

Effectiveness Comparison of Modular and Monoblock Femoral Prosthesis with Subtrochanteric Shortening Osteotomy in CroweType IV Developmental Dysplasia of the Hip
-
摘要:
目的 对比应用组配式S-ROM股骨假体与一体式Wagner Cone股骨假体联合转子下短缩截骨行全髋关节置换术(total hip arthroplasty,THA)治疗Crowe IV型发育性髋关节发育不良(developmental dysplasia of the hip,DDH)患者的临床疗效。 方法 回顾性分析2014年1月至2018年8月行THA治疗的58例(65髋)Crowe IV型DDH患者的临床资料,其中33例(37髋)使用组配式S-ROM假体,25例(28髋)使用一体式Wagner cone假体,记录两组患者的一般资料,手术时间,术中出血量,术后住院时间,截骨端愈合时间,手术前后Harris评分、VAS评分和相关并发症发生情况并进行分析。 结果 围手术期并发症发生率、术后住院时间、末次随访 Harris评分及VAS评分两组比较差异无统计学意义。组配式S-ROM假体组与一体式Wagner cone假体组,手术时间分别为(135.7±16.2)min和(113.3±13.0)min,术中出血量分别为(469.7±73.6)mL和(410.4±69.6)mL,组间比较差异有统计学意义(P < 0.05)。Wagner cone假体组愈合时间(5.8±1.5)月较组配式S-ROM假体组愈合时间(4.7±1.2)月延长,差异有统计学意义(P < 0.05)。 结论 应用组配式S-ROM假体与一体式Wagner cone假体联合股骨转子下短缩截骨行THA治疗Crowe Ⅳ型DDH均可获得良好的临床疗效。采用一体式Wagner Cone假体手术时间更短,术中出血量更少,采用组配式S-ROM假体截骨端愈合时间相对更短。 -
关键词:
- 发育性髋关节发育不良 /
- 全髋关节置换术 /
- 转子下截骨 /
- 组配式假体 /
- 一体式假体
Abstract:Objective To compare the clinical efficacy of modular S-ROM femoral prosthesis and monoblock Wagner Cone femoral prosthesis used in total hip arthroplasty for the treatment of Crowe type IV developmental dysplasia of the hip. Methods Retrospective study was conducted in 58 patients(65 hips) undergoing total hip arthroplasty for the treatment of Crowe type IV developmental dysplasia of the hip between January 2014 to August 2018, including 33 patients(37 hips) with modular S-ROM prosthesis and 25 patients(27 hips) with monoblock Wagner Cone prosthesis. The general data, operative time, intraoperative blood loss during the postoperative hospitalization, bone union time, Harris score, VAS score and perioperative complication rate were compared between the two groups. Results There was no significant difference in the perioperative complication rate during the postoperative hospitalization, Harris score and VAS score in the last follow-up between the two groups. The operative time was (135.7perat)min in the S-ROM group and (113.3n the)min in the Wagner Cone group, and there was a significant difference between the two groups (P < 0.05). The intraoperative blood loss was (469.7±43.6)ml in the S-ROM group and (410.4 rence between the two groups (and there was a significant difference between the two groups (P < 0.05). The bone healing time of Wagner Cone group was significantly longer than that of S-ROM group (P < 0.05). Conclusion The application of both the modular S-ROM andmonoblock Wagner Cone femoral prosthesis with subtrochanteric shortening osteotomy in total hip arthroplasty for the treatment of Crowe type IV developmental dysplasia of the hip has a good clinical efficacy. The monoblock Wagner Cone prosthesis has the shorter operative time and less intraoperative blood loss, and the modular S-ROM prosthesis has shorter bone healing time. -
全髋关节置换术(total hip arthroplasty,THA)是治疗DDH继发严重髋关节骨关节炎的有效术式[1],其中Crowe Ⅳ型DDH由于髋关节周围骨性结构及髋周软组织结构处于异常的病理状态,极大增加了手术难度及风险[2]。Crowe IV型DDH存在股骨头高脱位,恢复解剖中心需要相对延长肢体,多数学者认为当下肢延长超过4 cm时,行股骨转子下短缩截骨可利于平衡下肢长度,降低复位难度和神经损伤并发症发生率[3-4]。另外,Crowe IV型DDH通常存在股骨近端髓腔过度狭窄、前倾角过大等特点[5],采用常规初次置换假体可能面临术中假体安放困难,术后假体撞击及假体脱位等问题[6]。所以需要借助适用于DDH的股骨假体,组配式S-ROM股骨假体及一体式Wagner Cone股骨假体可适应畸形细小的髓腔,自由调节假体前倾角,降低Crowe IV型DDH的手术难度[4,7-8]。两类假体均已被证实可在Crowe IV型DDH患者中取得良好的临床疗效,但目前对于术中假体的选择,仍存在一定争议。本研究将回顾性分析2014年1月至2018年8月行THA治疗Crowe IV型DDH患者的临床资料,对比分析组配式S-ROM股骨假体及一体式Wagner Cone股骨假体联合转子下短缩截骨行THA治疗Crowe Ⅳ型 DDH疗效,借此为今后Crowe Ⅳ型 DDH 的治疗提供借鉴。
1. 临床资料
1.1 一般资料
纳入标准:(1)据Crowe分型标准[9]确诊为Ⅳ型的DDH患者;(2)具备手术指征,即合并髋关节严重疼痛和功能障碍。排除标准:(1)合并髋关节活动性感染;(2)伴随其他急性或重大疾病不能耐受手术。根据上述标准,本研究共纳入2014年1月至2018年8月昆明医科大学第一附属医院骨科收治的58例(65髋)Crowe Ⅳ型DDH患者。组配式S-ROM假体组33例(37髋),男4例(5髋),女29例(32髋),年龄23~73(41.6±12.7)岁,BMI(22.0±0.2)kg/m2。一体式Wagner cone假体组25例(28髋),男2例(2髋),女23例(26髋),年龄24~60(38.5±10.6)岁,BMI(21.5±0.2)kg/m2。两组患者的一般资料经比较,差异均无统计学意义,见表1。
表 1 两组患者的一般资料比较($\bar x \pm s $ )Table 1. Comparison of general data between 2 groups($\bar x \pm s $ )指标 组配式S-ROM假体组(n = 33) 一体式Wagner Cone假体组(n = 25) t/χ2 P 年龄(岁) 41.6 ± 12.7 38.5 ± 10.6 t = 1.017 0.313 性别(女∶男,n) 29∶4 23∶2 χ2 = 0.260 0.610 BMI(kg/m2) 22.0 ± 0.2 21.5 ± 0.2 t = 1.603 0.115 1.2 手术方法
所有手术均由昆明医科大学第一附属医院骨科关节组同一名经验丰富的医师主刀完成。患者均于全麻后取侧卧位,采用后外侧入路。切除增生肥厚的关节囊,屈曲、内收、内旋髋关节,于基底部截断股骨颈,清理增生的纤维组织及骨赘,以圆韧带和横韧带为解剖标志寻找真臼。取髋臼锉自小到大打磨加深、扩大髋臼,直至显露松质骨及点状出血。压配植入合适型号的髋臼假体,使用螺钉增加臼杯稳定性。股骨开髓后,两组患者分别采用组配式S-ROM假体及一体式Wagner Cone假体专用磨锉工具进行扩髓,分别打入各自假体试模,牵引远端肢体,试行复位,于小转子下方1~2 cm标记截骨部位,横行截骨截除与股骨近端重叠的远侧股骨段。为预防股骨劈裂,可在截骨端预扎钢丝。复位并固定截骨两端,进一步磨锉扩髓,分别安装合适的股骨假体及股骨头。复位后检查髋关节稳定性、活动度及下肢长度,留置引流,逐层缝合切口。
1.3 术后处理
两组患者术后患肢均保持屈髋、屈膝、外展中立位,麻醉苏醒后鼓励患者行股四头肌等长收缩及踝泵锻炼,常规预防性使用抗生素,口服利伐沙班预防深静脉血栓。2 d后逐渐减少屈髋、屈膝角度,开始拄双拐下地部分负重活动。6~8周时摄X线片视截骨端愈合情况渐进负重。术后3月、半年、1 a定期随访复查。
1.4 统计学处理
采用SPSS 22.0统计软件进行数据分析。计量资料采用(
$\bar x \pm s$ )表示,组内数据比较采用配对样本t检验,组间数据比较采用独立样本t检验,非计量资料以n(%)表示,采用χ2检验。P < 0.05为差异有统计学意义。2. 结果
组配式S-ROM假体组随访时间24~44(29.2±5.2)月,末次随访时髋关节Harris评分由术前(38.6±3.4)提高至术后(88.5±2.3),差异有统计学意义(t = −109.663,P < 0.001),VAS评分由术前(7.1±0.7)改善至术后(2.7±0.5),差异有统计学意义(t = 33.769,P < 0.001)。一体式Wagner cone假体组随访时间24~38(29.0±4.5)月,末次随访时髋关节Harris评分由术前(39.7±4.2)提高至术后(88.5±2.3),差异有统计学意义(t = −67.367,P < 0.001),VAS评分由术前(7.0±0.1)改善至术后(2.6±0.1),差异有统计学意义(t = 28.902,P < 0.001)。组间比较,两组患者末次随访时Harris评分比较没有差异(t = −1.097,P = 0.277),末次随访时VAS评分比较没有差异(t = 0.760,P = 0.450),见表2、表3。组配式S-ROM假体组与一体式Wagner cone假体组,手术时间分别为105~160 min,(135.7±16.2)min和90~140 min,(113.3±13.0)min组间比较差异有统计学意义(t = 5.659,P < 0.001),术中出血量分别为300~650 mL,(469.7±73.6)mL和280~550 mL,(410.4±69.6)mL,组间比较差异有统计学意义(t = 3.109,P = 0.003)。两组患者经临床评估,术前髋关节疼痛及功能受限均明显改善或消失。
表 2 两组术前和末次随访时Harris评分比较($\bar x \pm s$ )Table 2. Comparison of preoperative and last follow-up Harris scores between the two groups($\bar x \pm s$ )时间 组配式S-ROM
假体组
(n = 33)一体式Wagner
Cone假体组
(n = 25)t P 术前 38.6 ± 3.4 39.7 ± 4.2 −1.116 0.269 末次随访 88.5 ± 2.3 88.5 ± 2.3 −1.097 0.277 t −109.663 −67.367 P < 0.001 < 0.001 表 3 两组术前和末次随访时VAS评分比较($\bar x \pm s$ )Table 3. Comparison of preoperative and last follow-up VAS scores between the two groups($\bar x \pm s$ )时间 组配式S-ROM
假体组
(n = 33)一体式Wagner
Cone假体组
(n = 25)t P 术前 7.1 ± 0.7 7.0 ± 0.1 −0.197 0.277 末次随访 2.7 ± 0.5 2.6 ± 0.1 0.760 0.450 t 33.769 28.902 P < 0.001 < 0.001 术后并发症:组配式S-ROM假体组1例术后5 d发生下肢胫后静脉血栓形成,经保守治疗后消退。1例遗留轻度跛行,但较术前显著改善。一体式Wagner cone假体组1例出现股神经麻痹症状,予以营养神经对症治疗后恢复。两组患者截骨端均骨性愈合,Wagner cone假体组愈合时间较组配式S-ROM假体组延长,差异有统计学意义。切口均I期愈合,随访期内均未发生髋关节脱位、假体周围骨折、感染、松动等并发症。两组患者并发症发生率无统计学意义,见表4。典型病例见图1、图2。
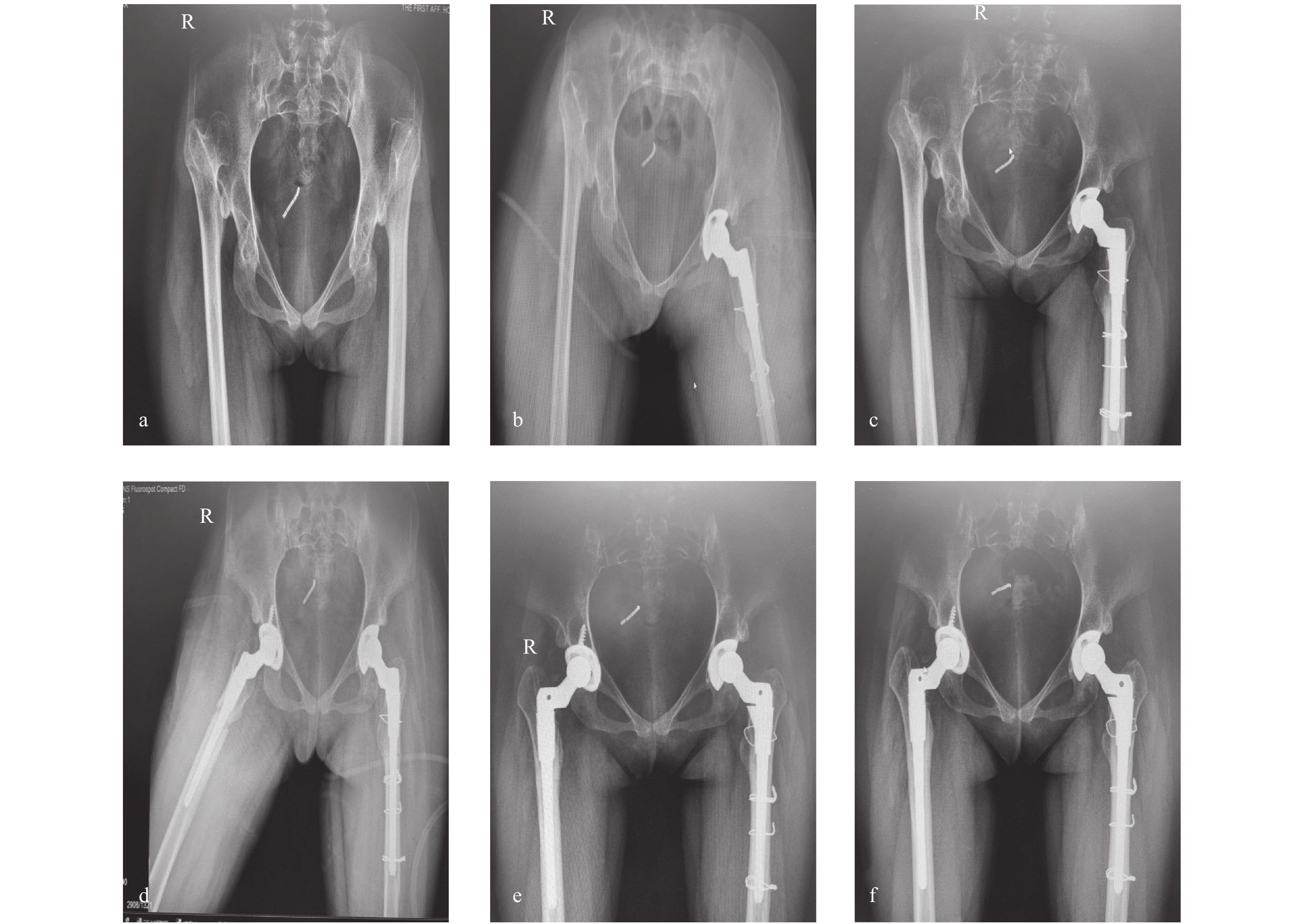 图 1 患者,女,27岁,双侧Crowe Ⅳ型DDH,应用组配式S-ROM假体联合股骨转子下截骨行THAa:术前;b:左侧术后当天;c:左侧术后3月;d:左侧术后6月,右侧术后当天;e:左侧术后12月,右侧术后6月;f:左侧术后30月,右侧术后24月。Figure 1. A 27-year-old women with bilateral Crowe type IV hip dysplasia,THA with modular S-ROM prosthesis and subtrochanteric shortening osteotomy
图 1 患者,女,27岁,双侧Crowe Ⅳ型DDH,应用组配式S-ROM假体联合股骨转子下截骨行THAa:术前;b:左侧术后当天;c:左侧术后3月;d:左侧术后6月,右侧术后当天;e:左侧术后12月,右侧术后6月;f:左侧术后30月,右侧术后24月。Figure 1. A 27-year-old women with bilateral Crowe type IV hip dysplasia,THA with modular S-ROM prosthesis and subtrochanteric shortening osteotomy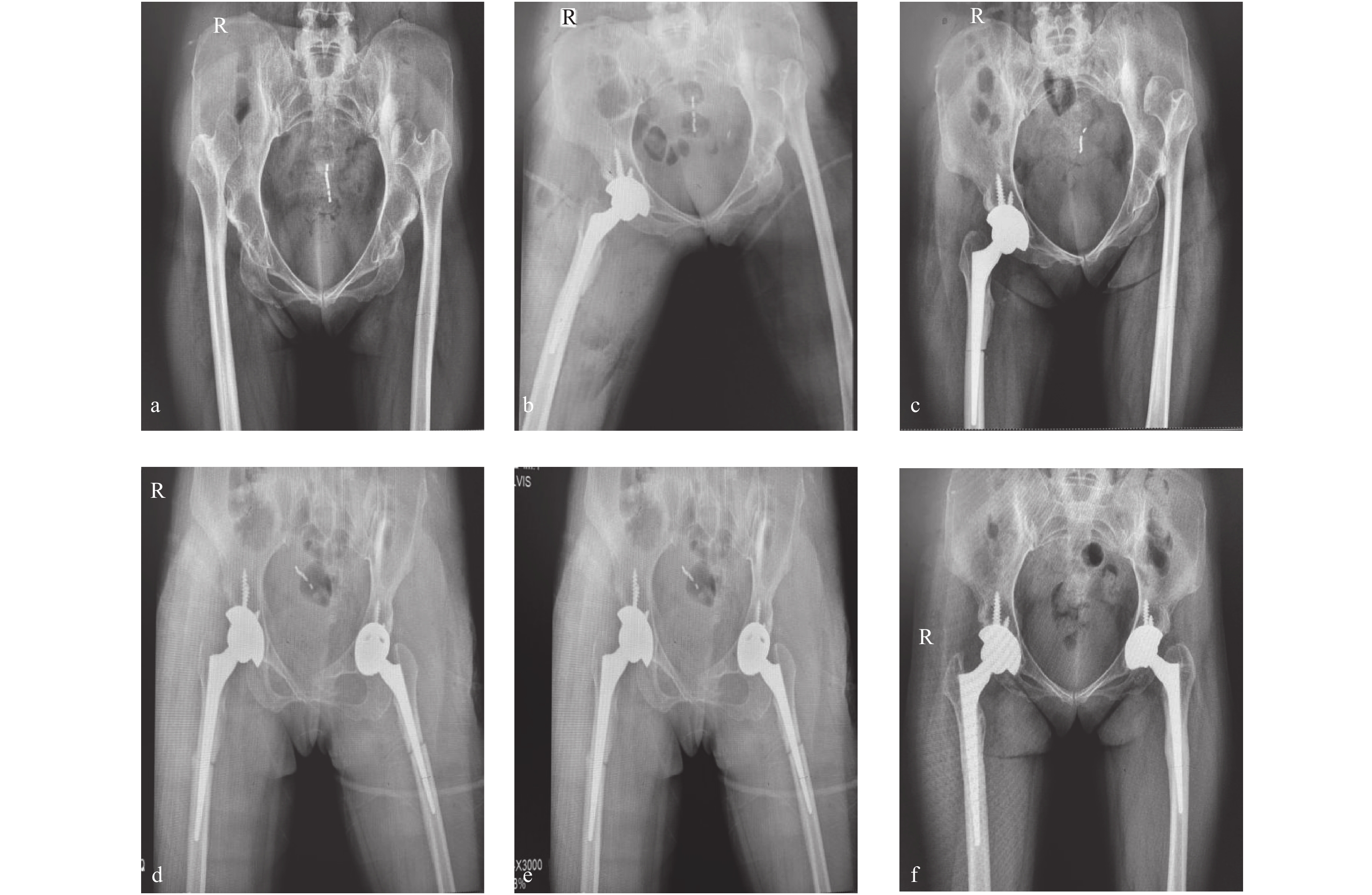 图 2 患者,女,50岁,双侧Crowe Ⅳ型DDH,一体式Wagner cone假体联合股骨转子下截骨行THAa:术前;b:右侧术后当天;c:右侧术后3月;d:右侧术后4月,左侧术后当天;e:右侧术后7月,左侧术后3月;f:右侧术后24月,左侧术后21月。Figure 2. A 50-year-old women with bilateral Crowe type IV hip dysplasia,THA with monoblock Wagner Cone prosthesis and subtrochanteric shortening osteotomy表 4 两组患者临床疗效比较(
图 2 患者,女,50岁,双侧Crowe Ⅳ型DDH,一体式Wagner cone假体联合股骨转子下截骨行THAa:术前;b:右侧术后当天;c:右侧术后3月;d:右侧术后4月,左侧术后当天;e:右侧术后7月,左侧术后3月;f:右侧术后24月,左侧术后21月。Figure 2. A 50-year-old women with bilateral Crowe type IV hip dysplasia,THA with monoblock Wagner Cone prosthesis and subtrochanteric shortening osteotomy表 4 两组患者临床疗效比较($\bar x \pm s$ )Table 4. Comparison of clinical outcomes between 2 groups($\bar x \pm s$ )指标 组配式S-ROM假体组(n = 33) 一体式Wagner Cone假体组(n = 25) t/χ2 P 手术时间(min) 135.7 ± 16.2 113.3 ± 13.0 t = 5.659 < 0.001 术中出血量(mL) 469.7 ± 73.6 410.4 ± 69.6 t = 3.109 0.003* 术后住院时间(d) 7.3 ± 1.5 7.1 ± 1.6 t = 0.520 0.605 围手术期并发症发生率[n(%)] 6.1%(2/33) 4.0%(1/25) χ2 = 0.123 0.726 截骨端愈合时间(月) 4.7 ± 1.2 5.8 ± 1.5 t = −3.242 0.002* *P < 0.05。 3. 讨论
在Crowe IV型DDH中,由于股骨头前倾角及外展角增大,股骨近端前弓弧度增大,髓腔细小,髓腔横径与矢状径比例异常增大,导致常规矩形股骨假体难以适用,故临床上常用前倾角可调,且能适应畸形细小髓腔的S-ROM股骨假体或Wagner Cone股骨假体[4-5,7]。虽然两类假体均已被证实可在Crowe IV型DDH患者THA术中取得较好的临床效果,但目前尚缺乏关于两类假体特点及疗效的比较研究。
S-ROM假体为组配式圆柱形柄,主要特点为:(1)双锥度连接设计,可调节股骨前倾角和下肢长度,还可通过选择合适形状及长度的假体颈恢复髋周软组织张力,重建髋关节生物力学结构;(2)近端固定依靠袖套表面微孔涂层提供骨长入,远端依靠髓内充填压配固定;(3)锥形袖套可在假体与股骨近端间提供椭圆形交锁,同时袖套表面沟槽可阶梯状传导压力负荷,保证了假体可以抵抗旋转应力和垂直应力;(4)假体直径范围6.0~21.0 mm,柄长范围115.0~175.0 mm可适应髓腔狭小畸形;(5)远端8条纵行脊状突起较股骨柄直径大1.25 mm,可插入松质骨中,提高假体抗旋转稳定性;(6)远端冠状槽设计可减小柄远端硬度,减少应力遮挡。Wagner cone假体一体式圆锥形短柄,主要特点为:(1)圆形横断面利于假体植入自由旋转,调整前倾角;(2)柄体带有8条纵行凸纹设计,可锚入股骨中远端皮质,增加骨接触面积和附着,并提供抗旋转稳定性;(3)颈干角有125°和135°两种设计,增加了术中可选择性;(4)假体直径范围6.4~10.4 mm,柄长范围115.0~127.2 mm,可适应短且狭小的近端髓腔。
本研究就术中出血量、手术时间进行比较,组配式S-ROM假体组均显著多于一体式Wagner Cone假体组,其原因可能在于S-ROM假体需要分别进行远端扩髓和近端磨锉,操作步骤相对复杂。但是两组间术后住院时间、并发症发生率、末次随访时Harris评分、VAS评分无统计学差异。这表明两类假体均可安全、有效地运用于Crowe IV型DDH患者。
Crowe Ⅳ型DDH存在股骨头高脱位,恢复解剖中心需要相对延长肢体,由此将增加神经、血管损伤风险[10]。对下肢短缩不是特别严重的患者不主张截骨,尽可能通过使用骨骼肌松弛药物,结合松解髋关节周围软组织达到复位的目的。目前临床研究表明,下肢延长超过4 cm时坐骨神经牵拉损伤的风险会明显增加[11]。因此对下肢短缩超过 4 cm 经牵引和松解仍无法复位的患者可考虑股骨转子下截骨。转子下短缩截骨用于治疗Crowe IV型DDH患者的有效性已经得到证实,但相关并发症比如术中股骨劈裂骨折、术后截骨端不愈合等,严重影响手术疗效及患者术后康复[12]。在Crowe IV型DDH患者THA术中,股骨骨折发生率为0%~27.8%[4、7、12]。在本次研究中,S-ROM假体组中无股骨劈裂骨折发生,Wagner Cone假体组中发生1例,其发生率无统计学差异。据近来文献报道,S-ROM假体术中骨折发生率为0%~5.3%[7,13],Wagner Cone假体术中骨折发生率为0%~3.92%[4,14-15]。Mu[16]等使用矩形的Zweymuller股骨假体对50例(71髋)Crowe IV型DDH患者行THA治疗,术中骨折发生率为27.8%。故在Crowe IV型DDH术中,采用S-ROM假体或Wagner Cone假体均可获得较低的股骨骨折发生率。另外,截骨端不愈合也是THA联合转子下短缩截骨治疗Crowe IV型DDH的一个常见并发症。据既往文献,Crowe IV型DDH患者截骨端不愈合率为0%~7.1%[17-18],主要影响因素之一是截骨端的稳定性。Muratli[19]等进行了一项生物力学研究,证明了横行截骨、楔形截骨、“Z”型截骨、双“V”型截骨之间稳定性无统计学差异。由于横行截骨操作相对简便,对截骨部位骨膜损伤较小,故本次研究中两组患者均采用转子下横行短缩截骨。此外,假体类型可能也是影响截骨端稳定性的重要因素[19]。在本组研究中,S-ROM假体组与Wagner Cone假体组中均未发生截骨不愈合,但S-ROM假体组截骨端愈合时间短于Wagner Cone假体组,差异有统计学意义。Onodera认为S-ROM假体可通过股骨近端袖套和远端脊状突起的充分压配来获得良好的旋转对线和初始稳定性[20]。Huang等认为截骨位置适当向远端移动可增加截骨端旋转稳定性[21]。Ozan认为假体柄应越过截骨端4 cm~5 cm,以增加截骨端稳定性[22]。S-ROM假体的最大长度(175.0 mm)大于Wagner Cone假体的最大长度(127.2 mm),且长柄可分担应力,减轻应力遮挡。因此,S-ROM假体被更广泛地应用于Crowe型IV型DDH。但是S-ROM假体也存在各组配部件之间磨损、腐蚀及断裂的可能性,且价格昂贵[23]。所以,有学者提出使用Wagner Cone假体在Crowe IV型DDH患者中也可取得良好的临床效果。Grappiolo等[4]对74例Crowe IV型DDH患者(102髋)采用Wagner Cone假体联合股骨转子下短缩截骨,平均随访11.3 a,截骨端不愈合率为3.9%,取得了良好的长期存活率、临床和影像学结果。
综上所述,应用组配式S-ROM假体与一体式Wagner cone假体联合股骨转子下短缩截骨行THA治疗Crowe Ⅳ型DDH均可获得良好的临床疗效。采用一体式Wagner Cone假体手术时间更短,术中出血量更少,采用组配式S-ROM假体截骨端愈合时间相对更短。但是具体两类假体的旋转稳定性差异还需进一步的生物力学研究,远期临床疗效还需继续随访观察。
-
图 1 患者,女,27岁,双侧Crowe Ⅳ型DDH,应用组配式S-ROM假体联合股骨转子下截骨行THA
a:术前;b:左侧术后当天;c:左侧术后3月;d:左侧术后6月,右侧术后当天;e:左侧术后12月,右侧术后6月;f:左侧术后30月,右侧术后24月。
Figure 1. A 27-year-old women with bilateral Crowe type IV hip dysplasia,THA with modular S-ROM prosthesis and subtrochanteric shortening osteotomy
图 2 患者,女,50岁,双侧Crowe Ⅳ型DDH,一体式Wagner cone假体联合股骨转子下截骨行THA
a:术前;b:右侧术后当天;c:右侧术后3月;d:右侧术后4月,左侧术后当天;e:右侧术后7月,左侧术后3月;f:右侧术后24月,左侧术后21月。
Figure 2. A 50-year-old women with bilateral Crowe type IV hip dysplasia,THA with monoblock Wagner Cone prosthesis and subtrochanteric shortening osteotomy
表 1 两组患者的一般资料比较(
$\bar x \pm s $ )Table 1. Comparison of general data between 2 groups(
$\bar x \pm s $ )指标 组配式S-ROM假体组(n = 33) 一体式Wagner Cone假体组(n = 25) t/χ2 P 年龄(岁) 41.6 ± 12.7 38.5 ± 10.6 t = 1.017 0.313 性别(女∶男,n) 29∶4 23∶2 χ2 = 0.260 0.610 BMI(kg/m2) 22.0 ± 0.2 21.5 ± 0.2 t = 1.603 0.115  下载: 导出CSV
下载: 导出CSV
表 2 两组术前和末次随访时Harris评分比较(
$\bar x \pm s$ )Table 2. Comparison of preoperative and last follow-up Harris scores between the two groups(
$\bar x \pm s$ )时间 组配式S-ROM
假体组
(n = 33)一体式Wagner
Cone假体组
(n = 25)t P 术前 38.6 ± 3.4 39.7 ± 4.2 −1.116 0.269 末次随访 88.5 ± 2.3 88.5 ± 2.3 −1.097 0.277 t −109.663 −67.367 P < 0.001 < 0.001
下载: 导出CSV
表 3 两组术前和末次随访时VAS评分比较(
$\bar x \pm s$ )Table 3. Comparison of preoperative and last follow-up VAS scores between the two groups(
$\bar x \pm s$ )时间 组配式S-ROM
假体组
(n = 33)一体式Wagner
Cone假体组
(n = 25)t P 术前 7.1 ± 0.7 7.0 ± 0.1 −0.197 0.277 末次随访 2.7 ± 0.5 2.6 ± 0.1 0.760 0.450 t 33.769 28.902 P < 0.001 < 0.001
下载: 导出CSV
表 4 两组患者临床疗效比较(
$\bar x \pm s$ )Table 4. Comparison of clinical outcomes between 2 groups(
$\bar x \pm s$ )指标 组配式S-ROM假体组(n = 33) 一体式Wagner Cone假体组(n = 25) t/χ2 P 手术时间(min) 135.7 ± 16.2 113.3 ± 13.0 t = 5.659 < 0.001 术中出血量(mL) 469.7 ± 73.6 410.4 ± 69.6 t = 3.109 0.003* 术后住院时间(d) 7.3 ± 1.5 7.1 ± 1.6 t = 0.520 0.605 围手术期并发症发生率[n(%)] 6.1%(2/33) 4.0%(1/25) χ2 = 0.123 0.726 截骨端愈合时间(月) 4.7 ± 1.2 5.8 ± 1.5 t = −3.242 0.002* *P < 0.05。
下载: 导出CSV
-
[1] Hartofilakidis G,Georgiades G,Babis G C,et al. Evaluation of two surgical techniques for acetabular reconstruction in total hip replacement for congenital hip disease:results after a minimumten years follow-up[J]. J Bone Joint surg Br,2008,90(6):724-730. [2] Greber E M,Pelt C E,Gililland J M,et al. Challenges in total hip arthroplasty in the setting of developmental dysplasia of the hip[J]. J Arthroplast,2017,32(9):38-44. doi: 10.1016/j.arth.2017.02.024 [3] Li H,Yuan Y,Xu J,et al. Direct leverage for reducing the femoral head in total hip arthroplasty without femoral shortening osteotomy for Crowe type 3 to 4 dysplasia of the hip[J]. J Arthroplasty,2018,33(3):794-799. doi: 10.1016/j.arth.2017.09.011 [4] Grappiolo G,La Camera F,Della Rocca A,et al. Total hip arthroplasty with a monoblock conical stem and subtrochanteric transverse shortening osteotomy in Crowe type IV dysplastic hips[J]. Int Orthop,2019,43(1):77-83. doi: 10.1007/s00264-018-4122-5 [5] Liu S,Zuo J,Li Z,et al. Study of three-dimensional morphology of the proximal femur in developmental adult dysplasia of the hip suggests that the on-shelf modular prosthesis may not be an ideal choice for patients with Crowe type IV hips[J]. Int Orthop,2017,41(4):707-713. doi: 10.1007/s00264-016-3248-6 [6] Ozden V E,Dikmen G,Beksac B,et al. Tapered stems one-third proximally coated have higher complication rates than cylindrical two-third coated stems in patients with high hip dislocation undergoing total hip arthroplasty with step-cut shortening osteotomy[J]. Orthop Traumatol Surg Res,2017,103(4):569-577. doi: 10.1016/j.otsr.2017.01.010 [7] Wang D,Li L L,Wang H Y,et al. Long-term results of cementles total hip arthroplasty with subtrochanteric shortening osteotomy in Crowe type IV developmental dysplasia[J]. J Arthroplasty,2017,32(4):1211-1219. doi: 10.1016/j.arth.2016.11.005 [8] 杨佳,杨毅,赵云宏,等. 应用3D打印技术联合组配式S-ROM假体人工髋关节置换术治疗成人Crowe Ⅳ DDH[J].昆明医科大学学报,2018,39(5):83-89. doi: 10.3969/j.issn.1003-4706.2018.05.017 [9] Crowe J F,Mani V J,Ranawat C S. Total hip replacement in congenital dislocation and dysplasia of the hip[J]. J Bone Joint Surg Am,1979,61(1):15-23. [10] Sonohata M,Kitajima M,Kawano S,et al. Nerve palsy after total hip arthroplasty without subtrochanteric femoral shortening osteotomy for a completely dislocated hip joint[J]. Open Orthop,2016,10:788-792. [11] Edwards B N,Tullos H S,Nobel P C. Contributory factors and etio-logy of sciatic nerve palsy in total hip arthroplasia[J]. Clin Orthop,1987(218):136-141. [12] Gong S,Xu W,Wang R,et al. The causes and management of nonunion of femoral subtrochanteric shortening osteotomy in a THA patient:a case report[J]. BMC Musculoskelet Disord,2019,20(1):203. doi: 10.1186/s12891-019-2612-2 [13] Shi X T,Cheng C M,Feng C Y,et al. Crowe type IV hip dysplasia treated by THA comebined with osteotomy to balance functional leg length discrepancy:A prospective observational study[J]. Orthop Surg,2020,12(2):533-542. doi: 10.1111/os.12655 [14] 卢玮,曾敏,雷鹏飞,等. Wagner Cone生物型股骨假体置换联合转子下短缩截骨术治疗成人Crowe Ⅳ型髋关节发育不良[J].中国修复重建外科杂志,2019,33(8):929-934. [15] 彭永刚,张坤,苗润清,等. Wagner cone股骨柄联合转子下横形截骨的全髋关节置换术治疗Crowe Ⅳ型髋关节发育不良[J].实用骨科杂志,2018,24(12):1077-1081. [16] Mu W,Yang D,Xu B,et al. Midterm outcome of cementless total hip arthroplasty in crowe IV-hartofilakidis type III developmental dysplasia of the hip[J]. J Arthroplasty,2016,31(3):668-675. doi: 10.1016/j.arth.2015.10.011 [17] Zhu J,Shen C,Chen X,et al. Total hip arthroplasty with a non-modular conical stem and transverse subtrochanteric osteotomy in treatment of high dislocated hips[J]. J Arthroplasty,2015,30(4):611-614. doi: 10.1016/j.arth.2014.11.002 [18] Ollivier M,Abdel M P,Krych A J,et al. Long-term results of total hip arthroplasty with shortening subtrochanteric osteotomy in crowe IV developmental dysplasia[J]. J Arthroplasty,2016,31(8):1756-1760. doi: 10.1016/j.arth.2016.01.049 [19] Muratli K S,Karatosun V,Uzun B,et al. Subtrochanteric shortening in total hip arthroplasty:biomechanical comparison of four techniques[J]. J Arthroplasty,2014,29(4):836-842. doi: 10.1016/j.arth.2013.09.004 [20] Onodera S,Majima T,Ito H,et al. Cementless total hip arthroplasty using the modular S-ROM prosthesis combined with corrective proximal femoral osteotomy[J]. J Arthroplasty,2006,21(5):664-669. doi: 10.1016/j.arth.2005.08.016 [21] Huang Z Y,Liu H,Li M,et al. Optimal location of subtrochanteric osteotomy in total hip arthroplasty for crowe type IV developmental dysplasia of hip[J]. BMC Musculoskelet Disord,2020,21(1):210. doi: 10.1186/s12891-020-03248-8 [22] Ozan F,Uzun E,Gürbüz K,et al. Total hip arthroplasty in the developmental dysplasia of the hip using transverse subtrochanteric osteotomy[J]. J Orthop,2016,13(4):259-263. doi: 10.1016/j.jor.2016.06.010 [23] 赵众首,孙俊英. 组配式S-ROM假体在髋关节发育不良及髋关节翻修术中的应用进展[J].中国修复重建外科杂志,2012,26(9):1054-1057. -



 下载:
下载:







 点击查看大图
点击查看大图
计量
- 文章访问数: 3406
- HTML全文浏览量: 1998
- PDF下载量: 15
- 被引次数: 0
