

Childhood Adverse Events and Their Correlation with FKBP5,ACTH,BDNF,and Cortisol in Susceptible and Resilient Drug-Using Populations
-
摘要:
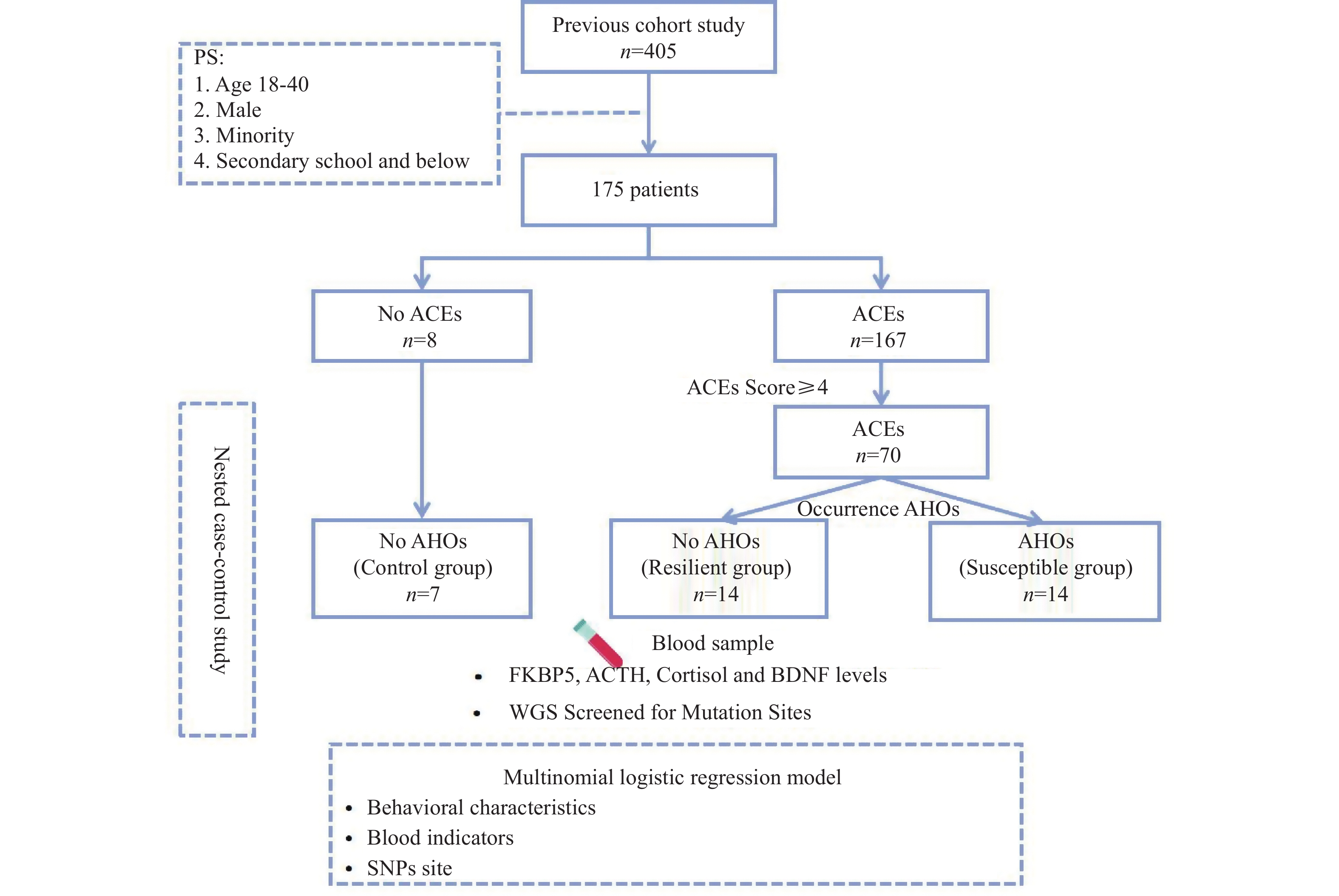
目的 探讨童年期负性事件与不良健康结局的关联,比较在童年期负性事件暴露下易感与弹性个体在FKBP5、ACTH、皮质醇、BDNF的差异。 方法 基于前期2021年1~7月建立的云南省405例吸毒人群的队列,采用巢式病例对照研究,检测对照组、弹性组及易感组的FKBP5、ACTH、皮质醇和BDNF水平;采用全基因组测序(whole genome sequencing,WGS)技术确定突变位点;运用SPSS 24.0和RStudio 4.3.1进行统计描述及多因素分析。 结果 对照组(n = 7)与弹性组(n = 14)的FKBP5水平存在显著差异[(4.67±1.08) vs. (6.86±1.87) ng/mL,P < 0.05]。与对照组相比,易感组(n = 14)的ACTH水平升高[(54.05±8.75) pg/mL,P < 0.05];与易感组相比,弹性组的ACTH水平升高[(67.28±8.36) pg/mL,P < 0.05]。皮质醇水平在对照组与易感组[(254.92±70.46) vs. (278.50±49.60) nmol/L,P < 0.05]以及易感组与弹性组[(278.50±49.60) vs. (406.27±72.07) nmol/L,P < 0.05]之间均存在显著差异。多元Logistic回归分析显示,以对照组为参照,弹性组的FKBP5、皮质醇及rs34224676基因型水平均存在显著差异(OR = 3.62,95%CI:1.36~9.64,P < 0.05;OR = 1.02,95%CI:1.00~1.04,P < 0.05;OR = 185.34,95%CI:69.56~493.83,P < 0.05)。 结论 有ACEs暴露的吸毒人群FKBP5、ACTH和皮质醇水平高于无ACEs暴露者。在ACEs暴露下,吸毒人群中FKBP5、皮质醇及SNPs位点rs34224676的表达可能与弹性现象有关。 Abstract:Object To investigate the association between adverse childhood experiences (ACEs) and adverse health outcomes (AHOs), and to compare the levels of FKBP5, ACTH, cortisol, and BDNF between susceptible and resilient individuals exposed to ACEs during childhood. Methods Based on a cohort of 405 individuals with substance use disorder in Yunnan Province established from January to July 2021, a nested case-control study was conducted. FKBP5, ACTH, cortisol, and BDNF levels were detected in the control group, resilient group and susceptible group. Whole-genome sequencing (WGS) technology was used to identify mutation sites Descriptive, univariate and multivariate analyses were conducted using SPSS 24.0 and R Studio version 4.3.1.n Results Significant differences in FKBP5 levels were found between the control group (n = 7) and resilient groups (n = 14) [(4.67±1.08) vs. (6.86±1.87) ng/mL, P < 0.05]. Compared with the control group, ACTH levels in the susceptible group (n = 14) were elevated [(54.05±8.75) pg/mL, P < 0.05]; compared with the susceptible group, ACTH levels in the resilient group were elevated [(67.28±8.36) pg/mL, P < 0.05]. Cortisol levels showed significant differences between the control and susceptible groups [(254.92±70.46) vs. (278.50±49.60) nmol/L, P < 0.05] and between the susceptible and resilient groups [(278.50±49.60) vs. (406.27±72.07) nmol/L, P < 0.05]. Multivariate logistic regression analysis showed that, with the control group as reference, the resilient group had significant differences in FKBP5, cortisol, and rs34224676 genotype levels (OR = 3.62, 95%CI: 1.36~9.64, P < 0.05; OR = 1.02, 95%CI: 1.00~1.04, P < 0.05; OR = 185.34, 95%CI: 69.56~493.83, P < 0.05). Conclusion Individuals with substance use disorder exposed to ACEs exhibited higher levels of FKBP5, ACTH, and cortisol compared to those without ACEs exposure. Under ACEs exposure, the expression of FKBP5, cortisol, and the SNP locus rs34224676 in individuals with substance use disorder may be associated with the resilience phenomena. -
Key words:
- Adverse childhood experiences /
- FKBP5 /
- ACTH /
- Resilience /
- Susceptibility
-
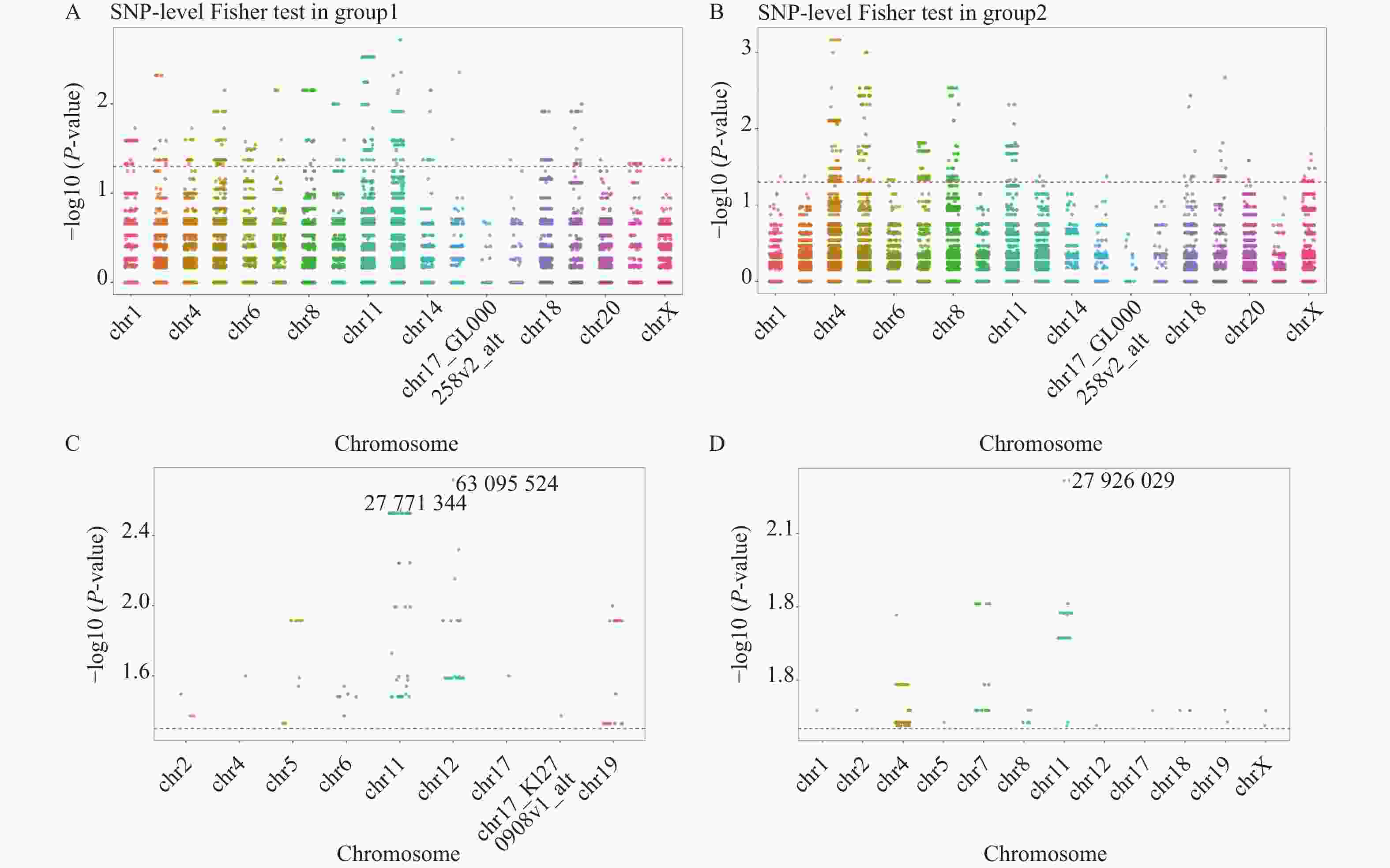
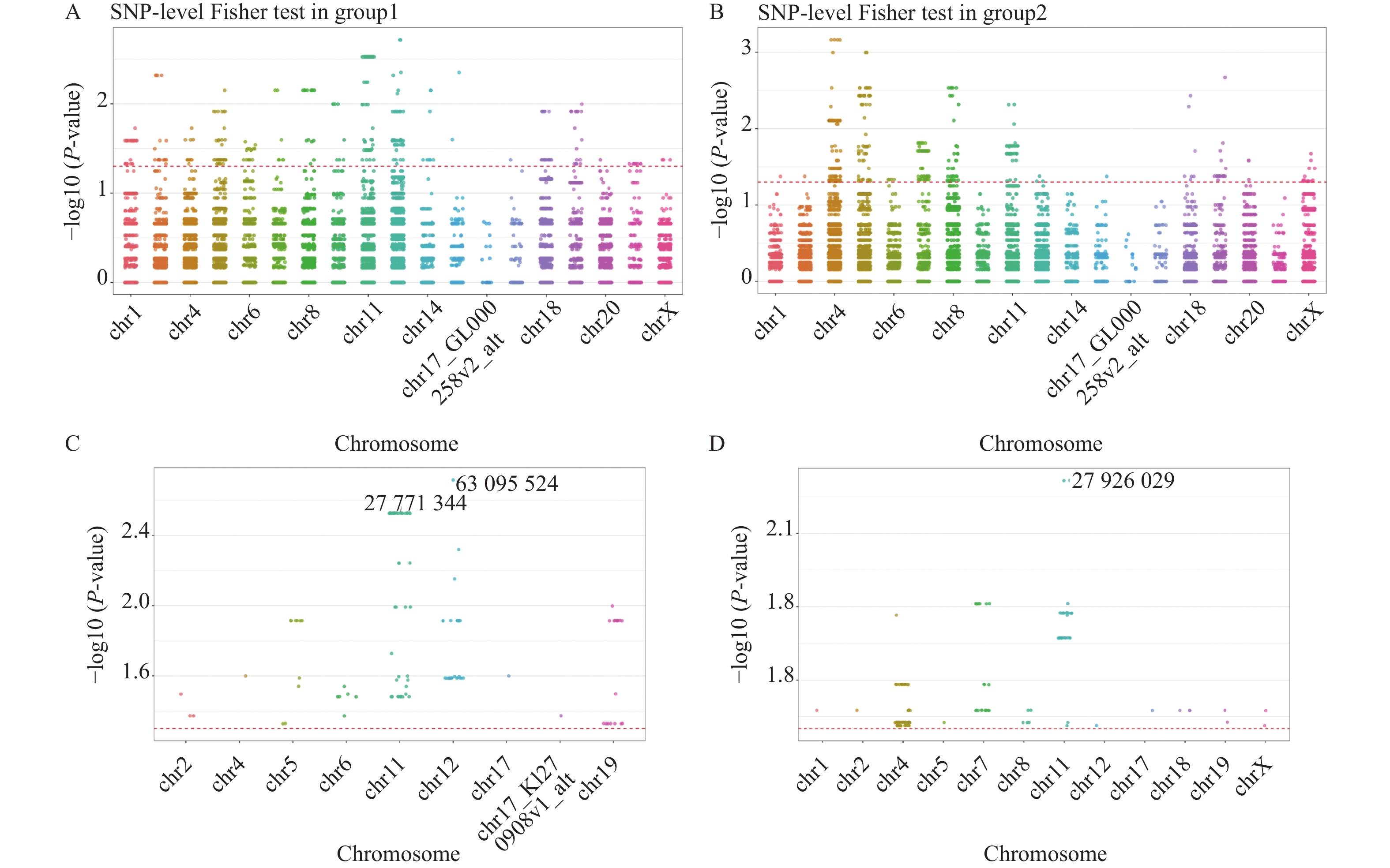
图 2 基于Fisher精确检验的曼哈顿图
A:对照组和其他组比较;B:易感组与弹性组比较;C:对照组和其他组间差异显著的基因位点;D:易感组与弹性组差异显著的基因位点。
Figure 2. Manhattan plot based on the Fisher exact test
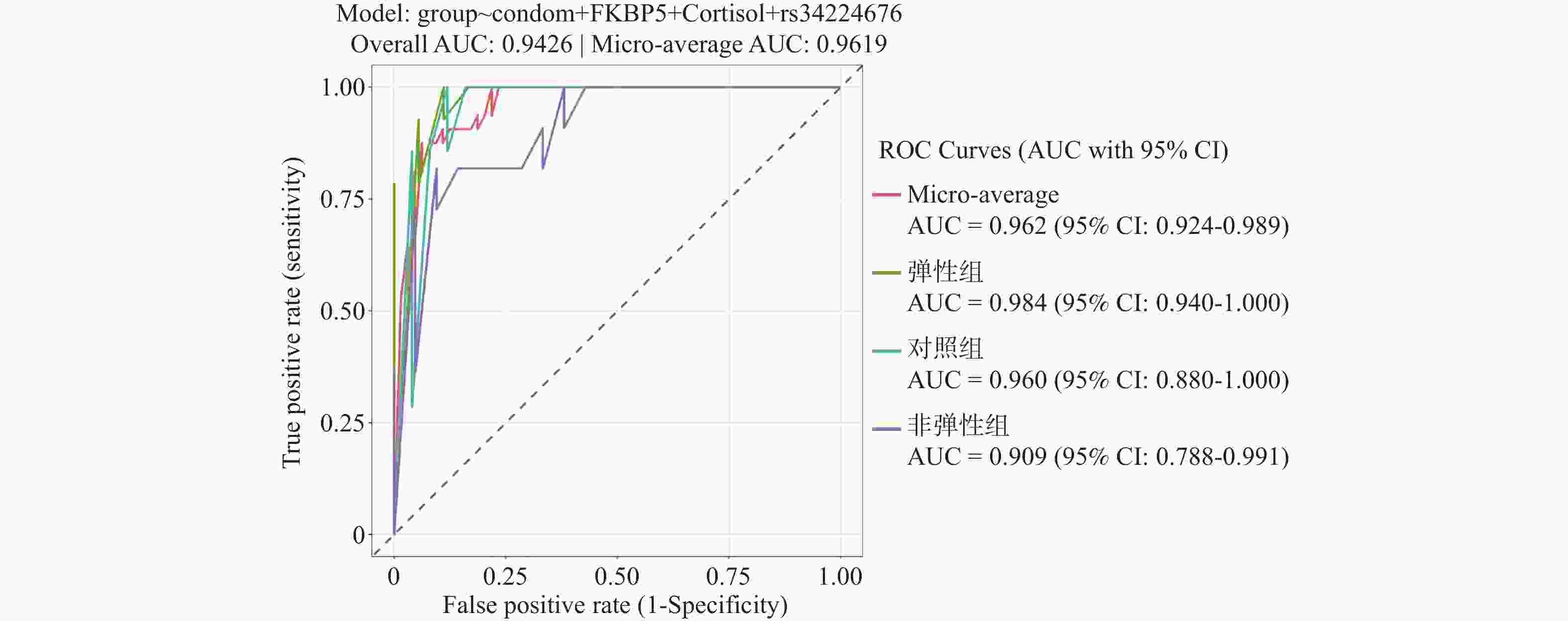
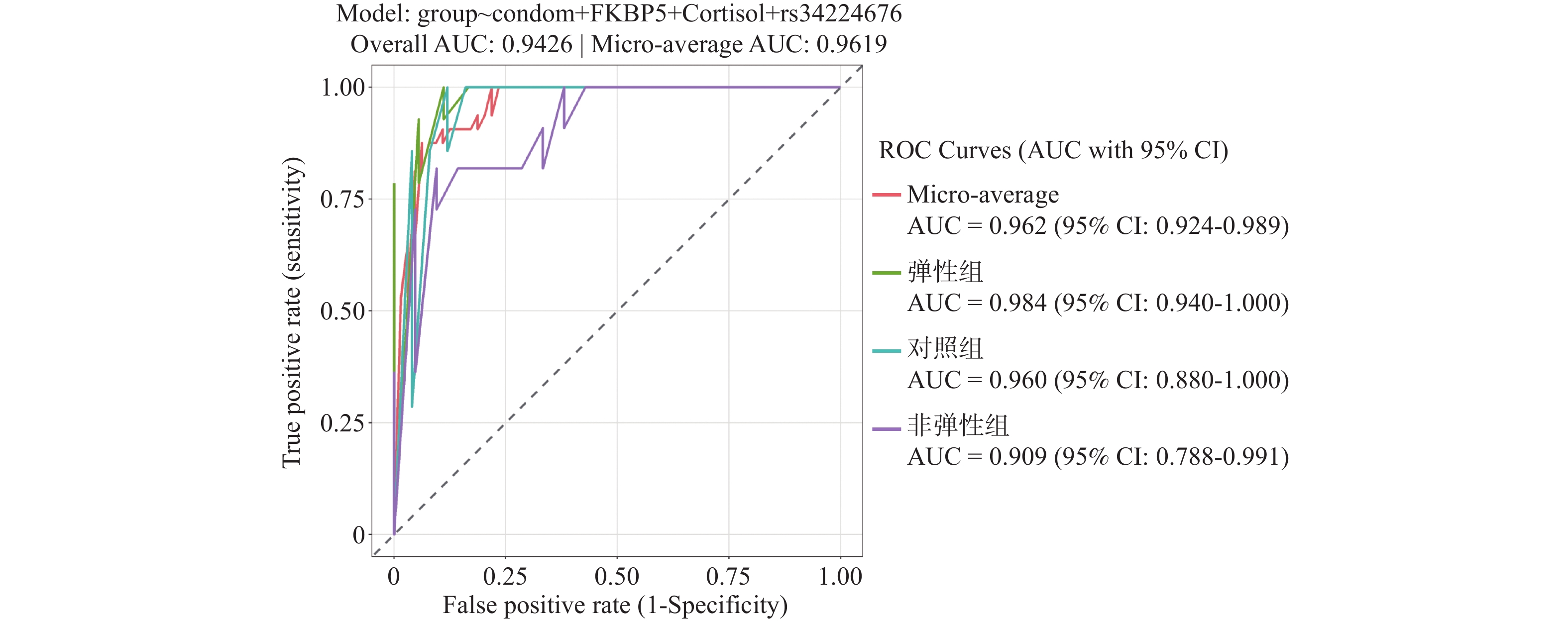
图 3 多分类模型的微平均ROC曲线
Figure 3. Micro-average ROC curve of the multi-classification model
表 1 对照组、弹性组和易感组中社会人口学特征分析[n(%)]
Table 1. Sociodemographic characteristics in the control,resilient and susceptibility groups[n(%)]
变量 总计 单因素分析 多元Logistic回归 对照组 弹性组 易感组 P 弹性组(Ref.对照组) P 易感组(Ref.对照组) P (n=7) (n=14) (n=14) OR(95%CI) OR(95%CI) 毒品种类 0.671 0.606 0.831 安非他命类 33(94.3) 6(85.7) 13(92.9) 14(100) Ref. Ref. 阿片类/其他 2(5.7) 1(14.3) 1(7.1) 0 0.462(0.025,8.700) 0.001(0.00,1.139) 使用年限(年) 0.254 0.135 0.744 <10 19(54.3) 5(71.4) 5(35.7) 9(64.3) Ref. Ref. ≥10 16(45.7) 2(28.6) 9(64.3) 5(35.7) 4.501(0.627,32.301) 1.389(0.194,9.970) 使用频率 0.613 0.355 0.355 每月1次/更少 21(60.0) 3(42.9) 9(64.3) 9(64.3) Ref. Ref. 每周2~6天/每天 14(30.0) 4(57.1) 5(35.7) 5(35.7) 0.417(0.065,2.660) 0.417(0.065,2.660) 使用方式 1.000 1.000 1.000 烫吸/抽吸/嗦吸 25(71.4) 5(71.4) 10(71.4) 10(71.4) Ref. Ref. 吞咽/其他 10(28.6) 2(28.6) 4(28.6) 4(28.6) 0.999(0.134,7.451) 0.999(0.134,7.451) 饮酒 0.228 0.694 0.323 否 31(88.6) 6 (85.7) 14 (100) 11 (78.6) Ref. Ref. 是 4(11.4) 1(14.3) 0 3(21.4) 0.822 (0.308,2.190) 0.610 (0.229,1.625) 婚姻状况 0.602 0.004* <0.001* 未婚/离异/未知 6(17.1) 0 3(21.4) 3(21.4) Ref. Ref. 已婚/有配偶 29(82.9) 7(100) 11(78.6) 11(78.6) 4.185 (1.571,11.151) 38.080 (14.292,101.462) 经济来源 0.296 0.463 0.600 工作收入 21(60.0) 5 (71.4) 6 (42.9) 10 (71.4) Ref. Ref. 他人救济 14(40.0) 2 (28.6) 8 (57.1) 4 (28.6) 0.693 (0.260,1.846) 1.300 (0.488,3.463) 育有子女 0.684 0.550 <0.001* 无 9(25.7) 1 (14.3) 3 (21.4) 5 (35.7) Ref. Ref. 有 26(74.3) 6 (85.7) 11(78.6) 9(64.3) 1.348 (0.506,3.592) 0.092 (0.035,0.246) 安全套的使用 0.671 <0.001* 0.117 从未/偶尔使用 2(5.7) 1 (14.3) 1 (7.1) 0 Ref. Ref. 每次使用 33(94.3) 6 (85.7) 13(92.9) 14(100) 0.106 (0.040,0.281) 0.457 (0.171,1.217) 多性伴模式 0.002* 0.635 <0.001* 否 24(68.6) 4 (57.1) 14 (100) 6 (42.9) Ref. Ref. 是 11(31.4) 3(42.9) 0 8(57.1) 0.789 (0.296,2.101) 21.663 (8.130,57.719) 注:单因素分析采用Fisher确切概率法;*P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 三个组的FKBP5、ACTH、皮质醇和BDNF水平差异分析
Table 2. Differences in FKBP5,ACTH,cortisol,and BDNF levels among the three groups
变量 总计 单因素分析 多因素分析 对照组 弹性组 易感组 P 弹性组
(Ref. 对照组)P 易感组
(Ref. 对照组)P (n=7) (n=14) (n=14) OR(95%CI) OR(95%CI) FKBP5 5.83 ± 1.86 4.67 ± 1.08 6.86 ± 1.87 5.38 ± 1.79 0.015*# 4.05(3.87,4.25) <0.001* 2.69(0.80,9.07) 0.111 ACTH 59.12 ± 11.94 52.96 ± 15.23 67.28 ± 8.36 54.05 ± 8.75 0.002*▲ 0.95(0.22,4.07) 0.949 1.07(0.79,1.43) 0.672 皮质醇 324.89 ± 91.78 254.92 ± 70.46 406.27 ± 72.07 278.50 ± 49.60 <0.001*#▲ 1.24(1.15,1.33) <0.001* 1.04(0.99,1.09) 0.170 BDNF 10.24 ± 2.39 9.37 ± 2.77 11.78 ± 2.33 9.15 ± 1.34 0.005*▲ 0.53(0.42,0.67) <0.001* 0.29(0.04,1.99) 0.206 注:单因素分析采用方差分析;对照组与弹性组相比#P < 0.05;弹性组与易感组相比▲P < 0.05;*P < 0.05;本研究样本量较小,采用Firth偏倚校正逻辑回归进行分析。
下载: 导出CSV
表 3 弹性组与易感组多元Logistic回归模型
Table 3. Multivariate Logistic regression model for the resilient and susceptible group
变量 弹性组(Ref. 对照组)a P 易感组(Ref. 对照组)a P OR(95%CI)b OR(95%CI)b 社会人口学特征 0.828 <0.001* 安全套的使用 从未/偶尔使用 Ref. Ref. 每次使用 0.90(0.33~2.39) 0.19(0.07~0.51) 血液指标 FKBP5 3.62(1.36~9.64) <0.001* 1.53(0.57~4.07) 0.301 皮质醇 1.02(1.00~1.04) 0.032* 0.99(0.38~2.66) 0.968 SNP 位点 <0.001* 0.027* rs34224676 无 Ref. Ref. 有 185.34(69.56~493.83) 17.58(6.60~46.84) 注:a以对照组作为参考;b本研究样本量较小且数据完全删失,因此采用Firth偏倚校正逻辑回归进行分析;*P < 0.05。
下载: 导出CSV
-
[1] Felitti V J, Anda R F, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ace) study[J]. Am J Prev Med, 1998, 14(4): 245-258. doi: 10.1016/S0749-3797(98)00017-8 [2] Madigan S, Deneault A A, Racine N, et al. Adverse childhood experiences: A meta-analysis of prevalence and moderators among half a million adults in 206 studies[J]. World Psychiatry, 2023, 22(3): 463-471. doi: 10.1002/wps.21122 [3] Madigan S, Thiemann R, Deneault A A, et al. Prevalence of adverse childhood experiences in child population samples: A systematic review and meta-analysis[J]. JAMA Pediatr, 2025, 179(1): 19-33. doi: 10.1001/jamapediatrics.2024.4385 [4] Whitaker R C, Dearth-Wesley T, Herman A N, et al. Association of childhood family connection with flourishing in young adulthood among those with type 1 diabetes[J]. JAMA Netw Open, 2020, 3(3): e200427. doi: 10.1001/jamanetworkopen.2020.0427 [5] Godoy L C, Frankfurter C, Cooper M, et al. Association of adverse childhood experiences with cardiovascular disease later in life: A review[J]. JAMA Cardiol, 2021, 6(2): 228-235. doi: 10.1001/jamacardio.2020.6050 [6] Wen S, Zhu J, Han X, et al. Childhood maltreatment and risk of endocrine diseases: An exploration of mediating pathways using sequential mediation analysis[J]. BMC Med, 2024, 22(1): 59. doi: 10.1186/s12916-024-03271-9 [7] Beatty A, Shepard E, Bickford E, et al. Adverse childhood experiences and prescription stimulant use in adults: A systematic review [J]. Pharmacy (Basel), 2024, 12(2). [8] Li J, Li M, Zhang Y, et al. Amphetamine-type stimulants use and socio-economic factors associated with hepatitis c antibody positivity among border drug users in south of china[J]. Front Public Health, 2022, 10: 998768. doi: 10.3389/fpubh.2022.998768 [9] Grummitt L, Barrett E, Kelly E, et al. An umbrella review of the links between adverse childhood experiences and substance misuse: What, why, and where do we go from here?[J]. Subst Abuse Rehabil, 2022, 13: 83-100. doi: 10.2147/SAR.S341818 [10] Chang X, Jiang X, Mkandarwire T, et al. Associations between adverse childhood experiences and health outcomes in adults aged 18-59 years[J]. PLoS One, 2019, 14(2): e0211850. doi: 10.1371/journal.pone.0211850 [11] Okwori G. Role of individual, family, and community resilience in moderating effects of adverse childhood experiences on mental health among children[J]. J Dev Behav Pediatr, 2022, 43(7): e452-e462. doi: 10.1097/DBP.0000000000001076 [12] McGowan E C, Oyeku S O, Lim S W. Family, neighborhood and parent resilience are inversely associated with reported depression in adolescents exposed to aces[J]. Acad Pediatr, 2023, 23(4): 773-781. doi: 10.1016/j.acap.2022.10.009 [13] Lensch T, Clements-Nolle K, Oman R F, et al. Adverse childhood experiences and suicidal behaviors among youth: The buffering influence of family communication and school connectedness[J]. J Adolesc Health, 2021, 68(5): 945-952. doi: 10.1016/j.jadohealth.2020.08.024 [14] He J, Yan X, Wang R, et al. Does childhood adversity lead to drug addiction in adulthood? A study of serial mediators based on resilience and depression[J]. Front Psychiatry, 2022, 13: 871459. doi: 10.3389/fpsyt.2022.871459 [15] Niu L, Gao Q, Xie M, et al. Association of childhood adversity with hpa axis activity in children and adolescents: A systematic review and meta-analysis[J]. Neurosci Biobehav Rev, 2025, 172: 106124. doi: 10.1016/j.neubiorev.2025.106124 [16] Ikram N, Frost A, LeMasters K, et al. Adverse childhood experiences and implications of perceived stress, anxiety and cortisol among women in pakistan: A cross-sectional study[J]. BMJ Open, 2022, 12(4): e052280. doi: 10.1136/bmjopen-2021-052280 [17] Marques-Feixa L, Palma-Gudiel H, Romero S, et al. Childhood maltreatment disrupts hpa-axis activity under basal and stress conditions in a dose-response relationship in children and adolescents[J]. Psychol Med, 2023, 53(3): 1060-1073. doi: 10.1017/S003329172100249X [18] Taylor K S, Steptoe A, Iob E. The relationship of adverse childhood experiences, hair cortisol, c-reactive protein, and polygenic susceptibility with older adults' psychological distress during the covid-19 pandemic[J]. Mol Psychiatry, 2022, 27(12): 5038-5048. doi: 10.1038/s41380-022-01805-2 [19] Herzog S, Galfalvy H, Keilp J G, et al. Relationship of stress-reactive cortisol to suicidal intent of prior attempts in major depression[J]. Psychiatry Res, 2023, 327: 115315. doi: 10.1016/j.psychres.2023.115315 [20] Goltser-Dubner T, Benarroch F, Lavon M, et al. Childhood trauma cortisol and immune cell glucocorticoid transcript levels are associated with increased risk for suicidality in adolescence[J]. Mol Psychiatry, 2025, 30(8): 3376-3383. doi: 10.1038/s41380-025-02923-3 [21] Cullen A E, Fisher H L, Gullet N, et al. Cortisol levels in childhood associated with emergence of attenuated psychotic symptoms in early adulthood[J]. Biol Psychiatry, 2022, 91(2): 226-235. doi: 10.1016/j.biopsych.2021.08.009 [22] Pallardo-Fernández I, García-Marchena N, Rodríguez-Rivera C, et al. Plasma midkine levels in patients with cocaine use disorder during abstinence[J]. Adicciones, 2022, 34(4): 273-278. [23] Demakakos P, Steptoe A. Adverse childhood experiences and diurnal cortisol patterns in older people in england[J]. Psychoneuroendocrinology, 2022, 142: 105798. doi: 10.1016/j.psyneuen.2022.105798 [24] Noddings C M, Johnson J L, Agard D A. Cryo-em reveals how hsp90 and fkbp immunophilins co-regulate the glucocorticoid receptor[J]. Nat Struct Mol Biol, 2023, 30(12): 1867-1877. doi: 10.1038/s41594-023-01128-y [25] Zhang Y, Yue W, Li J. The association of fkbp5 gene polymorphism with genetic susceptibility to depression and response to antidepressant treatment- a systematic review[J]. BMC Psychiatry, 2024, 24(1): 274. doi: 10.1186/s12888-024-05717-z [26] Misiak B, Karpiński P, Szmida E, et al. Adverse childhood experiences and methylation of the fkbp5 gene in patients with psychotic disorders [J]. J Clin Med, 2020, 9(12). [27] Rodríguez-Carrillo A, Verheyen V J, Van Nuijs A L N, et al. Brain-derived neurotrophic factor (bdnf): An effect biomarker of neurodevelopment in human biomonitoring programs [J]. Frontiers in Toxicology, 2024, Volume 5 - 2023. [28] Vyas N, Wimberly C E, Beaman M M, et al. Systematic review and meta-analysis of the effect of adverse childhood experiences (aces) on brain-derived neurotrophic factor (bdnf) levels[J]. Psychoneuroendocrinology, 2023, 151: 106071. doi: 10.1016/j.psyneuen.2023.106071 [29] Chan J C, Lee C T, Say Y H, et al. Exercise as a mediator between childhood adversity and psychological distress: Can bdnf moderate the mediating effect?[J]. J Psychiatr Res, 2025, 182: 277-283. doi: 10.1016/j.jpsychires.2025.01.017 [30] Yeh Y W, Chen C S H, Kuo S C, et al. Childhood trauma, family functioning, and the bdnf gene may affect the development of alcohol use disorder[J]. Drug Alcohol Depend, 2026, 278: 112987. doi: 10.1016/j.drugalcdep.2025.112987 [31] 李佳霜, 王沛, 李静, et al. 边境吸毒人群童年期负性事件与成年期不良健康结局的研究[J]. 中国药物依赖性杂志, 2023, 32(6): 535-540. [32] Bernstein D P, Stein J A, Newcomb M D, et al. Development and validation of a brief screening version of the childhood trauma questionnaire[J]. Child Abuse Negl, 2003, 27(2): 169-190. doi: 10.1016/S0145-2134(02)00541-0 [33] Grant B F, Goldstein R B, Saha T D, et al. Epidemiology of dsm-5 alcohol use disorder: Results from the national epidemiologic survey on alcohol and related conditions iii[J]. JAMA Psychiatry, 2015, 72(8): 757-766. [34] Urkin B, Parnas J, Raballo A, et al. Clinical activity and psychopathological knowledge are related to real-world performance of leading international psychiatrists in diagnosing schizophrenia spectrum disorders [J]. Psychopathology, 2025: 1–7. [35] World Health Organization. Self-collection of samples for sexually transmitted infections(stis)[EB/OL](2020-06-12)[2026-05-15]. https://www.who.int/publications/i/item/WHO-SRH-20.10. [36] Livne O, Shmulewitz D, Stohl M, et al. Agreement between dsm-5 and dsm-iv measures of substance use disorders in a sample of adult substance users[J]. Drug Alcohol Depend, 2021, 227: 108958. doi: 10.1016/j.drugalcdep.2021.108958 [37] 中华人民共和国国家卫生健康委员会. 静脉血液标本采集指南[EB/OL] (2020-04-15)[2026-05-15]. https://www.nhc.gov.cn/wjw/s9492/202004/c09a4128e8194e40baad2498fd8a1f26.shtml. [38] Jin Y, Lu R, Wang M, et al. Analysis of blood screening strategies and their efficacy among voluntary blood donors in a region of east china[J]. PLoS One, 2025, 20(8): e0331027. doi: 10.1371/journal.pone.0331027 [39] Zhang S, Cheon M, Park H, et al. Interaction between glucocorticoid receptors and fkbp5 in regulating neurotransmission of the hippocampus[J]. Neuroscience, 2022, 483: 95-103. doi: 10.1016/j.neuroscience.2021.12.020 [40] Nöthling J, Womersley J S, Mhlongo S, et al. The relationship between childhood trauma, rs1360780 genotypes, fkbp5 intron 7 methylation and posttraumatic stress disorder in women who have experienced rape[J]. Eur J Psychotraumatol, 2025, 16(1): 2485707. doi: 10.1080/20008066.2025.2485707 [41] Arancibia M, Manterola M, Ríos U, et al. The rs1360780 variant of fkbp5: Genetic variation, epigenetic regulation, and behavioral phenotypes [J]. Genes (Basel), 2025, 16(3). [42] Grasso D J, Drury S, Briggs-Gowan M, et al. Adverse childhood experiences, posttraumatic stress, and fkbp5 methylation patterns in postpartum women and their newborn infants[J]. Psychoneuroendocrinology, 2020, 114: 104604. doi: 10.1016/j.psyneuen.2020.104604 [43] Yang R, Xu C, Bierer L M, et al. Longitudinal genome-wide methylation study of ptsd treatment using prolonged exposure and hydrocortisone[J]. Transl Psychiatry, 2021, 11(1): 398. doi: 10.1038/s41398-021-01513-5 [44] Everson T M, Kaczor K, Makoroff K, et al. Epigenetic differences in stress response gene fkbp5 among children with abusive vs accidental injuries[J]. Pediatric Research, 2023, 94(1): 193-199. doi: 10.1038/s41390-022-02441-w [45] Karlbauer V N, Martins J, Rex-Haffner M, et al. Prenatal exposures and cell type proportions are main drivers of fkbp5 DNA methylation in maltreated and non-maltreated children[J]. Neurobiology of Stress, 2024, 33: 100687. doi: 10.1016/j.ynstr.2024.100687 [46] Souama C, Lamers F, Milaneschi Y, et al. The metabolomic signature of childhood trauma[J]. Biological Psychiatry, 2025, 98(10): 779-787. doi: 10.1016/j.biopsych.2025.03.018 [47] Nold V, Portenhauser M, Del Prete D, et al. Impact of fkbp5 × early life adversity × sex in humanised mice on multidimensional stress responses and circadian rhythmicity[J]. Molecular Psychiatry, 2022, 27(8): 3544-3555. doi: 10.1038/s41380-022-01549-z [48] Li Y, Jia H, Wei X, et al. Interaction of childhood trauma with bdnf and fkbp5 gene polymorphisms in predicting burnout in general occupational groups[J]. European Archives of Psychiatry and Clinical Neuroscience, 2025, 275(7): 1959-1968. doi: 10.1007/s00406-024-01825-9 [49] Yeshaw W M, Adhikari A, Chiang C Y, et al. Localization of ppm1h phosphatase tunes parkinson's disease-linked lrrk2 kinase-mediated rab gtpase phosphorylation and ciliogenesis[J]. Proc Natl Acad Sci U S A, 2023, 120(44): e2315171120. doi: 10.1073/pnas.2315171120 [50] Broniarczyk-Czarniak M, Szemraj J, Śmigielski J, et al. The role of oxt, oxtr, avp, and avpr1a gene expression in the course of schizophrenia[J]. Curr Issues Mol Biol, 2022, 44(1): 336-349. doi: 10.3390/cimb44010025 [51] Cahill S, Chandola T, Hager R. Genetic variants associated with resilience in human and animal studies [J]. Frontiers in Psychiatry, 2022, Volume 13 - 2022. [52] Malekpour M, Shekouh D, Safavinia M E, et al. Role of fkbp5 and its genetic mutations in stress-induced psychiatric disorders: An opportunity for drug discovery[J]. Front Psychiatry, 2023, 14: 1182345. doi: 10.3389/fpsyt.2023.1182345 [53] Ferrer A, Soria V, Salvat-Pujol N, et al. The role of childhood trauma, hpa axis reactivity and fkbp5 genotype on cognition in healthy individuals[J]. Psychoneuroendocrinology, 2021, 128: 105221. doi: 10.1016/j.psyneuen.2021.105221 [54] Kang J I, Kim T Y, Choi J H, et al. Allele-specific DNA methylation level of fkbp5 is associated with post-traumatic stress disorder[J]. Psychoneuroendocrinology, 2019, 103: 1-7. doi: 10.1016/j.psyneuen.2018.12.226 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 14
- HTML全文浏览量: 12
- PDF下载量: 3
- 被引次数: 0
