

Construction and Validation of a Nomogram for Predicting the Risk of Delirium in Patients with Acute Exacerbation of COPD Complicated by Respiratory Failure
-
摘要:
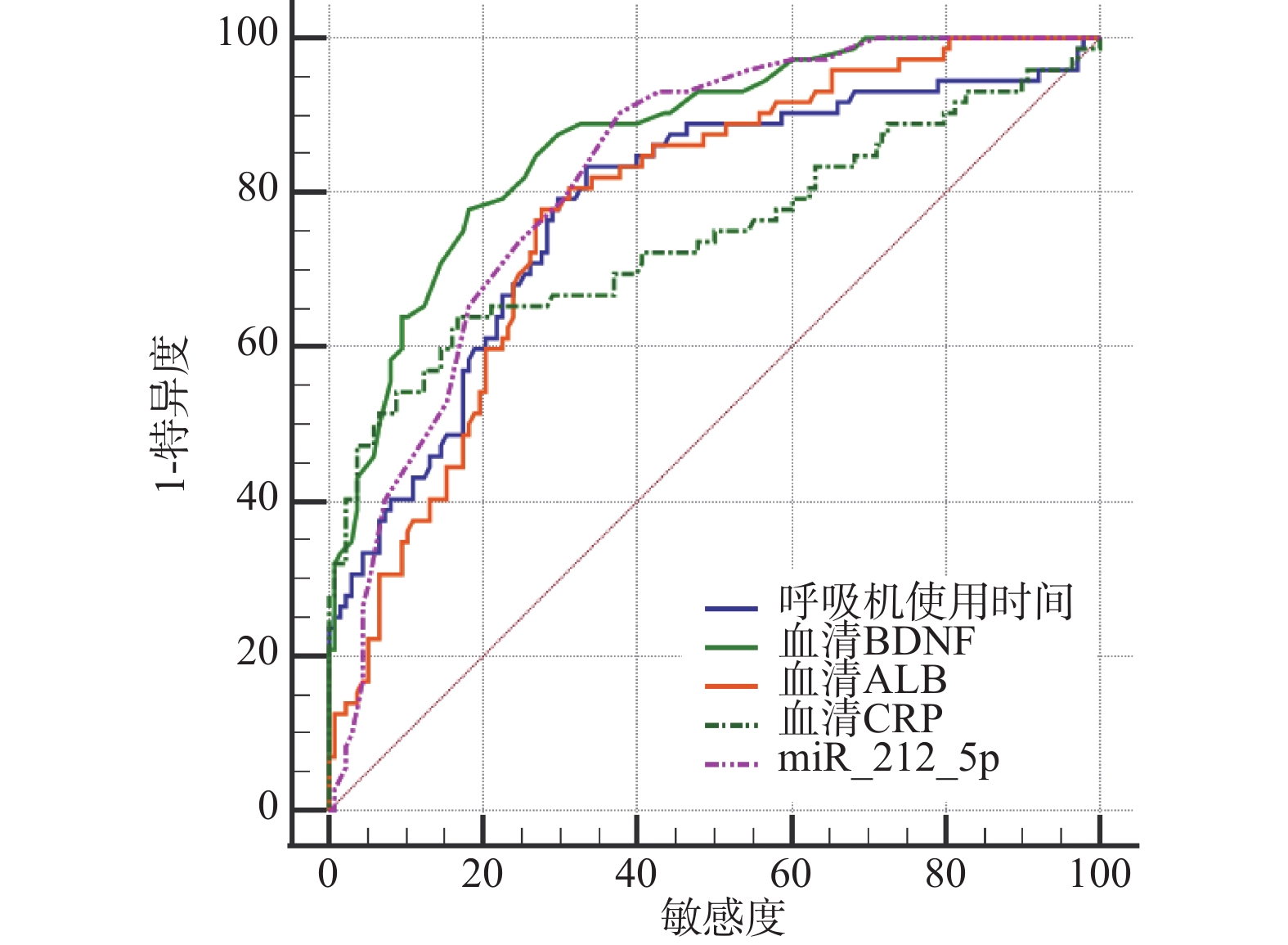
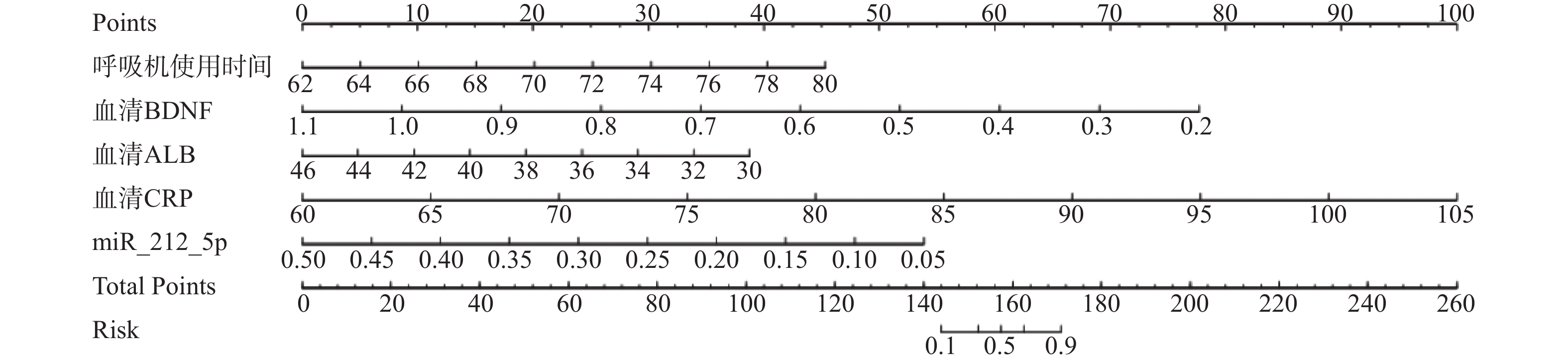
目的 探讨急性加重期慢性阻塞性肺疾病(acute exacerbation of chronic obstructive pulmonary disease,AECOPD)呼吸衰竭患者发生谵妄的影响因素,以此构建列线图预测模型,并评估该模型的预测效能。 方法 回顾性选取2023年3月至2025年3月安徽医科大学第一附属医院收治的210例AECOPD伴呼吸衰竭患者的临床资料作为观察对象,根据患者是否发生谵妄分为谵妄组(n = 72)及非谵妄组(n = 138)。比较两组一般基线资料,采用单因素和多因素Logistic回归分析AECOPD伴呼吸衰竭患者发生谵妄的影响因素。将发生谵妄纳入阳性,非谵妄纳入阴性,绘制受试者工作特征(receiver operating characteristic,ROC)曲线分析单因素中有差异的因素对AECOPD伴呼吸衰竭患者发生谵妄的预测价值。构建AECOPD伴呼吸衰竭患者谵妄发生风险预测的列线图模型并分析预测效果。 结果 两组呼吸机使用时间、动脉血氧分压(arterial partial pressure of oxygen,PaO2)、动脉血二氧化碳分压(partial pressure of carbon dioxide,PaCO2)、血清脑源性神经营养因子(brain-derived neurotrophic facto,BDNF)、白蛋白(albumin,ALB)、C反应蛋白(C-reactive protein,CRP)、微小核糖核酸-212-5p (microRNA,miR-212-5p)水平比较(P < 0.001)。多因素Logistic回归分析结果显示,呼吸机使用时间>72 h (OR = 1.082,95%CI:1.016~1.152,P = 0.014),血清BDNF≤0.64 μg/L(OR = 0.922,95%CI:0.859~0.99,P = 0.024)、ALB≤35 g/L(OR = 0.920,95%CI:0.875~0.968,P = 0.001)、miR-212-5p相对表达量≤0.27(OR = 0.927,95%CI:0.869~0.989,P = 0.021),血清CRP>76.95 mg/L(OR = 1.081,95%CI:1.023~1.142,P = 0.005)等均为AECOPD伴呼吸衰竭患者发生谵妄的独立危险因素。ROC曲线结果显示,呼吸机使用时间、血清BDNF、ALB、CRP、miR-212-5p水平预测AECOPD伴呼吸衰竭患者发生谵妄的AUC分别为0.807(0.745~0.859)、0.841 (0.783~0.889)、0.793(0.730~0.847)、0.745(0.61~0.803)、0.826(0.768~0.875),均具有较高的预测价值。进一步绘制ROC曲线结果发现,列线图模型预测AECOPD伴呼吸衰竭患者谵妄发生风险具有较好的预测能力(AUC=0.852,95%CI:0.797~0.897),Hosmer-Lemeshow拟合优度检验结果显示模型具有较高准确度(χ2 = 2.309,P = 0.970)。DCA曲线结果显示,当高风险阈值为0.0~0.4时,呼吸机使用时间、血清BDNF、ALB、CRP、miR-212-5p水平预测AECOPD伴呼吸衰竭患者谵妄发生风险的净获益率优于以上指标单独预测。 结论 呼吸机使用时间延长,血清BDNF、ALB、miR-212-5p水平降低,血清CRP水平升高均为AECOPD伴呼吸衰竭患者发生谵妄的影响因素,临床可借助以上因素辅助评估谵妄发生。 Abstract:Objective To explore the influencing factors of delirium in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) complicated by respiratory failure, and to construct a nomogram prediction model, and to evaluate the predictive efficacy of this model. Methods A retrospective analysis was conducted on clinical data from 210 patients with AECOPD complicated by respiratory failure admitted to the First Affiliated Hospital of Anhui Medical University from March 2023 to March 2025, serving as the observation cohort. Patients were stratified into a delirium group (n = 72) and a non-delirium group (n = 138) based on whether delirium occurred. General baseline data of the two groups were compared, and univariate and multivariate Logistic regression analyses were conducted to explore the influencing factors of delirium in patients with AECOPD with respiratory failure. With delirium occurrence designated as positive and absence of delirium as negative, receiver operating characteristic (ROC) curves were plotted to analyze the predictive value of factors with significant differences in univariate analysis for delirium development. A nomogram model was constructed to predict the risk of delirium in AECOPD patients with respiratory failure, and the predictive performance was analyzed. Results Between the two groups, significant differences were observed in mechanical ventilation duration, arterial partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), serum brain-derived neurotrophic factor (BDNF), albumin (ALB), C-reactive protein (CRP), and microRNA-212-5p (miR-212-5p) levels (P < 0.001). Multivariate Logistic regression analysis showed that mechanical ventilation duration > 72 hours (OR = 1.082, 95%CI: 1.016 ~1.152, P = 0.014), serum BDNF ≤ 0.64 μg/L (OR = 0.922, 95%CI: 0.859~0.99, P = 0.024), ALB ≤ 35 g/L (OR = 0.920, 95%CI: 0.875~0.968, P = 0.001), miR-212-5p relative expression≤ 0.27 (OR = 0.927, 95%CI: 0.869~0.989, P = 0.021), and serum CRP > 76.95 mg/L (OR = 1.081, 95%CI: 1.023~1.142, P = 0.005) were all independent risk factors for delirium in AECOPD patients with respiratory failure. ROC curve results showed that mechanical ventilation duration, serum BDNF, ALB, CRP, and miR-212-5p levels had AUCs of 0.807 (0.745~0.859), 0.841 (0.783~0.889), 0.793 (0.730~0.847), 0.745 (0.61~ 0.803), and 0.826 (0.768~0.875), respectively, all demonstrating high predictive value. Further analysis of the ROC curve revealed that the nomogram model demonstrated a good predictive ability for the risk of delirium in AECOPD patients with respiratory failure (AUC=0.852, 95%CI:0.797~0.897). Hosmer-Lemeshow goodness-of-fit test indicated high model accuracy (χ2 = 2.309, P = 0.970). Decision curve analysis (DCA) demonstrated that at high-risk thresholds of 0.0-0.4, the combined predictive value of mechanical ventilation duration, serum BDNF, ALB, CRP, and miR-212-5p levels for delirium risk in AECOPD patients with respiratory failure showed superior net benefit compared to individual indicators. Conclusion Prolonged mechanical ventilation duration, decreased serum BDNF, ALB and miR-212-5p levels, and the elevated serum CRP leves are all influencing factors for the occurrence of delirium in patients with AECOPD with respiratory failure. Clinically, these factors can serve as auxiliary tools for assessing delirium occurrence. these factors can be utilized to assist in the assessment of the occurrence of delirium. -
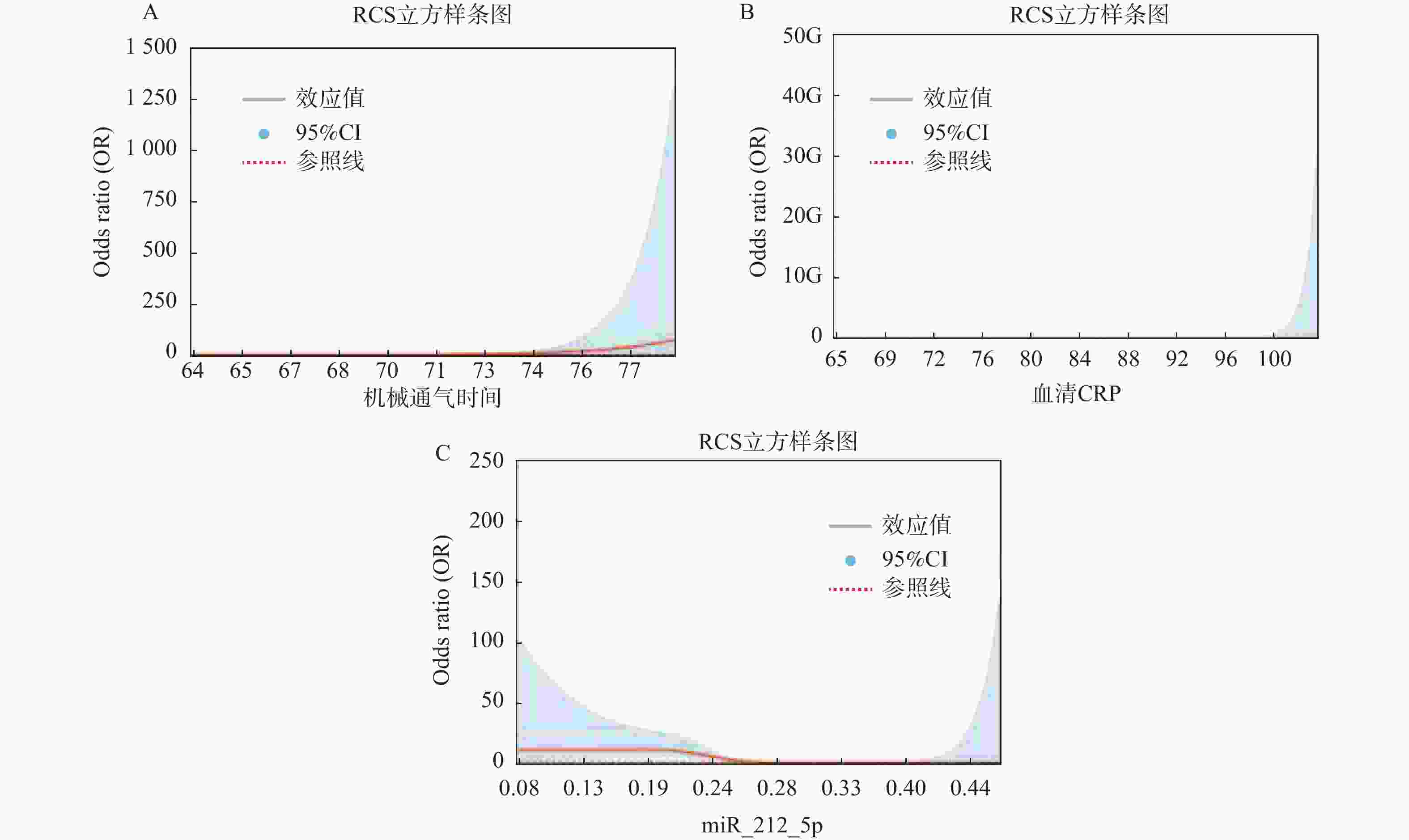
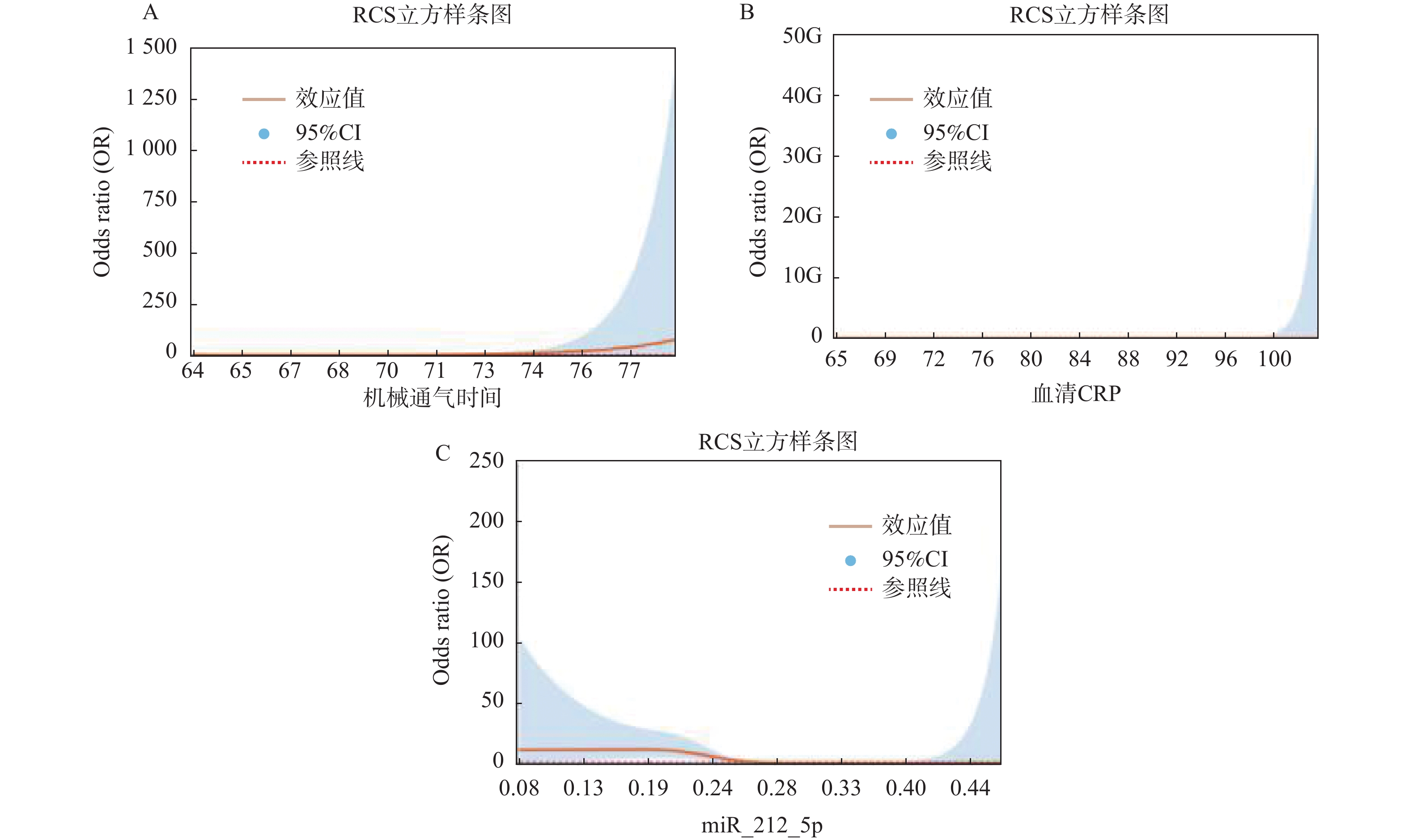
图 1 呼吸机使用时间、血清ALB、 miR-212-5p RCS立方样条图
A:呼吸机使用时间RCS立方样条图;B:血清ALBRCS立方样条图;C:miR-212-5p RCS立方样条图。
Figure 1. Cubic spline plot of mechanical ventilating duration,serum ALB,and miR-212-5p RCS
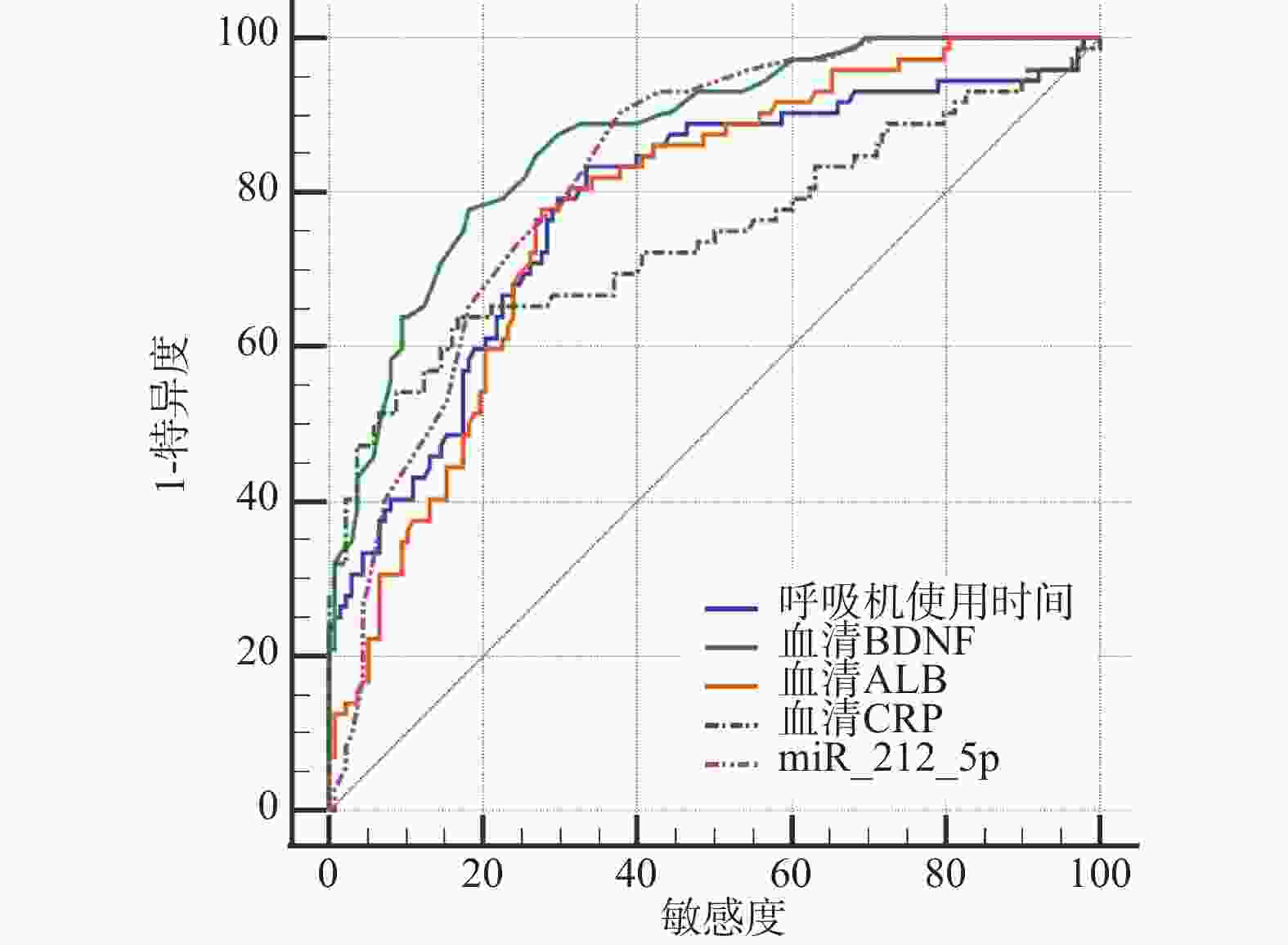
图 2 呼吸机使用时间、血清BDNF、ALB、CRP、miR-212-5p水平预测AECOPD伴呼吸衰竭患者发生谵妄的ROC曲线图
Figure 2. ROC curve showing the relationship between mechanical ventilating duration,serum BDNF,ALB,CRP,and miR-212-5p levels and the occurrence of delirium in patients with AECOPD and respiratory failure
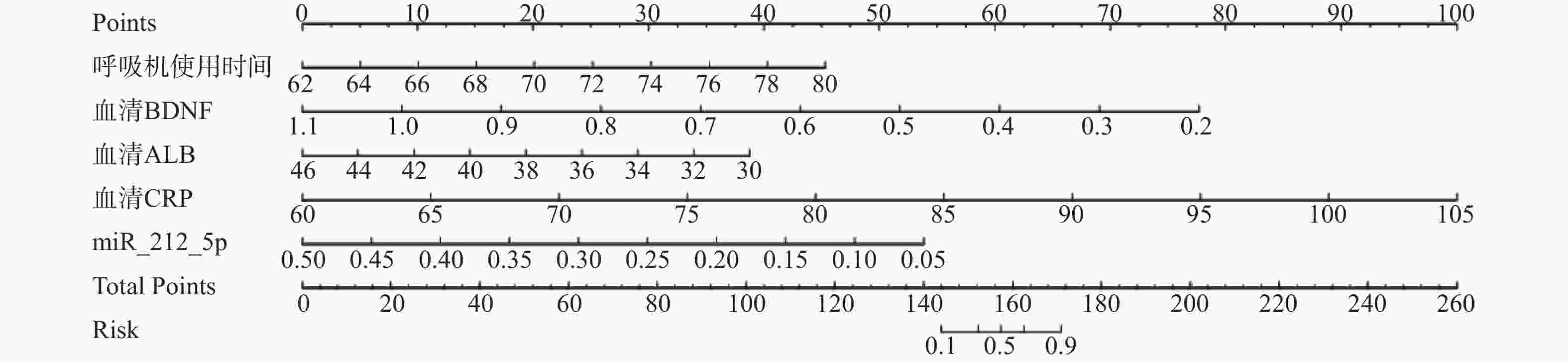
图 3 AECOPD伴呼吸衰竭患者谵妄发生的列线图可视化分析
Figure 3. Visualized analysis of the nomogram for the occurrence of delirium in patients with AECOPD and respiratory failure
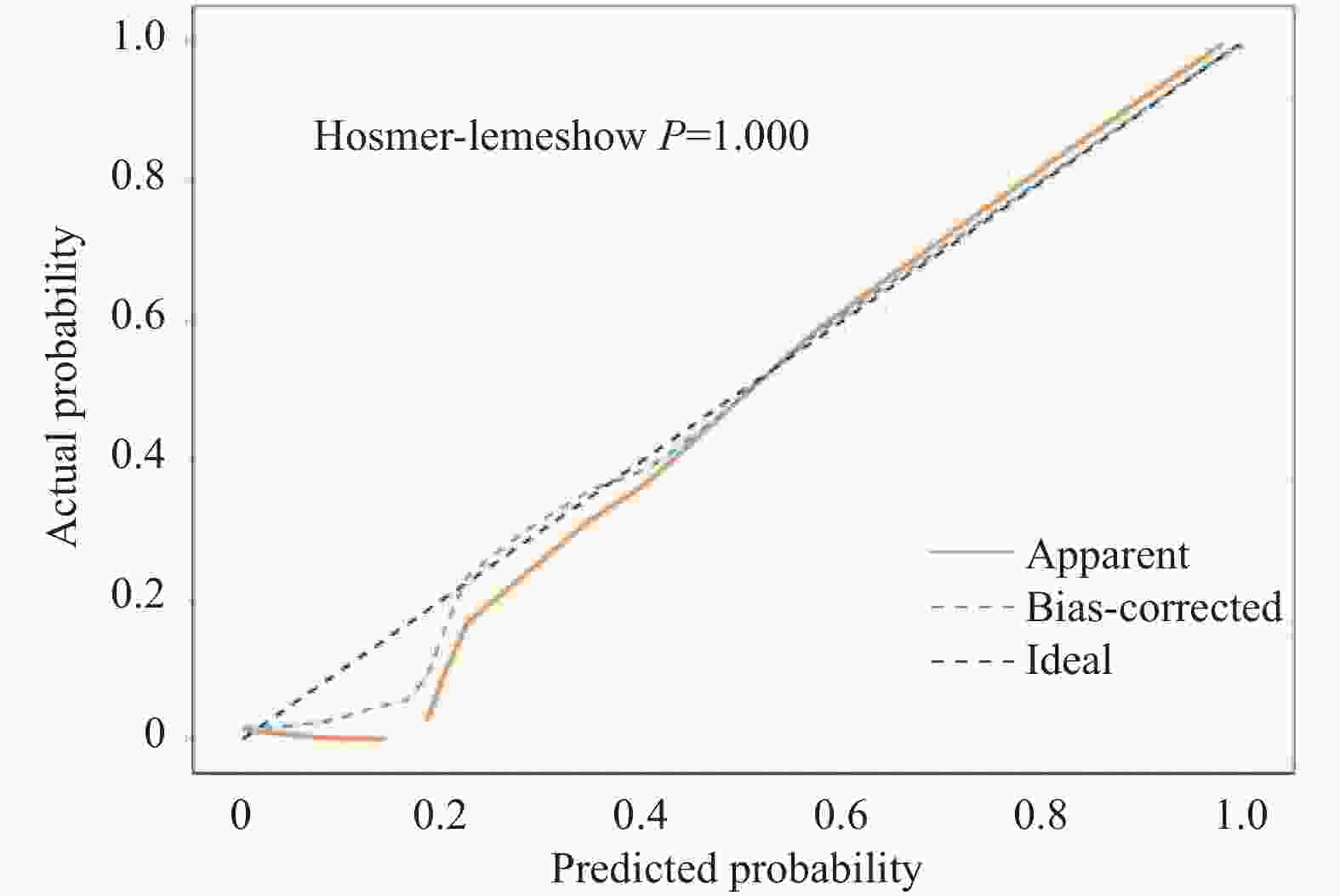
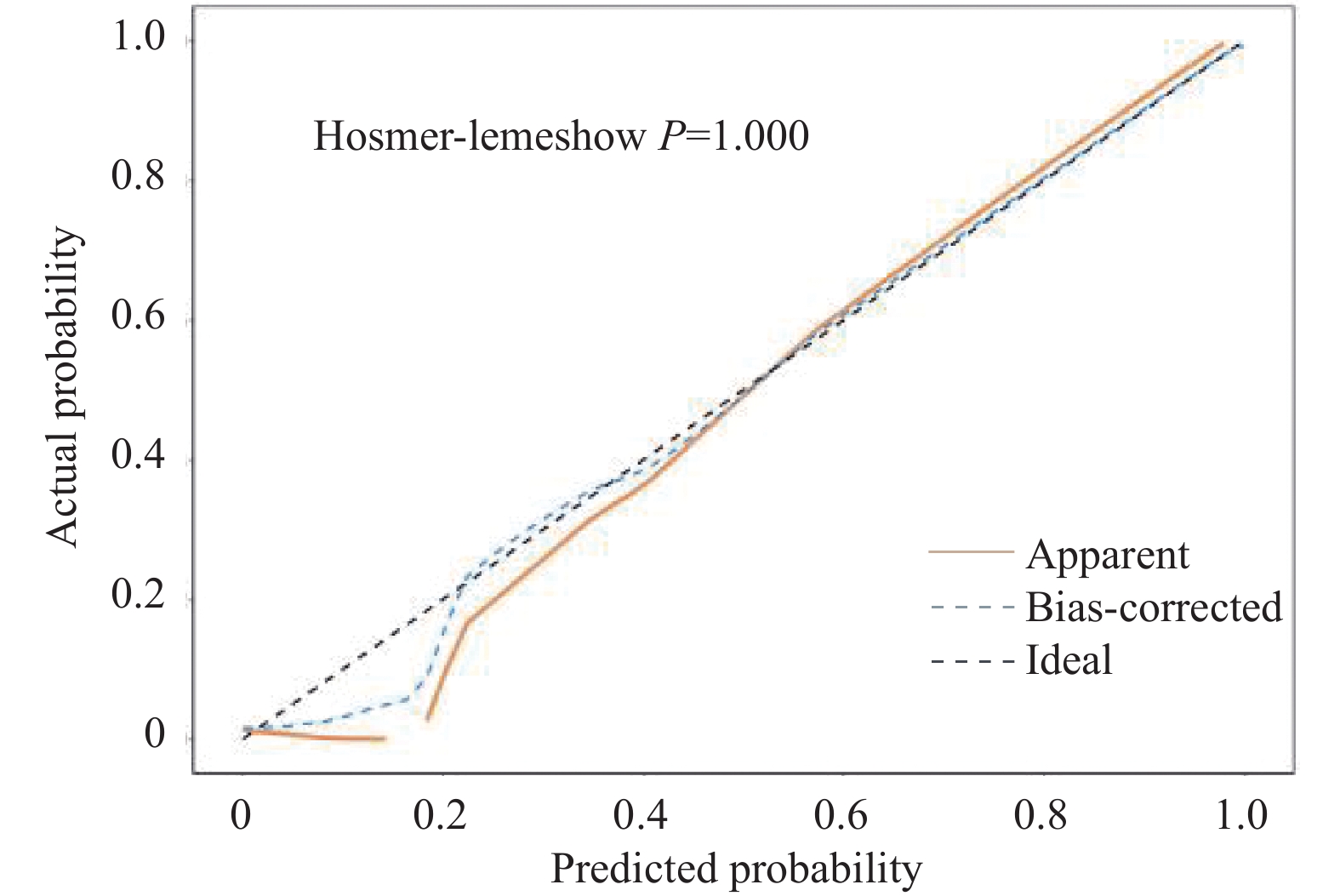
图 4 AECOPD伴呼吸衰竭患者发生谵妄的列线图模型校准曲线
Figure 4. Calibration curve of the nomogram model for predicting delirium in patients with AECOPD and respiratory failure
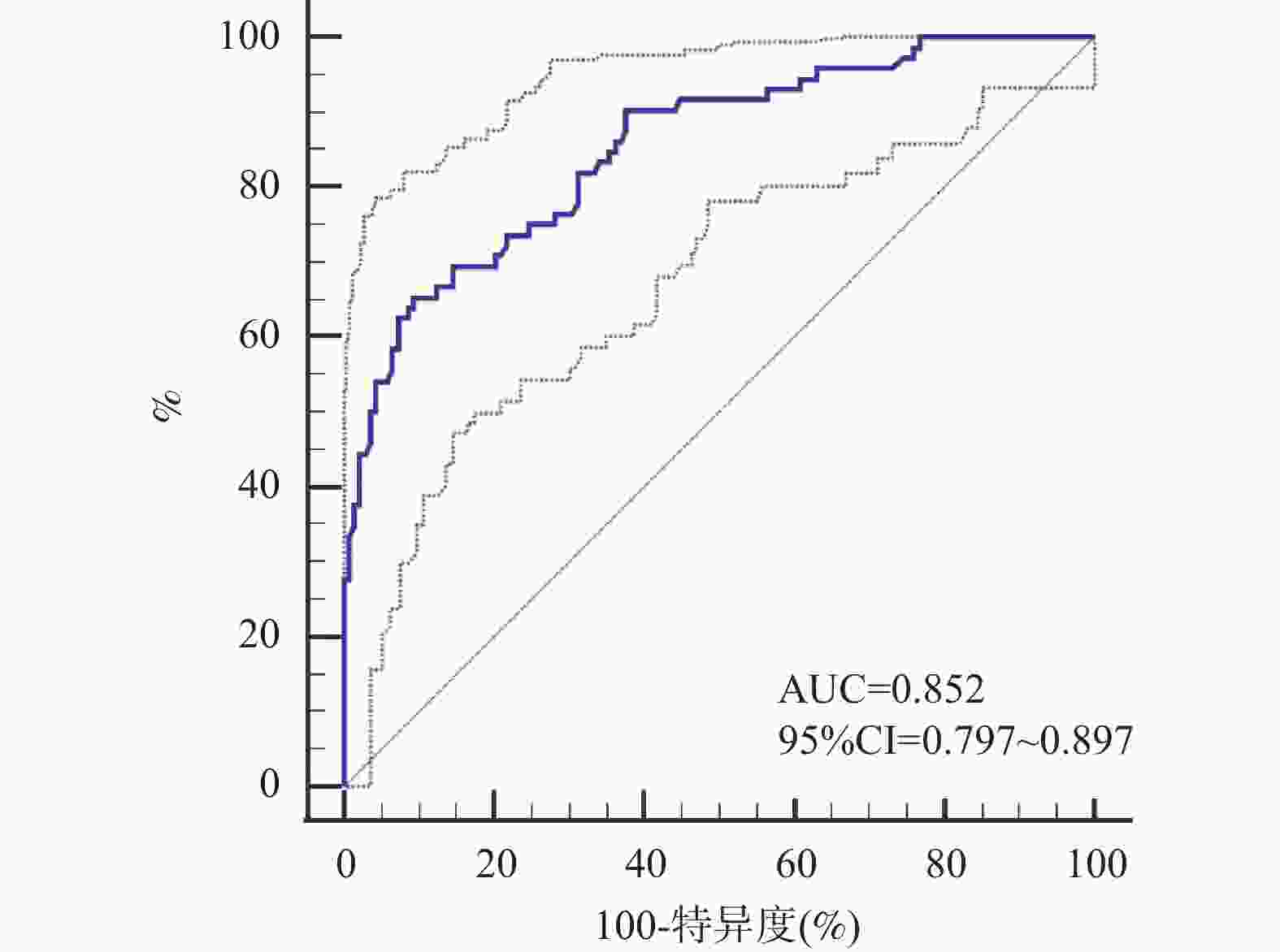
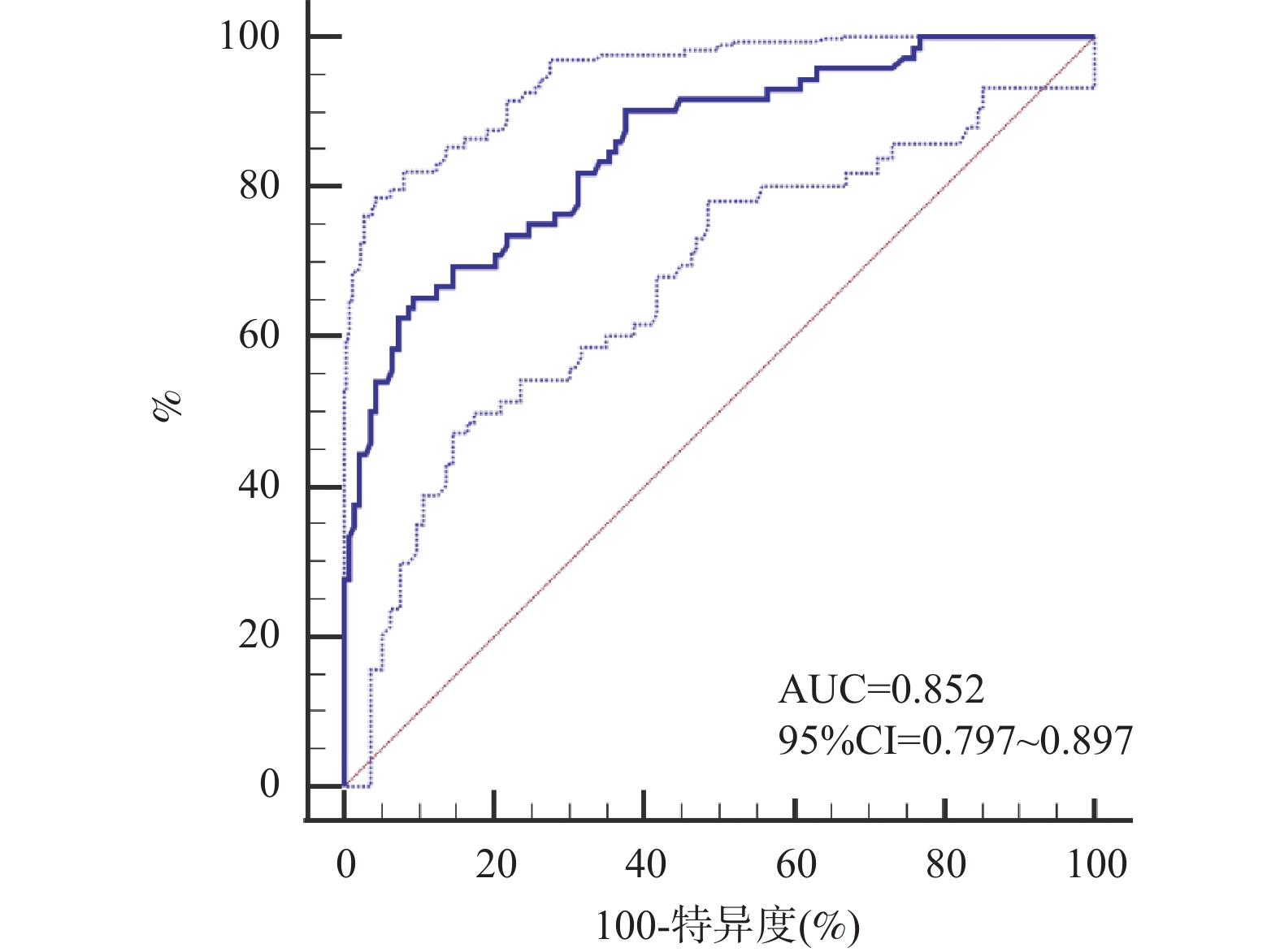
图 5 列线图模型预测AECOPD伴呼吸衰竭患者谵妄发生风险的ROC曲线图
Figure 5. ROC curve of the nomogram model for predicting the risk of delirium in patients with AECOPD and respiratory failure
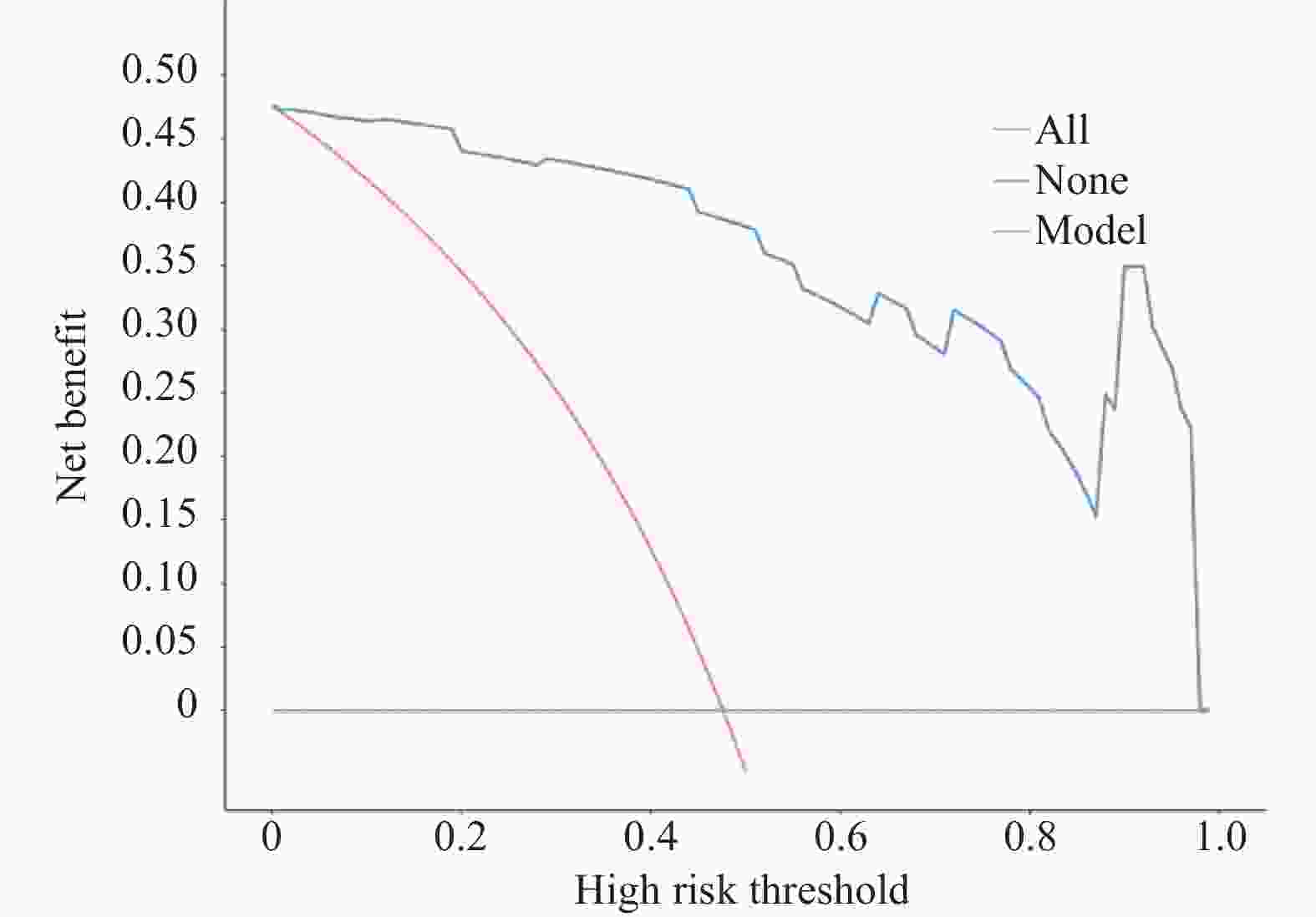
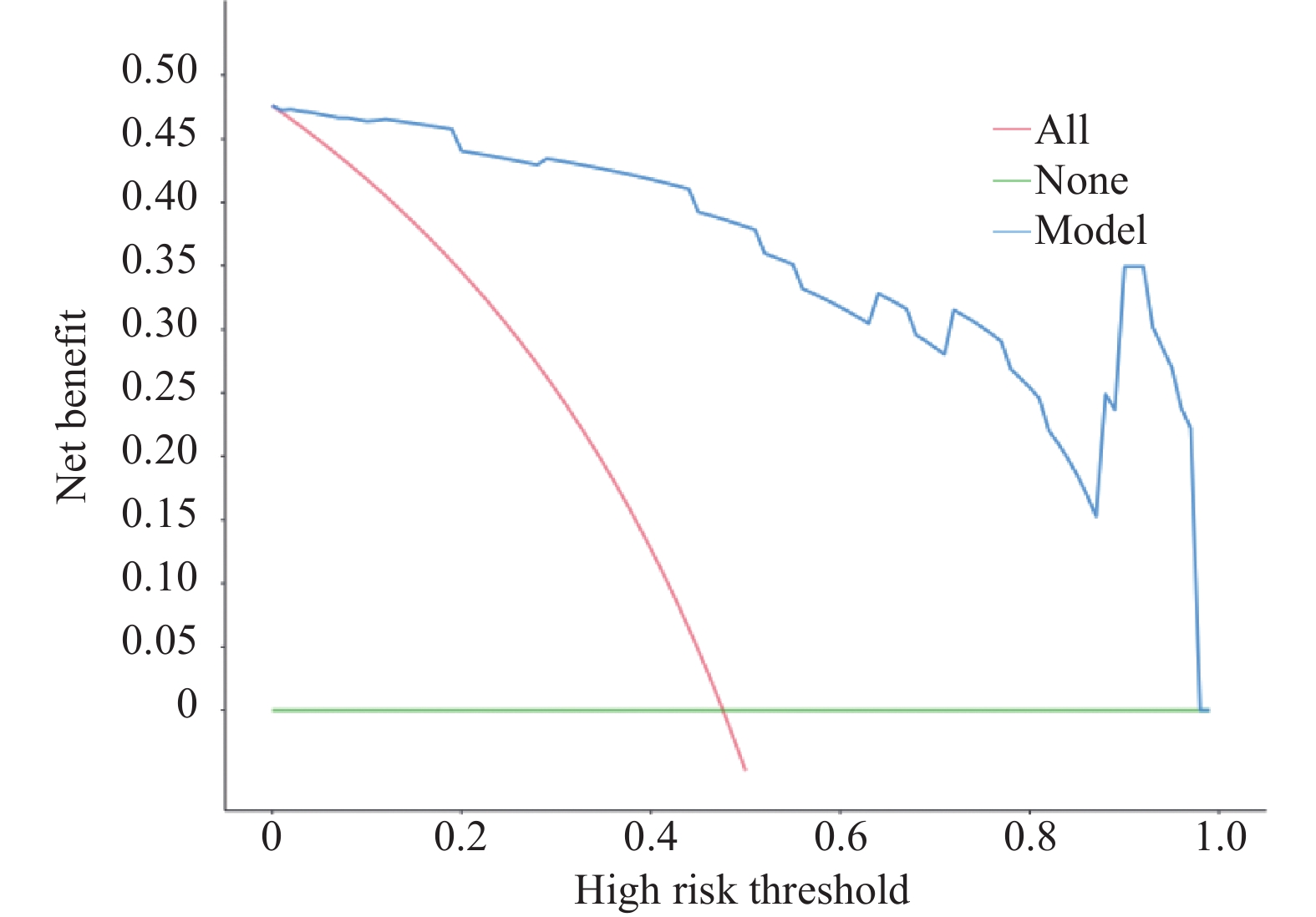
图 6 呼吸机使用时间、血清BDNF、ALB、CRP、miR-212-5p水平预测AECOPD伴呼吸衰竭患者谵妄发生风险临床实用性的DCA曲线图
Figure 6. DCA curve graph for predicting the risk of delirium in patients with AECOPD and respiratory failure based on the duration of ventilator use,serum BDNF,ALB,CRP,and miR-212-5p levels,which is clinically practical
表 1 两组一般基线资料及单因素分析[n(%)/($ \bar x \pm s $)]
Table 1. General baseline data of the two groups and univariate analysis[n(%)/($ \bar x \pm s $)]
资料 谵妄组(n = 72) 非谵妄组(n = 138) χ2/t P 性别 0.023 0.879 男 42(58.33) 82(59.42) 女 30(41.67) 56(40.58) 年龄(岁) 0.518 0.472 <60 53(73.61) 95(68.84) ≥60 19(26.39) 43(31.16) BMI(kg/m2) 20.14 ± 1.26 20.21 ± 1.32 0.370 0.711 COPD病程(年) 5.26 ± 1.03 5.21 ± 1.01 0.338 0.736 疾病史 有糖尿病 32(44.44) 45(32.61) 2.854 0.091 有高血压 35(48.61) 49(35.51) 3.385 0.066 吸烟史 3.316 0.069 有 46(63.89) 70(50.72) 无 26(36.11) 68(49.28) 饮酒史 2.959 0.085 有 48(66.67) 75(54.35) 无 24(33.33) 63(45.65) 机械通气方式 2.036 0.154 有创 50(69.44) 82(59.42) 无创 22(30.56) 56(40.58) 呼吸机使用时间(h) 72.36 ± 2.58 69.54 ± 2.14 8.435 <0.001* 住院天数(d) 13.05 ± 1.24 12.69 ± 1.34 1.895 0.059 APACHEII评分(分) 25.23 ± 2.14 24.85 ± 2.11 1.233 0.219 肺功能指标 FVC(L) 2.05 ± 0.11 2.03 ± 0.12 1.179 0.240 FEV1(L) 1.06 ± 0.12 1.08 ± 0.13 1.086 0.279 FEV1/FVC(%) 51.71 ± 3.12 52.20 ± 2.79 1.159 0.248 动脉血气分析相关指标 PaO2(mmHg) 51.02 ± 9.54 53.89 ± 9.62 2.058 0.041* PaCO2(mmHg) 61.89 ± 10.23 58.66 ± 10.25 2.169 0.031* 血清BDNF(μg/L) 0.52 ± 0.11 0.69 ± 0.13 9.466 <0.001* 血清ALB(g/L) 36.58 ± 2.14 39.12 ± 2.34 7.684 <0.001* CRP(mg/L) 82.36 ± 8.59 76.54 ± 3.25 7.061 <0.001* NEU(×109/L) 4.21 ± 1.03 4.06 ± 1.02 1.008 0.315 LYM(×109/L) 1.38 ± 0.12 1.42 ± 0.21 1.493 0.137 NLR 3.12 ± 0.72 2.95 ± 0.65 1.733 0.085 miR-212-5p 0.23 ± 0.04 0.31 ± 0.06 10.188 <0.001* *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 影响AECOPD伴呼吸衰竭患者发生谵妄的变量赋值
Table 2. Variable assignment for factors affecting delirium in AECOPD patients with respiratory failure
变量类型 名称 赋值 因变量 AECOPD伴呼吸衰竭发生谵妄 0=未发生;1=发生 自变量 呼吸机使用时间 0=≤72 h;1=>72 h PaO2 0=>60 mmHg;1=≤60 mmHg PaCO2 0=≤50 mmHg;1=>50 mmHg 血清BDNF水平 0=>0.64 μg/L;1=≤0.64 μg/L 血清ALB水平 0=>35 g/L;1=≤35 g/L 血清CRP水平 0=≤76.95 mg/L;1=>76.95 mg/L miR-212-5p水平 0=>0.27;1=≤0.27
下载: 导出CSV
表 3 AECOPD伴呼吸衰竭患者发生谵妄的多因素Logistic回归分析
Table 3. Multivariate Logistic regression analysis of delirium in AECOPD patients with respiratory failure
变量 β SE Wald χ2 P OR 95%CI 呼吸机使用时间 0.079 0.032 6.095 0.014* 1.082 1.016~1.152 PaO2 0.068 0.037 3.378 0.066 1.070 0.995~1.151 PaCO2 0.066 0.041 2.591 0.107 1.068 0.986~1.158 血清BDNF水平 −0.081 0.036 5.063 0.024* 0.922 0.859~0.99 血清ALB水平 −0.083 0.026 10.191 0.001* 0.920 0.875~0.968 血清CRP水平 0.078 0.028 7.760 0.005* 1.081 1.023~1.142 miR-212-5p水平 −0.076 0.033 5.304 0.021* 0.927 0.869~0.989 *P < 0.05。
下载: 导出CSV
表 4 呼吸机使用时间、血清BDNF、ALB、CRP、miR-212-5p水平预测AECOPD伴呼吸衰竭患者发生谵妄的ROC曲线分析
Table 4. ROC curve analysis for predicting delirium in patients with AECOPD and respiratory failure based on mechanical ventilating duration,serum BDNF,ALB,CRP,and miR-212-5p levels
指标 截断值 AUC 标准误 95%CI P 约登指数 灵敏度(%) 特异度(%) 呼吸机使用时间 72 h 0.807 0.0338 0.745~0.859 < 0.0001 *0.522 76.40 75.80 血清BDNF水平 0.64 μg/L 0.841 0.0288 0.783~0.889 < 0.0001 *0.554 81.94 73.44 血清ALB水平 35 g/L 0.793 0.0316 0.730~0.847 < 0.0001 *0.497 77.80 71.90 血清CRP水平 76.95 mg/L 0.745 0.0403 0.610~0.803 < 0.0001 *0.472 63.90 83.33 miR-212-5p水平 0.27 0.826 0.0281 0.768~0.875 < 0.0001 *0.526 90.28 62.32 *P < 0.05。
下载: 导出CSV
-
[1] 申普, 李乔玉, 张静, 等. 慢性阻塞性肺疾病急性加重期生物标志物研究进展[J]. 国际呼吸杂志, 2022, 42(24): 1874-1881. doi: 10.3969/j.issn.2096-2665.2025.13.007 [2] 李莉, 王蕾, 张丽, 等. 衰弱增加慢性阻塞性肺疾病急性加重期老年患者院内死亡风险: 一项真实世界研究[J]. 中国循证医学杂志, 2024, 24(6): 652-657. [3] 曾黎静, 张嘉瑞, 易群. 慢性阻塞性肺疾病急性加重期合并II型呼吸衰竭列线图模型的构建及验证[J]. 中国呼吸与危重监护杂志, 2024, 23(12): 876-881. [4] 王亮, 武柳君, 冯乐乐, 等. 慢性阻塞性肺疾病并发谵妄的研究进展[J]. 临床肺科杂志, 2024, 29(8): 1290-1293. doi: 10.3969/j.issn.1009-6663.2024.08.028 [5] 慢性阻塞性肺疾病急性加重诊治专家组. 慢性阻塞性肺疾病急性加重诊治中国专家共识(2023年修订版)[J]. 国际呼吸杂志, 2023, 43(2): 132-149. doi: 10.3760/cma.j.cn131368-20221123-01066 [6] 邹姮婧. 中文版CAM-ICU的信度效度检验及与其他量表的比较[D]. 武汉: 华中科技大学, 2012. [7] 贾睿奕, 张勃, 刘美新, 等. 慢性阻塞性肺疾病合并呼吸衰竭患者无创通气谵妄风险预测模型研究[J]. 心肺血管病杂志, 2025, 44(12): 1244-1252. [8] 苏妍, 高慧, 张艳, 等. 血清学指标联合急性生理学与慢性健康状况评分系统Ⅱ评分预测急性加重期慢性阻塞性肺疾病的预后[J]. 实用临床医药杂志, 2023, 27(17): 82-87. [9] 鲍传飞, 刘杰, 崔涛, 等. ICU住院期间酒精性肝硬化患者谵妄发生的危险因素: 倾向性匹配分析[J]. 肝胆外科杂志, 2025, 33(4): 283-288. [10] 李春萍, 曾艳, 蔡少青, 等. 急诊多发伤患者谵妄的影响因素及其风险预测列线图模型的构建[J]. 中国医药, 2022, 17(11): 1652-1656. [11] 王雷原, 胡小义, 王迪, 等. 老年患者术前脑损伤程度与术后谵妄的关系: 基于脑损伤标志物的潜在类别分析[J]. 中华麻醉学杂志, 2024, 44(3): 267-271. doi: 10.3760/cma.j.cn131073.20231031.00303 [12] 李静, 毕煜玲, 陈敏. 急性加重期COPD合并呼吸衰竭患者hs-CRP/Alb、CysC与预后的相关性分析[J]. 中国急救复苏与灾害医学杂志, 2020, 15(3): 311-314. doi: 10.3969/j.issn.1673-6966.2020.03.017 [13] 周大文, 杨晓梅, 赵文婷, 等. 慢性阻塞性肺疾病合并呼吸衰竭患者无创呼吸机治疗失败的影响因素及其风险预测列线图模型构建[J]. 实用心脑肺血管病杂志, 2023, 31(7): 11-16. doi: 10.12114/j.issn.1008-5971.2023.00.130 [14] 赵成刚, 王雅萍, 高洁, 等. CRP、PCT对重症监护室中慢性阻塞性肺疾病急性加重患者发生谵妄的预测价值[J]. 贵州医药, 2024, 48(5): 683-686. doi: 10.3969/j.issn.1000-744X.2024.05.003 [15] 周瑞玲, 张新宇, 张文江, 等. 基于“虚-毒-瘀”病机探讨慢性阻塞性肺疾病急性加重与炎症免疫相关miRNA的关系[J]. 辽宁中医药大学学报, 2023, 25(12): 208-212. [16] 刘继征, 曹佳璐, 赵敏, 等. 血清miR-212-5p、miR-221-3p与AECOPD患者TLR4/NF-κB炎症信号通路和预后的关系研究[J]. 检验医学与临床, 2024, 21(23): 3459-3465. [17] 安华, 王鑫, 张锡红, 等. 气道分级管理方案配合音乐刺激疗法对老年肺炎机械通气患者脱机时间及谵妄的影响[J]. 老年医学与保健, 2024, 30(3): 751-756. [18] 吴华炼, 辜甜田, 陈淼, 等. 早期离床活动对ICU机械通气患者谵妄的影响[J]. 中华危重病急救医学, 2021, 33(11): 1353-1357. doi: 10.3969/j.issn.2095-7629.2025.20.050 [19] 张伟丽, 娄景盛, 宋玉祥, 等. 生物标志物在老年患者术后谵妄诊疗中的应用综述[J]. 解放军医学院学报, 2023, 44(2): 197-200. doi: 10.3969/j.issn.2095-5227.2023.02.018 [20] 施咏梅, 陈尔真. 应重视老年重症患者的个体化营养治疗[J]. 老年医学与保健, 2024, 30(1): 6-9. [21] 王新, 张占华, 马丽, 等. C反应蛋白/白蛋白联合综合脱机指数对AECOPD并发呼吸衰竭有创机械通气患者撤机失败的预测价值[J]. 中国医药导报, 2024, 21(29): 106-110. doi: 10.20047/j.issn1673-7210.2024.29.21 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 208
- HTML全文浏览量: 203
- PDF下载量: 67
- 被引次数: 0
