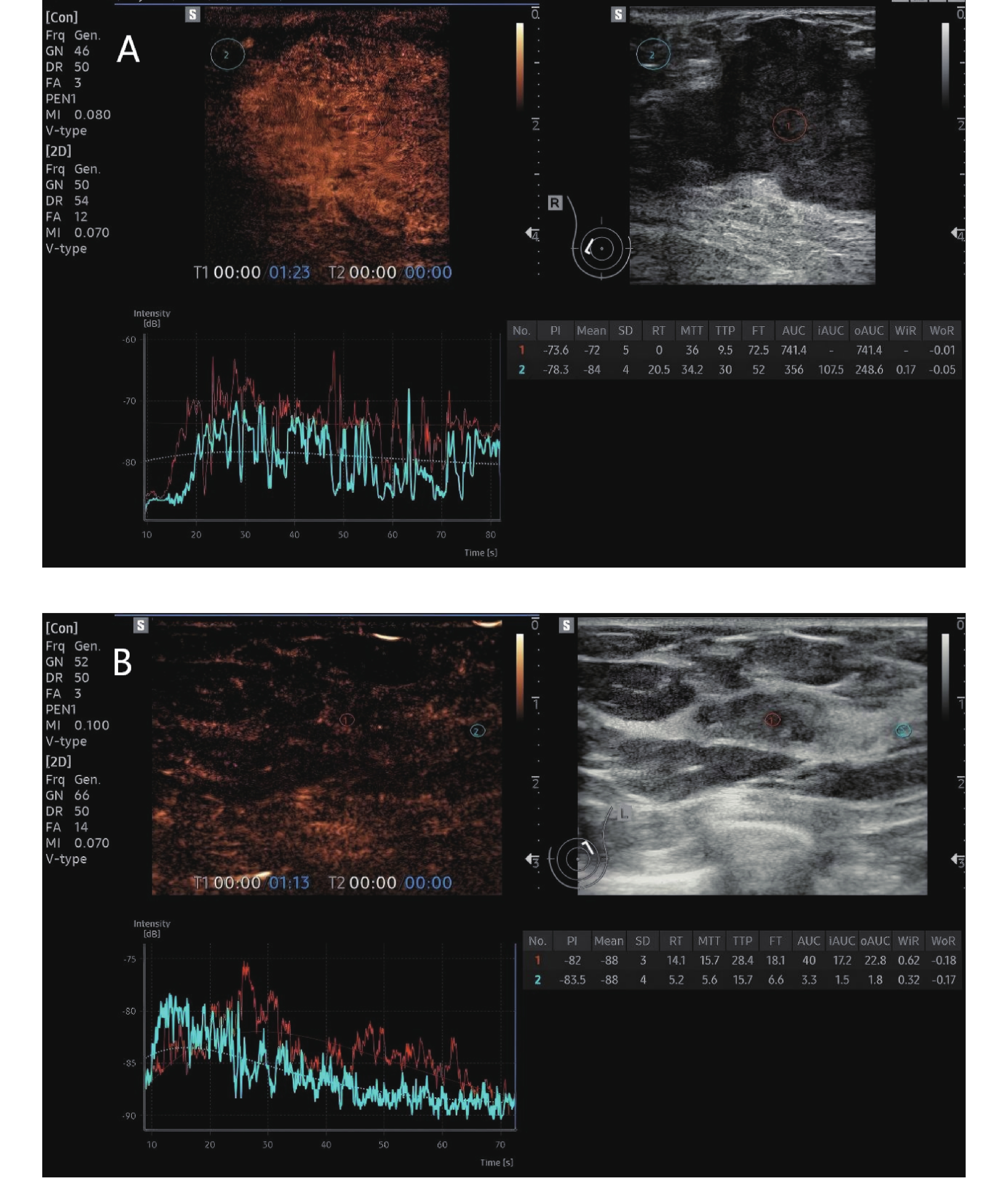
图 1 铂类耐药、铂类敏感乳腺癌患者典型CEUS图像
A:铂类耐药,女性,60岁,确诊右侧乳腺癌,行新辅助化疗6周期后超声造影图像;B:铂类敏感,女性,55岁,确诊左侧乳腺癌,行新辅助化疗6周期后超声造影图像。
Figure 1. Typical CEUS images of patients with platinum-resistant and platinum-sensitive breast cancer
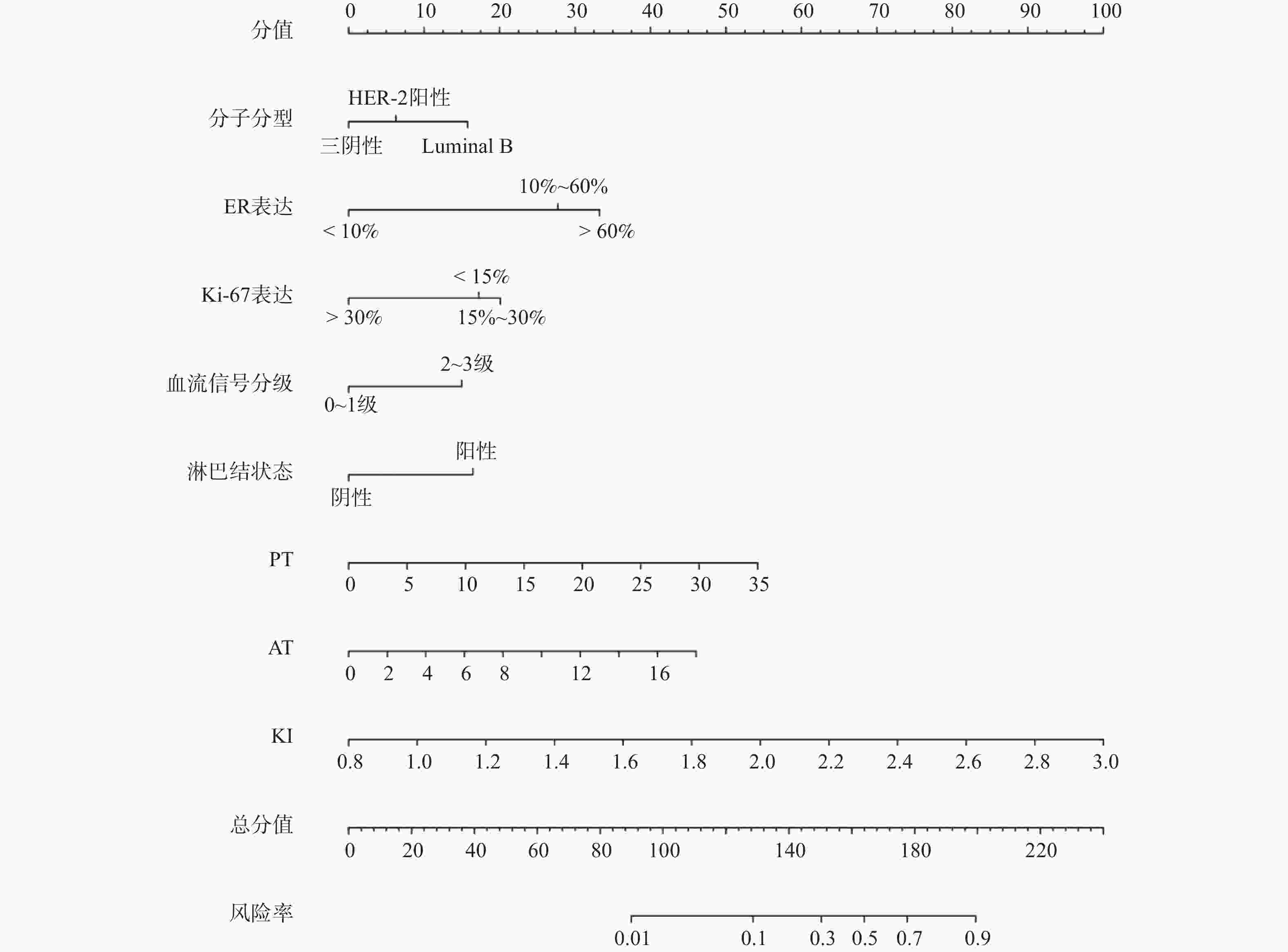
图 2 乳腺癌患者铂类药物化疗耐药的列线图预测模型
Figure 2. Nomogram prediction model of platinum-based chemotherapy resistance in breast cancer patients
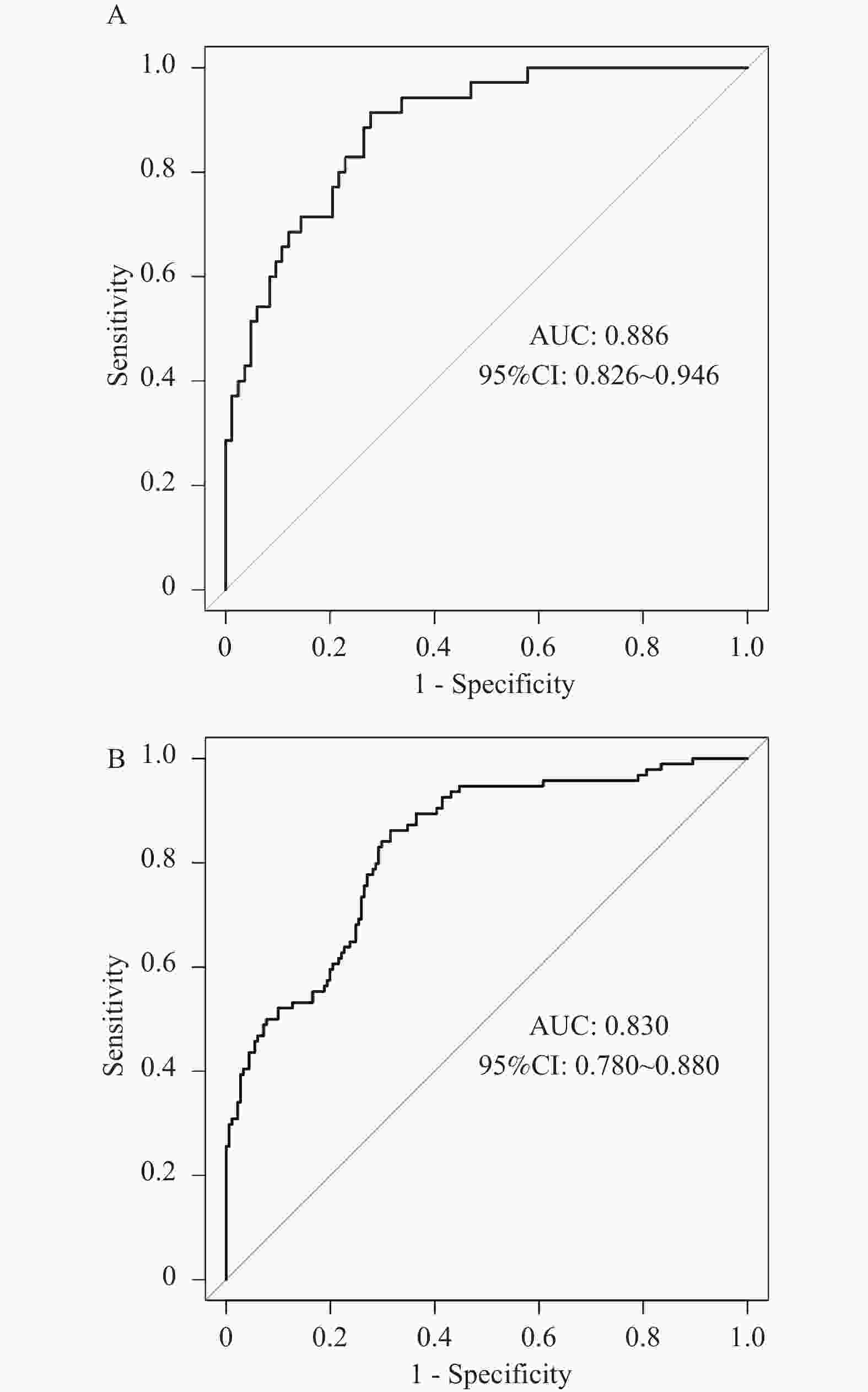
图 3 列线图模型预测乳腺癌患者铂类药物化疗耐药的ROC曲线
A:建模队列;B:时间验证队列。
Figure 3. ROC curve of the nomogram model for predicting platinum-based chemotherapy resistance in breast cancer patients
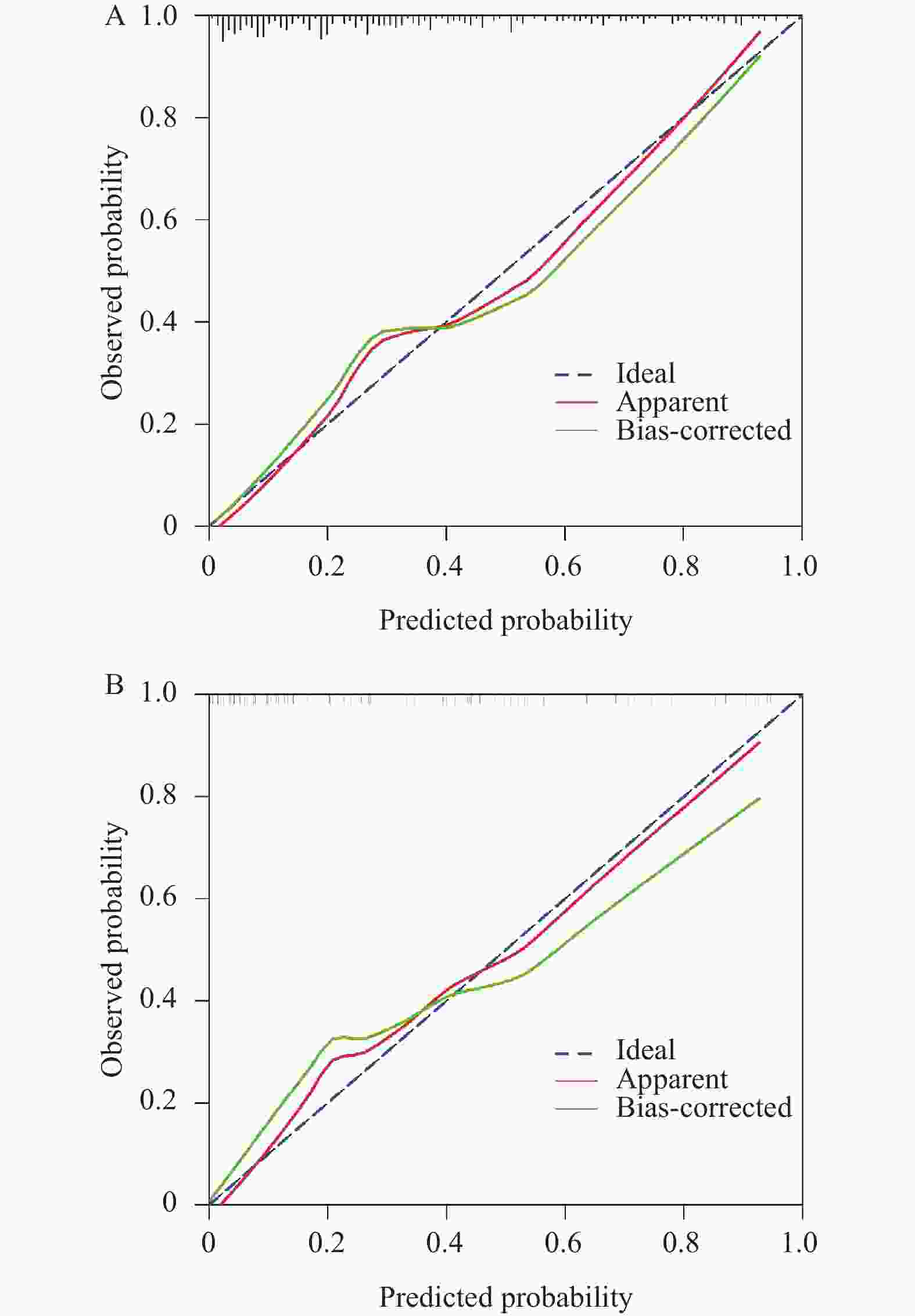
图 4 列线图模型预测乳腺癌患者铂类药物化疗耐药的校准曲线
A:建模队列;B:时间验证队列。
Figure 4. Calibration curve of nomogram model for predicting platinum-based chemotherapy resistance in breast cancer patients
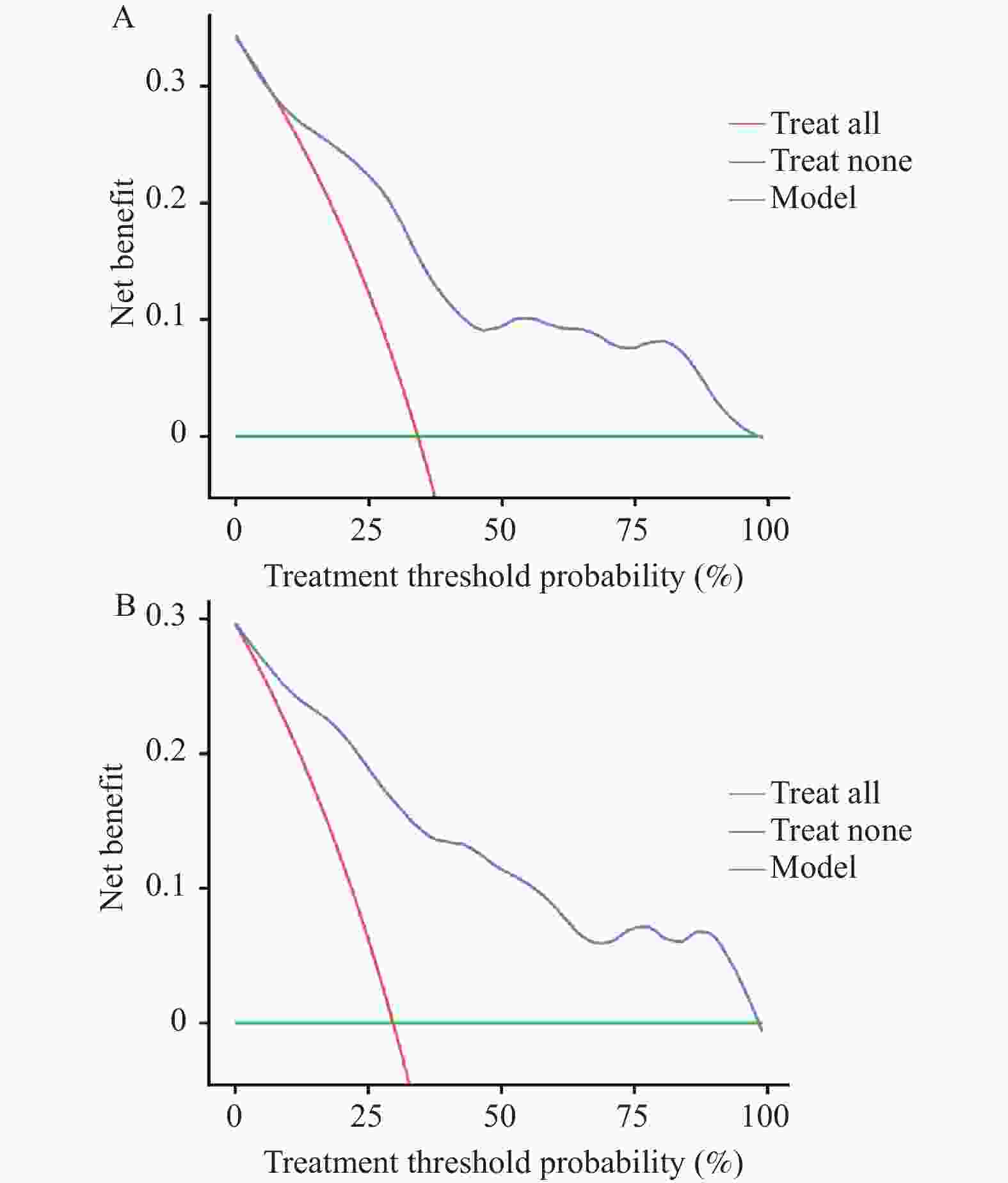
图 5 列线图模型预测乳腺癌患者铂类药物化疗耐药的DCA曲线
A:建模队列;B:时间验证队列。
Figure 5. DCA curve of line graph model predicting platinum-based chemotherapy in breast cancer patients
表 1 建模队列、时间验证队列临床资料比较[($ \bar x \pm s $)/n(%)]
Table 1. Comparison of clinical data between modeling cohort and validation cohort [($ \bar x \pm s $)/n(%)]
临床资料 建模队列(n=275) 时间验证队列(n=118) t/χ2 P 年龄(岁) 49.32 ± 5.87 50.36 ± 6.25 1.579 0.115 体重指数(kg/m2) 22.36 ± 1.74 22.51 ± 1.69 0.790 0.430 月经状态 1.610 0.204 绝经 123(44.73) 61(51.69) 未绝经 152(55.27) 57(48.31) 家族史 25(9.09) 8(6.78) 0.573 0.449 基础疾病 高血压 29(10.55) 17(14.41) 1.191 0.275 糖尿病 23(8.36) 15(12.71) 1.787 0.181 瘤体直径(cm) 3.48 ± 0.92 3.53 ± 1.01 0.479 0.632 瘤体位置 0.077 0.782 左侧 151(54.91) 63(53.39) 右侧 124(45.09) 55(46.61) 临床分期 0.208 0.649 Ⅱ期 156(56.73) 64(54.24) Ⅲ期 119(43.27) 54(45.76) 病理分型 1.883 0.170 非浸润性癌 61(22.18) 19(16.10) 浸润性癌 214(77.82) 99(83.90) 分子分型 4.559 0.102 HER-2阴性 163(59.27) 59(50.00) 三阴性 45(16.36) 18(15.25) HER-2阳性 67(24.36) 41(34.75) BRCA突变状态 0.036 0.850 突变型 24(8.73) 11(9.32) 野生型 251(91.27) 107(90.68) 铂类药物耐药率 94(34.18) 35(29.66) 0.765 0.382  下载: 导出CSV
下载: 导出CSV
表 2 建模队列乳腺癌患者铂类药物化疗敏感性的单因素分析[($ \bar x \pm s $)/n(%)]
Table 2. Univariate analysis of platinum-based chemotherapy sensitivity of breast cancer patients in a modeled cohort [($ \bar x \pm s $)/n(%)]
临床资料 铂类耐药组(n=94) 铂类敏感组(n=181) t/χ2 P 年龄(岁) 50.13 ± 5.61 48.90 ± 5.78 1.691 0.092 体重指数(kg/m2) 22.14 ± 1.56 22.47 ± 1.69 1.576 0.116 月经状态 3.164 0.075 绝经 49(52.13) 74(40.88) 未绝经 45(47.87) 107(59.12) 家族史 8(8.51) 17(9.39) 0.058 0.809 基础疾病 高血压 9(9.57) 20(11.05) 0.143 0.706 糖尿病 10(10.64) 13(7.18) 0.964 0.326 瘤体直径(cm) 3.56 ± 0.84 3.44 ± 0.85 1.115 0.266 瘤体位置 0.125 0.723 左侧 53(56.38) 98(54.14) 右侧 41(43.62) 83(45.86) 临床分期 3.532 0.060 Ⅱ期 46(48.94) 110(60.77) Ⅲ期 48(51.06) 71(39.23) 病理分型 0.761 0.383 非浸润性癌 18(19.15) 43(23.76) 浸润性癌 76(80.85) 138(76.24) 分子分型 7.091 0.029* HER-2阴性 66(70.21) 97(53.59) HER-2阳性 17(18.09) 50(27.62) 三阴性 11(11.70) 34(18.78) PR表达(阳性染色细胞所占百分比,%) 0.019 0.890 <10 34(36.17) 67(37.02) ≥10 60(63.83) 114(62.98) ER表达(阳性染色细胞所占百分比,%) 10.739 0.005* <10 2(2.13) 22(12.15) 10~60 30(31.91) 69(38.12) >60 62(65.96) 90(49.72) Ki-67表达(阳性染色细胞所占百分比,%) 14.066 0.001* <15 20(21.28) 36(19.89) 15~30 59(62.77) 78(43.09) >30 15(15.96) 67(37.02) BRCA突变状态 0.129 0.720 突变型 9(9.57) 15(8.29) 野生型 85(90.43) 166(91.71) 血流信号分级 8.568 0.003* 0~1级 62(65.96) 148(81.77) 2~3级 32(34.04) 33(18.23) 淋巴结状态 8.624 0.003* 阴性 68(72.34) 157(86.74) 阳性 26(27.66) 24(13.26) CEUS定量参数 TTP(s) 20.36 ± 4.91 17.47 ± 4.63 4.809 <0.001* AT(s) 9.62 ± 2.62 8.57 ± 2.19 3.521 0.001* PI(dB) 24.17 ± 3.72 23.84 ± 3.90 0.676 0.500 WiR 1.78 ± 0.31 1.54 ± 0.27 6.641 <0.001* *P < 0.05。
下载: 导出CSV
表 3 赋值表
Table 3. Assignment table
因素 赋值 分子分型 HER-2阴性=1,三阴性=2,HER-2阳性=3 ER表达(%) <10=1,10~60=2,>60=3 Ki-67表达(%) <15=1,15~30=2,>30=3 淋巴结状态 阴性=0,阳性=1 TTP 实际值带入 AT 实际值带入 WiR 实际值带入
下载: 导出CSV
表 4 建模队列中乳腺癌患者铂类药物化疗耐药的多因素Logistic回归分析
Table 4. Multivariate Logistic regression analysis of platinum chemotherapy resistance in breast cancer patients in the modeling cohort
因素 β S.E. Waldχ2 OR 95%CI P 下限 上限 分子分型(参考:HER-2阴性) 三阴性 −1.124 0.397 8.016 0.325 0.149 0.708 0.005* HER-2阳性 −0.785 0.317 6.132 0.456 0.245 0.849 0.013* ER表达(%) 10~60 0.745 0.328 5.159 2.106 1.108 4.006 0.023* >60 1.534 0.385 15.876 4.637 2.180 9.861 <0.001* Ki-67表达(参考:<15%) 15~30 1.057 0.391 7.308 2.878 1.337 6.193 0.007* >30 1.605 0.457 12.333 4.978 2.033 12.191 <0.001* 淋巴结状态(阳性) 1.914 0.439 19.009 6.780 2.868 16.030 <0.001* TTP 0.121 0.039 9.626 1.129 1.046 1.218 0.002* AT 0.300 0.116 6.708 1.350 1.016 1.795 0.010* WiR 0.341 0.138 6.106 1.406 1.073 1.843 0.014* *P < 0.05。
下载: 导出CSV
-
[1] Katsura C, Ogunmwonyi I, Kankam H K, et al. Breast cancer: Presentation, investigation and management[J]. Br J Hosp Med, 2022, 83(2): 1-7. [2] Wilkinson L, Gathani T. Understanding breast cancer as a global health concern[J]. Br J Radiol, 2022, 95(1130): 20211033. doi: 10.1259/bjr.20211033 [3] Britt K L, Cuzick J, Phillips K A. Key steps for effective breast cancer prevention[J]. Nat Rev Cancer, 2020, 20(8): 417-436. doi: 10.1038/s41568-020-0266-x [4] 王雪, 岳健, 康一坤, 等. DNA损伤修复变异指导铂类药物治疗三阴性乳腺癌的应用前景[J]. 中华肿瘤杂志, 2022, 44(1): 68-72. [5] 蔡凌翼, 陈涛, 张晓琳, 等. 基于基因组学视角的乳腺癌化疗耐药机制研究进展[J]. 中华全科医学, 2023, 21(12): 2005-2008+2073. [6] Mann R M, Kuhl C K, Moy L. Contrast-enhanced MRI for breast cancer screening[J]. J Magn Reson Imag, 2019, 50(2): 377-390. doi: 10.1002/jmri.26654 [7] 马维东, 张丹丹, 苏洁, 等. 乳腺癌超声造影参数与Ki-67、HER-2及雌孕激素水平的相关性[J]. 临床误诊误治, 2022, 35(3): 73-77. doi: 10.3969/j.issn.1002-3429.2022.03.017 [8] 杨亮, 张明帅. 环状RNA ADAM22 及其下游信号因子在顺铂耐药三阴性乳腺癌组织中的表达[J]. 中国医药, 2023, 18(2): 256-259. doi: 10.3760/j.issn.1673-4777.2023.02.022 [9] 中国抗癌协会乳腺癌专业委员会. 中国抗癌协会乳腺癌诊治指南与规范(2017年版)[J]. 中国癌症杂志, 2017, 27(9): 695-759. [10] 中华医学会妇科肿瘤学分会. 妇科肿瘤铂类药物临床应用指南[J]. 现代妇产科进展, 2021, 30(10): 721-736. doi: 10.12290/xhyxzz.2021-0690 [11] 李健斌, 江泽飞. 2021年中国临床肿瘤学会乳腺癌诊疗指南更新要点解读[J]. 中华医学杂志, 2021, 101(24): 1835-1838. [12] Ogston K N, Miller I D, Payne S, et al. A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival[J]. Breast, 2003, 12(5): 320-327. doi: 10.1016/S0960-9776(03)00106-1 [13] Kristiansen M U, Martiniussen M A, Larsen A S F. Contrast-enhanced ultrasound of breast tumors: An initial experience[J]. Acta Radiol Open, 2022, 11(4): 20584601221097458. [14] Leng X, Huang G, Li S, et al. Correlation of breast cancer microcirculation construction with tumor stem cells (CSCs) and epithelial-mesenchymal transition (EMT) based on contrast-enhanced ultrasound (CEUS)[J]. PLoS One, 2021, 16(12): e0261138. doi: 10.1371/journal.pone.0261138 [15] 马维东, 张丹丹, 苏洁, 等. 乳腺癌超声造影参数与Ki-67、HER-2及雌孕激素水平的相关性[J]. 临床误诊误治, 2022, 35(3): 73-77. [16] Rix A, Piepenbrock M, Flege B, et al. Effects of contrast-enhanced ultrasound treatment on neoadjuvant chemotherapy in breast cancer[J]. Theranostics, 2021, 11(19): 9557-9570. [17] 程春霞, 杨世艳, 赵寒箫, 等. 三阴性乳腺癌超声造影和声触诊组织成像特征及影响因素分析[J]. 临床超声医学杂志, 2023, 25(6): 483-487. doi: 10.3969/j.issn.1008-6978.2023.06.016 [18] 张刘璐, 陈媛琪, 邹佳晨, 等. 铂类在三阴性乳腺癌新辅助治疗中的应用进展及疗效预测作用[J]. 中华内分泌外科杂志, 2022, 16(5): 516-519. [19] Boca (Bene) I, Dudea S M, Ciurea A I. Contrast-enhanced ultrasonography in the diagnosis and treatment modulation of breast cancer[J]. J Pers Med, 2021, 11(2): 81. doi: 10.3390/jpm11020081 [20] Grewal D S, Bhanu K U, Sahni H, et al. Role of qualitative contrast-enhanced ultrasound in the diagnosis of malignant breast lesions[J]. Med J Armed Forces Ind, 2023, 79(4): 414-420. doi: 10.1016/j.mjafi.2022.01.015 [21] 宋晶晶, 熊伟, 姚淑辉, 等. AKR1C3通过PD1/PD-L1信号通路对乳腺癌细胞恶性生物学行为的干预作用[J]. 昆明医科大学学报, 2026, 47(1): 31-38. [22] Kondo S, Satoh M, Nishida M, et al. Ceusia-breast: Computer-aided diagnosis with contrast enhanced ultrasound image analysis for breast lesions[J]. BMC Med Imag, 2023, 23(1): 114. doi: 10.1186/s12880-023-01072-9 [23] 毛咪咪, 李海明, 石健, 等. 基于多序列MRI影像组学列线图预测上皮性卵巢癌患者对铂类药物化疗的敏感性[J]. 中华医学杂志, 2022, 102(3): 201-208. [24] Jia Y, Zhu Y, Li T, et al. Evaluating tumor-infiltrating lymphocytes in breast cancer: The role of conventional ultrasound and contrast-enhanced ultrasound[J]. J Ultrasound Med, 2023, 42(3): 623-634. doi: 10.1002/jum.16058 [25] Huang Y, Le J, Miao A, et al. Prediction of treatment responses to neoadjuvant chemotherapy in breast cancer using contrast-enhanced ultrasound[J]. Gland Surg, 2021, 10(4): 1280-1290. doi: 10.21037/gs-20-836 [26] Ioannidis G S, Goumenakis M, Stefanis I, et al. Quantification and classification of contrast enhanced ultrasound breast cancer data: A preliminary study[J]. Diagnostics, 2022, 12(2): 425. doi: 10.3390/diagnostics12020425 [27] 叶细容, 江峰, 洪玮. 超声造影与DCE-MRI对乳腺癌患者新辅助化疗的评估价值[J]. 中国CT和MRI杂志, 2024, 22(2): 95-97. [28] Wan C, Zhou L, Li H, et al. Multiparametric contrast-enhanced ultrasound in early prediction of response to neoadjuvant chemotherapy and recurrence-free survival in breast cancer[J]. Diagnostics, 2023, 13(14): 2378. doi: 10.3390/diagnostics13142378 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 86
- HTML全文浏览量: 60
- PDF下载量: 14
- 被引次数: 0
