

Polyethylene Glycol 4000 Lowers Serum Uric Acid in Uricase-deficient Rats
-
摘要:
目的 观察聚乙二醇4000(PEG4000)对雄性Kunming-DY大鼠(尿酸酶缺失大鼠)的降尿酸作用。 方法 选取45d雄性Kunming-DY大鼠共24只,设对照组(n = 6)和治疗组:PEG4000高(10.5 g/L)、中(5.25 g/L)、低(2.625 g/L)剂量组各6只。对照组自由饮水,治疗组自由饮用1周。实验前后需剪尾取血,收集血清以及大鼠24 h尿液和粪便,记录24 h进食和饮水量同时收集大鼠主要组织器官。测定血清样品中的尿酸、血尿素氮和血肌酐的含量和排泄物尿酸含量以及组织器官样品尿酸含量,观察对照组和治疗组各个指标的变化。 结果 (1)对照组血尿酸高于70 µg/mL,而PEG4000(10.5、5.25 g/L)能将大鼠血尿酸降低在50~60 µg/mL之间,差异有统计学意义(P < 0.05);与对照组相比,PEG4000(10.5、5.25、2.625 g/L)粪便排泄量增加,差异有统计学意义(P < 0.05);(2)与对照组相比,治疗组PEG4000(5.25 g/L)血尿素氮也有明显的下降,差异有统计学意义(P < 0.05);(3)与对照组相比,PEG4000(5.25 g/L)降低组织(心、肝、脾、肺、肾、肾上腺)的尿酸含量,差异有统计学意义(P < 0.05);PEG4000(2.625 g/L)降低组织(肝、脾、肾、肾上腺)的尿酸含量,差异有统计学意义(P < 0.05)。 结论 (1)口服PEG4000溶液具有降尿酸作用,其降低血尿酸与增加排便有关;(2)口服PEG4000溶液可以减少肾脏尿酸负担。 -
关键词:
- Kunming-DY大鼠 /
- 尿酸酶缺失 /
- 高尿酸血症 /
- 聚乙二醇4000 /
- 降尿酸作用
Abstract:Objective To explore serum uric acid (SUA) lowering effect of polyethylene glycol 4000 (PEG4000) on male Kunming-DY rats (uricase-deficient rats). Methods A total of 24 45-day male Kunming-DY rats were selected and divided into control group (n = 6) and treatment group: high (10.5 g/L), medium (5.25 g/L) and low (2.625 g/L) PEG4000 dose groups with 6 rats in each group. The control group drank freely and the treatment group drank freely for 1 week. Before and after the experiment, the tail was cut and blood was collected, and the serum, urine and feces of the rats were collected for 24 hours. The food and water intake for 24 hours were recorded, and the main tissues and organs of the rats were harvested. The contents of uric acid, blood urea nitrogen and creatinine in serum samples, uric acid in excreta and uric acid in tissues and organs were tested, and the changes of indexes in control group and treatment group were compared. Results The blood uric acid in the control group was higher than 70 µg/mL, while PEG4000 (10.5 and 5.25 g/L) reduced it to 50-60 g/ml, and the difference was statistically significant (P < 0.05). Compared with the control group, the fecal excretion of PEG4000 (10.5, 5.25, 2.625 g/L) groups increased significantly (P < 0.05). Compared with the control group, the blood urea nitrogen of PEG4000 (5.25 g/L) in the treatment group also decreased significantly, and the difference was statistically significant (P < 0.05). Compared with the control group, PEG4000 (5.25 g/L) group decreased the uric acid content in tissues (heart, liver, spleen, lung, kidney and adrenal gland), and the difference was statistically significant (P < 0.05); PEG4000 (2.625 g/L) decreased the uric acid in tissues (liver, spleen, kidney and adrenal gland), and the difference was statistically significant (P < 0.05). Conclusion Oral PEG4000 solution can reduce uric acid, which is related to the increase of defecation. Oral PEG4000 solution can reduce the burden of uric acid in kidney. -
Key words:
- Kunming-DY rat /
- Uricase deficiency /
- Hyperuricemia /
- PEG4000 /
- Serum uric acid lowering
-
睑板腺功能障碍(meibomian gland dysfunction,MGD)是一个全球普遍性疾病,据流行病学研究报告显示,MGD的发病率较高,尤其在亚洲人群中,其发病率可高达70%[1]。针对MGD患者的治疗过程中仍有部分临床医生尚未对此足够重视,需要重视存在蒸发过强性干眼的患者,这是导致MGD的主要因素[2]。泪液不足引发的泪膜不稳定,加之蒸发速度渐渐加快,泪液渗透压升高是MGD患者常常存在的表现,此外,分泌物在被挤压后呈现颗粒样、泡沫样或者牙膏样,分泌物呈现黄色粘液是病变进展表现[3]。临床治疗此类患者方式主要有人工泪液、促泌剂、强脉冲光(intense pulsed light,IPL)等。IPL是目前有前景的干眼病辅助治疗方法,尤其在MGD相关干眼(蒸发过强型干眼)的治疗上,疗效显著[4]。近来有研究发现,MGD所致干眼症患者运用IPL联合睑板腺按摩治疗效果较好,且经多次IPL治疗后持续性效果更佳,但对于不同频率治疗MGD所致干眼症患者的治疗影响却少有报道[5]。本研究选取玉溪市人民医院眼科2021年3月至2021年12月收治的70例140眼MGD患者采用不同频率IPL治疗,观察不同频率IPL治疗后对MGD患者泪膜稳定性及睑板腺功能的影响,评估IPL治疗频率对患者的疗效,为临床治疗此类患者提供科学依据。
1. 资料与方法
1.1 一般资料
选取玉溪市人民医院眼科2021年3月至2021年12月收治的70例MGD患者共计140眼为实验对象。按照数字表法随机将患者分为A组和B组,每组35例。纳入病例标准:(1)均为双眼发病;(2)经检查(裂隙灯)呈现睑板腺开口异常,睑板腺存在分泌物异常、存在脂质层厚度异常者;(3)所有病例符合《干眼临床诊疗专家共识》[6]中制定的对于睑板腺功能障碍性干眼的诊断认定标准,该标准由中华医学会眼科学会制定;(4)临床资料完整患者。排除标准:(1)眼部存在手术病历者;(2)双眼存在病变者;(3)疗程内存在更改治疗方案以及不配合治疗者;(4)存在合并疾病者,如高血压、糖尿病、风湿性疾病;(5)孕产妇患者;(6)既往存在眼部外伤史、晒伤史或者手术史;(7)依从性差患者。A组:男性17例,女性18例;年龄18~75岁,平均(48.65±8.85)岁;病程15~50 d,平均(32.52±5.47) d。B组:男性15例,女性20例;年龄18~76岁,平均(47.97±9.03)岁;病程15~51 d,平均(33.12±5.56) d。2组患者在性别、年龄、患病时间等一般性资料对比差异无统计学意义(P > 0.05)。本研究经医院伦理会批准,患者家属、患者对所研究内容知情,并自愿签署同意书。
1.2 治疗方法
采用M22(美国科医人有限公司Lumenis Ltd.)对70例患者进行IPL治疗;A组患者在0周,间隔1周(第1周)、间隔2周(第3周)以及间隔4周(第7周)各进行1次IPL治疗,共治疗4次。B组患者在0周,间隔1周(第1周)各进行1次IPL治疗,共治疗2次。每次治疗均由同一位医师完成。患者在治疗前,皮肤须维持清洁且不干燥,不可使用化妆品之类的护肤品,而且,在进行治疗前须清水洗脸后再戴上眼罩,以达到保护眼睛的目的,均匀涂敷医用耦合剂,涂敷范围为鼻部区域及眼睑下方面部,涂敷厚度为1~2 mm。设置能量为9.8~15.0 J/cm2,脉冲光波长为590 nm,治疗过程中医师须戴护目镜。选择治疗点位:在内眦下端至外眦下端选择4个治疗部位,外眦至颞侧(太阳穴附近)1~2 cm处选择1个部位,每只眼共5个部位 . 将治疗头置于偶合剂上,按下开关按钮发出光脉冲,将治疗移至下一个位置。 重复该操作,直到完成所有5个位置的处理。
1.3 观察指标
(1)记录不同频率IPL治疗前后患者泪膜破裂时间:在患者治疗前后采用由北京若水合科技有限公司采购的荧光素钠眼科检测试纸实施检测,将试纸置于结膜囊内进行染色,患者眨眼3~4次后,平视,泪膜破裂时间的认定为裂隙灯下呈现第一个黑斑完成认定,所有操作流程由同一位医师完成;(2)记录不同频率IPL治疗前后患者眼表疾病指数(ooular surfacediseaseindex,OSDI)量表评分[7]:分别在每次治疗前及治疗后,采用OSDI评分,以百分制为标准,共纳入12项眼表疾病症状,分数越高,症状越严重;(3)记录不同频率IPL治疗前后患者眼表综合检查:利用眼表综合分析仪(欧科路光学仪器有限责任公司)定量测量MGD患者泪河高度、平均非侵入性泪膜破裂时间(average noninva-sive tear film break-up time,NIBUTav)、首次非侵入性泪膜破裂时间(first noninvasive tear break-up time,NIBUTf)。每次操作均由同一位医师完成;(4)记录不同频率IPL治疗前后睑板腺分泌能力评分:将睑板腺评估器置于距眼睑边缘1~2 mm处,轻轻按压,以利于睑板腺睑脂排出;在双眼下睑中央部位选取共计5条睑板腺,根据睑板腺排出睑酯难易程度进行评分[8];评分标准设定0~3分: 3分(睑板腺无排出分泌物的能力); 2分( 1个或2个能排泄分泌物的腺体); 1分(3个或4个能排泄分泌物的腺体);0分(所有腺体均有分泌物排出能力)。每次评分均由同一位医师完成;(5)记录不同频率IPL治疗前后睑板腺分泌物状态评分[9],评分标准设定0~4分:分泌物液体状态呈透明、清澈为0分;排出的分泌物液体状态呈浑浊且呈液态状为1分;分泌物状态呈浑浊、颗粒状为2分;分泌物状态如牙膏状且浓稠为3分;无分泌物排出为4分。每次评分均由同一位医师完成;(6)记录不同频率IPL治疗前后角膜荧光素染色评分[10]:患者在眼表综合分析仪完成测量结束后,须休息8 min左右,无任何不适症状出现后可进行眼表综合分析仪检查角膜荧光素染色。浸湿荧光素钠眼科检测试纸(北京若水合科技有限公司)一端后,接触患者下睑结膜,叮嘱MGD患者瞬目多次后再凝视前方,当对焦角膜、结膜上皮层至最清晰的时候进行拍照,检测结果再结合仪器上自带分析角膜上皮点染分级图实施对照,记录角膜与结膜上皮点染分区情况与分级。对角膜荧光素钠评分办法是将角膜分设定为4个象限,规定为轻度(无染色为0分)、中度(染色须少于5个点为1分)和重度(出现丝状物或块状染色,介于以上2者之间为2分)染色3个等级,共0~12分。每次操作均由同一组医师完成,上述所有指标均为双眼均值。
1.4 统计学处理
应SPSS22.0软件进行统计分析。所有实验数据均符合正态分布,计量资料使用均数标准差( $\bar x \pm s $)进行表示,采用独立样本t检验比较2组间差异,采用配对t检验比较组内治疗前后差异,检验水准为α = 0.05,以双侧P < 0.05时,说明差异具有统计学意义。
2. 结果
2.1 不同频率IPL治疗前后MGD患者泪膜破裂时间以及OSDI评分比较
治疗前,A组和B组泪膜破裂时间和OSDI评分比较,差异无统计学意义(P > 0.05);治疗后,A组和B组泪膜破裂时间和OSDI评分均明显降低,差异有统计学意义( P < 0.05);治疗后,A组泪膜破裂时间低于B组,差异有统计学意义( P < 0.05),但A组和B组之间OSDI评分比较,差异无统计学意义( P > 0.05),见 表1。
表 1 比较不同频率IPL治疗前后MGD患者泪膜破裂时间和OSDI评分( $\bar x \pm s $)Table 1. Comparison of tear film rupture time and OSDI score of MGD patients before and after IPL treatment at different frequencies( $\bar x \pm s $)组别 n 泪膜破裂时间(d) t P OSDI评分(分) t P 治疗前 治疗后 治疗前 治疗后 A组 35 69.12 ± 8.05 16.78 ± 3.85 34.701 < 0.001* 23.31 ± 4.56 9.32 ± 3.04 15.102 < 0.001* B组 35 68.87 ± 7.92 28.52 ± 5.12 25.312 < 0.001* 23.18 ± 4.47 9.24 ± 2.81 15.619 < 0.001* t 0.131 10.842 0.120 0.114 P 0.896 < 0.001* 0.905 0.909 *P < 0.05。 2.2 不同频率IPL治疗前后MGD患者眼表临床数据比较
治疗前,A组和B组患者NIBUTav、NIBUTf和泪河高度比较,差异无统计学意义(P > 0.05);治疗后,A组和B组患者NIBUTav、NIBUTf和泪河高度均明显升高,差异有统计学意义( P < 0.05);治疗后,A组NIBUTav、NIBUTf高于B组,而泪河高度低于B组,差异有统计学意义( P < 0.05),见 表2。
表 2 比较不同频率IPL治疗前后MGD患者眼表临床数据(n = 35, $\bar x \pm s $)Table 2. Comparison of ocular surface clinical data of MGD patients before and after IPL treatment at different frequencies (n = 35, $\bar x \pm s $)组别 NIBUTav(s) t P NIBUTf(s) t P 泪河高度(mm) t P 治疗前 治疗后 治疗前 治疗后 治疗前 治疗后 A组 7.98 ± 2.14 12.57 ± 3.21 7.039 < 0.001* 6.08 ± 1.77 9.46 ± 2.14 7.200 < 0.001* 0.18 ± 0.03 0.20 ± 0.02 3.282 0.002* B组 7.86 ± 2.05 11.06 ± 2.86 5.380 < 0.001* 5.94 ± 1.68 8.11 ± 1.89 5.077 < 0.001* 0.17 ± 0.02 0.22 ± 0.04 6.614 < 0.001* t 0.239 2.078 0.339 2.797 1.641 2.646 P 0.811 0.042* 0.735 0.007* 0.106 0.010* *P < 0.05。 2.3 不同频率IPL治疗前后MGD患者睑板腺分泌能力评分和睑板腺分泌物状态评分比较
治疗前,A组和B组患者睑板腺分泌能力评分和睑板腺分泌物状态评分比较,差异无统计学意义(P > 0.05);治疗后,A组和B组患者睑板腺分泌能力评分和睑板腺分泌物状态评分均下降,差异有统计学意义( P < 0.05);治疗后,A组睑板腺分泌能力评分和睑板腺分泌物状态评分低于B组,差异有统计学意义( P < 0.05),见 表3。
表 3 比较不同频率IPL治疗前后MGD患者睑板腺分泌能力和睑板腺分泌物状态评分( $\bar x \pm s $)Table 3. Comparison of meibomian gland secretion capacity and meibomian gland secretion status scores of MGD patients before and after IPL treatment at different frequencies ( $\bar x \pm s $)组别 n 睑板腺分泌能力评分(分) t P 睑板腺分泌物状态评分(分) t P 治疗前 治疗后 治疗前 治疗后 A组 35 17.52 ± 3.21 5.86 ± 1.32 19.874 < 0.001* 14.89 ± 3.05 5.48 ± 1.18 17.023 < 0.001* B组 35 17.36 ± 3.13 12.34 ± 2.42 7.506 < 0.001* 14.75 ± 2.86 8.64 ± 2.17 10.069 < 0.001* t 0.211 13.907 0.198 7.569 P 0.833 < 0.001* 0.844 < 0.001* *P < 0.05。 2.4 不同频率IPL治疗前后MGD患者角膜荧光素染色情况比较
治疗前,A组和B组患者角膜荧光素染色评分比较,差异无统计学意义(P > 0.05);治疗后,A组和B组患者角膜荧光素染色评分均下降,差异有统计学意义( P < 0.05);治疗后,A组角膜荧光素染色评分高于B组,差异有统计学意义( P < 0.05),见 表4。
表 4 不同频率IPL治疗前后MGD患者角膜荧光素染色情况比较( $\bar x \pm s $)Table 4. Comparison of corneal luciferin staining of MGD patients before and after IPL treatment at different frequencies ( $\bar x \pm s $)组别 n 角膜荧光素染色评分(分) t P 治疗前 治疗后 A组 35 3.25 ± 0.35 2.21 ± 0.23 14.691 < 0.001* B组 35 3.17 ± 0.29 2.08 ± 0.21 18.010 < 0.001* t 0.225 2.469 P 0.823 0.016* *P < 0.05。 3. 讨论
睑板腺功能障碍以终末导管阻塞、腺体分泌或分泌量异常为特征,可引起眼表刺激以及泪膜稳定性异常等症状,通常伴有眼表炎症及损伤等情况,此症状属于是一种慢性弥漫性眼表病变疾病[11]。对于MGD引起的相关干眼症状,传统方法包括眼睑热敷、睑缘清洁、人工眼泪以及采用抗炎药物进行缓解,但效果无法长期维持。近年来,研究表明IPL治疗对MGD起到改善作用,而对于不同频率IPL治疗MGD患者影响临床疗效的研究不多。有研究显示[12],多次IPL的治疗效果虽然具有累积性,但随着第次间隔时间的延长,累加效果会下降。因此,临床治疗上在积极寻找既安全且疗效佳的IPL治疗频率。
MGD可导致泪膜不稳定,而泪膜失稳是干眼症发病的主要机制[13]。泪膜包含最上面的脂质层、中间的水液层和下面的黏蛋白层的3层架构;泪膜脂的质层主要作用是减慢泪液水液层的蒸发速率,主要是由睑板腺分泌的睑酯构成。正常状态下,睑酯为透明油状液体;它在人眨眼时眼肌的机械作用下,沿着垂直的睑板腺管向睑缘开口处流通,最终覆盖在泪膜最表层;病理状态下,可见睑酯浑浊,甚至凝固阻滞睑板腺,严重的会影响到睑板腺在结构上的完整性。MGD直接影响到泪膜的脂质层,使泪膜失去稳定性[14]。本研究结果显示,与治疗前相比,A组和B组泪膜破裂时间和OSDI评分均明显降低;A组泪膜破裂时间低于B组,而A组和B组之间OSDI评分比较,差异无统计学意义。相关研究显示,感染以及炎症是直接导致眼部疾病发生病变的重要原因,对病原微生物繁殖的有效控制,缓解炎症发生反应是治疗相关疾病的首要任务。IPL是一种经过聚焦和滤过后形成的脉冲光,本质是一种非相干的普通光,刺激皮肤中血红蛋白、黑色素和水3种靶色素,诱发光热效应。IPL在皮肤科中广泛用于治疗,鲜红斑痣、痤疮和色素病变等皮肤病[15]。IPL具有无创、简单、安全且有效等优势,逐步成为眼科领域中治疗MGD导致干眼症的新型治疗方法,该治疗方法能够缓解炎症,能有效增强IPL对细菌的杀灭作用。既往研究结果显示[4],IPL能够改善MGD等眼表炎症,应用在治疗MGD患者中获得良好效果。本研究结果提示,采用不同频率IPL治疗MGD患者能有效杀灭细菌,减缓泪膜破裂时间,炎症相关反应得到抑制,达到维持泪膜稳定性目的。
IPL可以抑制住炎症介质,促使眼睑脂肪排出,减少螨虫以及皮肤表面细菌的数量,加强泪膜的稳定性,减少泪膜水层的蒸发。 因此,MGD患者的症状和体征可以得到明显改善。本研究结果显示,治疗后,A组和B组患者NIBUTav、NIBUTf和泪河高度均明显升高,且A组NIBUTav、NIBUTf高于B组,而泪河高度低于B组。同时研究还发现,不断逐渐增加的治疗次数所累加的治疗效果更加突出,究其原因主要是睑板腺不断提高的分泌能力促使分泌物性状的不断改善,所以与IPL治疗次数有紧密关系。文中角膜荧光素染色结果,治疗后,A组和B组患者角膜荧光素染色评分均下降,且A组角膜荧光素染色评分高于B。多项研究表明[12],IPL可有效治疗MGD患者,改善临床症状,泪膜稳定性提高,睑板腺功能得到改善。能够消除炎症的主要来源是非正常血管被IPL所产生的热效应破坏,炎症介导因子无法到达腺体,而这些炎症因子可能会引起睑板腺功能障碍;此外,IPL的热能量间接被睑板腺吸收后,使睑板腺融化,打开堵塞的腺体口;降低睑缘蠕形螨和细菌的载量。正是因为可通过多种机制共同作用于睑板腺,IPL才会快速改善MGD患者干眼症状并且改善睑板腺功能[16]。本研究结果说明,不同频率IPL均可改善MGD患者眼表症状和体征。
综上所述,本文分析70例MGD患者,相比于治疗前,随着治疗间隔增加,泪膜破裂时间逐渐下降;不同治疗间隔周期对MGD患者睑板腺的功能均有不同程度的改善,根据患者具体情况选择合适的IPL治疗频率可在一定程度上确保治疗安全的安全性和有效性。
-
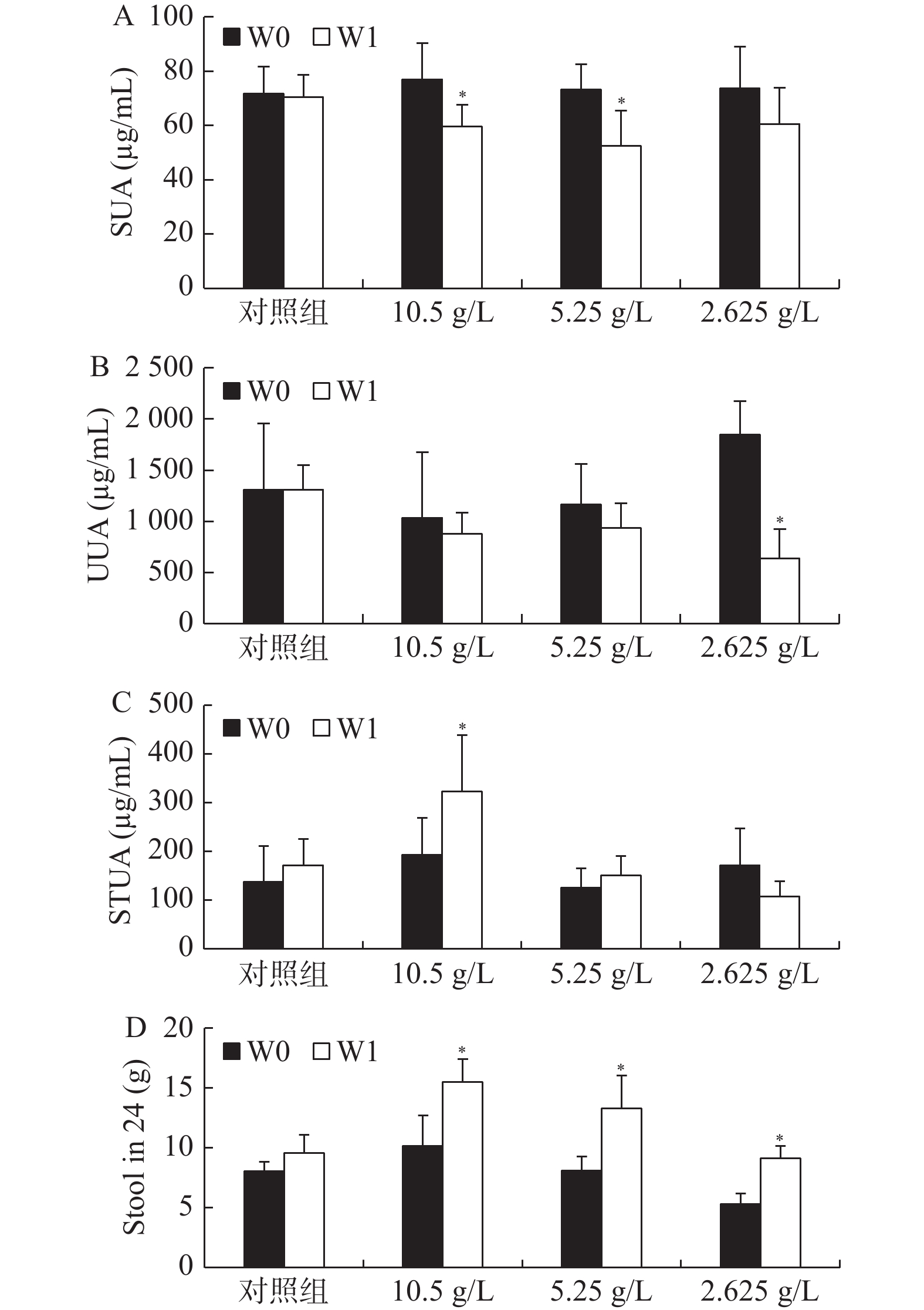
图 1 PEG4000对Kunming-DY大鼠的降尿酸作用[(
$\bar x \pm s $ ),n = 6]A:1周前后大鼠血清尿酸(SUA)变化;B:1周前后大鼠尿液尿酸(UUA)浓度变化;C:1周前后大鼠粪便尿酸(StUA)含量变化;D:1周前后24h粪便尿酸总量变化。*P < 0.05。
Figure 1. PEG4000 lowered serum uric acid in Kunming-DY rats [(
$\bar x \pm s $ ),n = 6]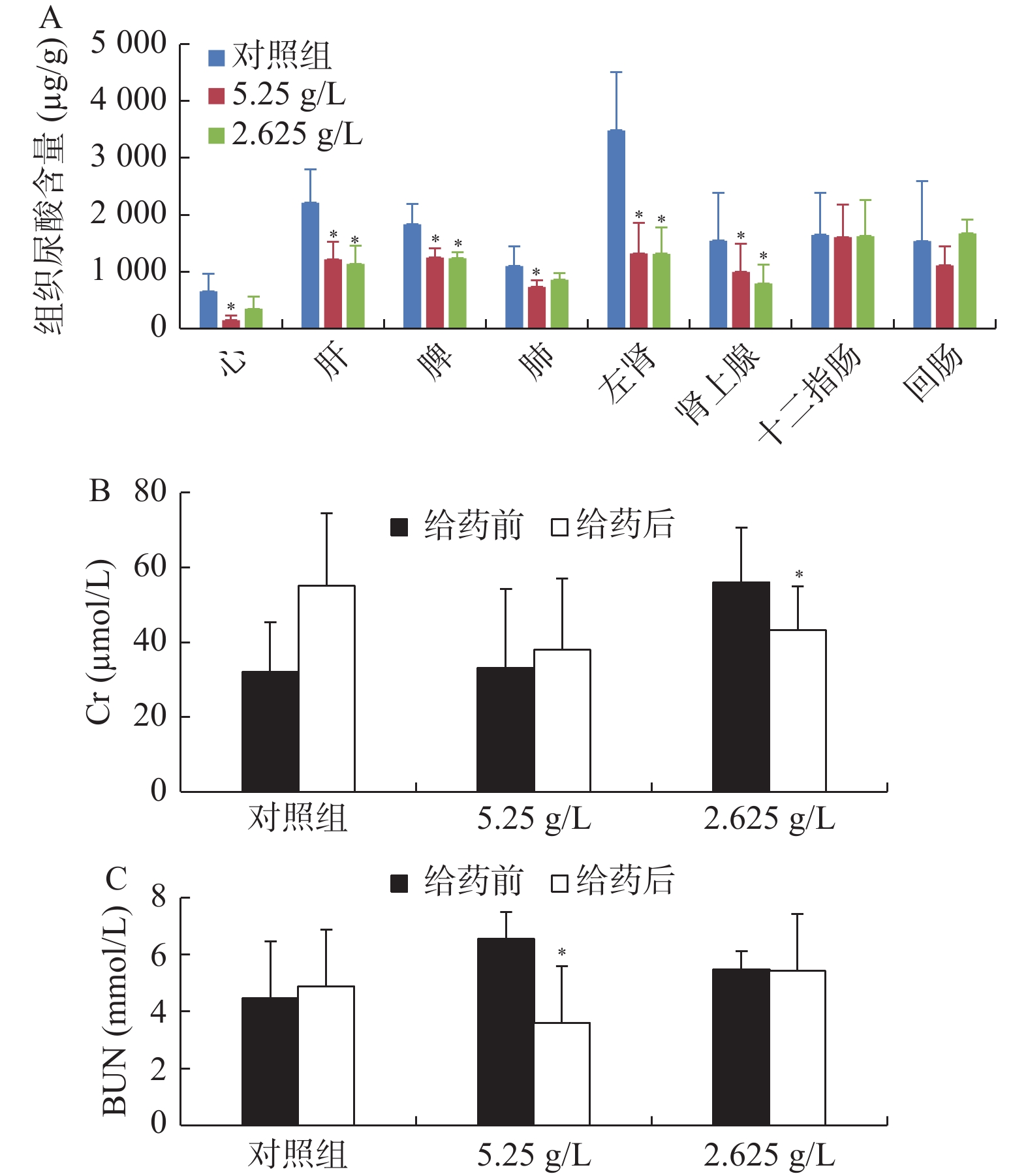
图 2 PEG4000对Kunming-DY大鼠的组织尿酸、血肌酐、血尿素氮的影响[(
$\bar x \pm s $ ),n = 6]A:1周后Kunming-DY大鼠脏器尿酸(UA)含量变化;B:1周前后Kunming-DY大鼠血肌酐含量(Cr)变化;C:1周前后Kunming-DY大鼠血尿素氮(BUN)变化。*P < 0.05。
Figure 2. Effects of PEG4000 on tissue uric acid,blood creatinine and blood urea nitrogen in Kunming-DY rats [(
$\bar x \pm s $ ),n = 6]表 1 实验前后多个指标的变化值[(
$ \bar x \pm s $ ),n = 6](1)Table 1. Changes of various indexes before and after treatment [(
$ \bar x \pm s $ ),n = 6](1)项目 24 h尿量(mL) 尿液尿酸(μg/mL) 24 h尿液尿酸(mg) W0 W1 W1-W0 W0 W1 W1-W0 W0 W1 W1-W0 对照组 29.3 ± 5.5 31.4 ± 3.7 2.2 ± 4.4 1307.8 ± 647.2 1308.6 ± 241.2 0.8 ± 656.9 37.5 ± 19.7 41.5 ± 10.3 4.0 ± 19.3 10.5 g/L 44.7 ± 7.8 34.3 ± 4.4 −10.3 ± 11.4 1034.0 ± 638.9 877.8 ± 209.0 −156.2 ± 746.4 42.3 ± 18.6 30.0 ± 7.5 −12.3 ± 19.8 5.25 g/L 35.7 ± 1.6 43.9 ± 7.4 8.13 ± 7.7 1165.0 ± 396.5 936.3 ± 238 −228.7 ± 375.2 41.0 ± 14.4 41.1 ± 13.6 0.1 ± 17.1 2.625 g/L 37.7 ± 3.2 39.1 ± 11.1 1.4 ± 10.5 1849.2 ± 324.0 636.0 ± 288.8 −1213.2+586.1 70.3 ± 16.5 24.9 ± 11.3 −45.4 ± 25.6 F 4.65 4.31 6.20 P 0.00* 0.00* 0.00* 与对照组比较,*P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 1 实验前后多个指标的变化值[(
$ \bar x \pm s $ ),n = 6](2)Table 1. Changes of various indexes before and after treatment [(
$ \bar x \pm s $ ),n = 6](2)项目 24 h粪便(g) 粪便尿酸(μg/g) 24 h粪便尿酸(mg) W0 W1 W1-W0 W0 W1 W1-W0 W0 W1 W1-W0 对照组 8.1 ± 0.9 9.6 ± 1.7 1.5 ± 1.7 137.9 ± 73.6 171.5 ± 53.8 33.6 ± 92.5 1.2 ± 0.8 1.6 ± 0.4 0.4 ± 0.9 10.5 g/L 10.1 ± 2.8 15.5 ± 2.1 5.3 ± 2.4 192.7 ± 75.5 323.6 ± 114.4 130.9 ± 102.9 2.1 ± 1.5 5.0 ± 1.9 2.9 ± 1.7 5.25 g/L 8.4 ± 1.1 14.3 ± 2.7 5.9 ± 2.8 125.5 ± 39.9 150.3 ± 40.7 24.7 ± 42.5 1.0 ± 0.3 2.1 ± 0.7 1.1 ± 0.5 2.625 g/L 9.6 ± 0.9 7.0 ± 1.0 2.6 ± 1.2 171.8 ± 41.3 107.2 ± 31.8 −64.6 ± 63.6 1.2 ± 0.3 1.0 ± 0.4 −0.2 ± 0.6 F 8.07 5.32 6.85 P 0.00* 0.00* 0.00* 与对照组比较,*P < 0.05。
下载: 导出CSV
表 1 实验前后多个指标的变化值[(
$ \bar x \pm s $ ),n = 6] (3)Table 1. Changes of various indexes before and after treatment [(
$ \bar x \pm s $ ),n = 6] (3)项目 24 h排尿酸总量(mg) 24 h进食量(g) 24 h饮水量(mL) W0 W1 W1-W0 W0 W1 W1-W0 W0 W1 W1-W0 对照组 38.7 ± 19.9 43.0 ± 10.1 4.4 ± 19.0 18.1 ± 3.6 21.8 ± 1.2 3.7 ± 2.9 51.3 ± 5.5 59.4 ± 5.4 8.2 ± 7.4 10.5g/L 44.4 ± 17.7 35.0 ± 7.4 9.4 ± 20.0 20.4 ± 2.6 24.5 ± 2.4 4.1 ± 1.6 69.9 ± 12.4 72.9 ± 14.0 3.0 ± 11.6 5.25g/L 42.2 ± 19.1 41.4 ± 18.4 −0.8 ± 15.2 22.0 ± 2.8 26.9 ± 1.9 4.9 ± 3.2 56.9 ± 3.9 71.2 ± 12.7 14.3 ± 14.9 2.625g/L 57.8 ± 22.7 60.7 ± 17.7 2.9 ± 15.2 19.9 ± 0.7 23.2 ± 3.5 3.3 ± 0.7 59.6 ± 3.5 70.1 ± 7.1 13.2 ± 6.7 F 0.57 1.70 4.99 P 0.72 1.61 0.00* 与对照组比较,*P < 0.05。
下载: 导出CSV
表 2 实验前后多种指标用体重校正后[(
$ \bar x \pm s $ ),n = 6] (1)Table 2. Various indexes were balanced by weight before and after treatment [(
$ \bar x \pm s $ ),n = 6] (1)项目 相对排尿量(mL/200 g) 相对尿液尿酸(mg/200 g) 相对排便量(g/200 g) W0 W1 W1-W0 W0 W1 W1-W0 W0 W1 W1-W0 对照组 29.9 ± 5.5 24.4 ± 2.5 −5.5 ± 4.5 37.6 ± 18.4 32.0 ± 7.2 −5.6 ± 19.0 8.2 ± 1.0 7.4 ± 1.3 −0.8 ± 1.3 10.5 g/L 46.5 ± 7.7 35.7 ± 4.9 −10.8 ± 12.3 44.1 ± 20.2 23.7 ± 7.7 −20.4 ± 19.0 10.4 ± 2.6 12.0 ± 1.7 1.6 ± 3.0 5.25 g/L 33.6 ± 3.2 34.1 ± 5.1 0.5 ± 6.6 34.2 ± 17.6 28.4 ± 14.1 −5.8 ± 17.8 7.8 ± 1.1 11.0 ± 1.7 3.2 ± 2.1 2.625 g/L 38.6 ± 2.3 31.5 ± 8.3 −7.0 ± 8.3 72.0 ± 16.1 20.2 ± 9.3 −51.8 ± 23.6 7.2 ± 0.9 7.4 ± 0.9 0.2 ± 1.1 F 7.89 6.91 7.2 P 0.00* 0.00* 0.00* 与对照组比较,*P < 0.05。
下载: 导出CSV
表 2 实验前后多种指标用体重校正后[(
$ \bar x \pm s $ ),n = 6] (2)Table 2. Various indexes were adjusted by weight before and after the experimen[(
$ \bar x \pm s $ ),n = 6](2)项目 相对粪便尿酸(mg/200 g) 相对尿酸排泄总量(mg/200 g) 相对进食量(g/200 g) W0 W1 W1-W0 W0 W1 W1-W0 W0 W1 W1-W0 对照组 1.2 ± 0.7 1.3 ± 0.3 0.1 ± 0.9 38.8 ± 18.6 33.3 ± 7.0 −5.5 ± 18.8 18.4 ± 3.4 17.0 ± 0.7 −1.5 ± 3.2 10.5 g/L 2.2 ± 1.5 3.8 ± 1.3 1.6 ± 1.5 46.3 ± 19.3 27.5 ± 7.7 −18.8 ± -5.6 21.2 ± 2.7 19.1 ± 2.7 −2.1 ± 2.1 5.25 g/L 1.0 ± 0.5 1.6 ± 0.5 0.6 ± 0.4 39.1 ± 17.6 31.7 ± 13.9 −7.4 ± 17.4 20.7 ± 3.3 20.9 ± 1.4 0.2 ± 3.1 2.625 g/L 1.2 ± 0.4 0.8 ± 0.3 −0.4 ± 0.6 59.8 ± 24.8 49.4 ± 15.7 −10.3 ± -9.8 20.4 ± 1.1 18.8 ± 0.7 −1.6 ± 0.8 F 6.47 0.62 2.11 P 0.00* 0.68 0.09 与对照组比较,*P < 0.05。
下载: 导出CSV
表 2 实验前后多种指标用体重校正后[(
$ \bar x \pm s $ ),n = 6] (3)Table 2. Various indexes were adjusted by weight Before and after the experiment[(
$ \bar x \pm s $ ),n = 6] (3)项目 相对饮水量(mL/200 g) W0 W1 W1-W0 对照组 52.2 ± 4.5 46.4 ± 6.3 −5.8 ± 4.1 10.5 g/L 72.5 ± 12.0 56.6 ± 10.6 −15.9 ± 13.0 5.25 g/L 53.5 ± 5.7 55.5 ± 9.9 2.0 ± 12.8 2.625 g/L 61.2 ± 3.9 56.9 ± 6.8 −4.3 ± 5.9 F 7.84 P 0.00* 与对照组比较,*P < 0.05。
下载: 导出CSV
表 3 实验前后大鼠肾功能变化[(
$\bar x \pm s $ ),n = 6]Table 3. Changes of renal function indexes before and after treatment [(
$\bar x \pm s $ ),n = 6]项目 血肌酐浓度(µmol/L) 尿素氮浓度(mmol/L) W0 W1 W1-W0 W0 W1 W1-W0 对照组 32.2 ± 13.1 55.1 ± 17.7 22.9 ± 22.4 4.5 ± 1.9 4.9 ± 2.2 0.4 ± 2.2 5.25 g/L 33.1 ± 21.1 38.1 ± 18.9 5.0 ± 7.3 6.5 ± 0.9 3.7 ± 1.8 −2.8 ± 1.7 2.625 g/L 56.0 ± 14.5 43.2 ± 11.7 −12.8 ± 20.8 5.5 ± 0.6 5.4 ± 0.7 −0.1 ± 0.6 F 0.58 6.14 P 0.01* 0.01* 与对照组比较,*P < 0.05。
下载: 导出CSV
-
[1] 叶佩玉,赵小元,闫银坤,等. 儿童高尿酸血症与心血管代谢异常发生风险[J]. 中华流行病学杂志,2021,42(3):433-439. doi: 10.3760/cma.j.cn112338-20200825-01094 [2] 王诗涵,袁涛. 儿童及青少年高尿酸血症和痛风的危险因素、病因及诊治策略[J]. 中华临床营养杂志,2021,29(3):163-170. doi: 10.3760/cma.j.cn115822-20210225-00043 [3] 徐璧云. 尿酸高:“三高”以外的“第四高”[J]. 家庭医药,2014,13(6):20-21. [4] 金剑. 高尿酸血症 危险的第四高[J]. 江苏卫生保健,2016,18(23):23. [5] 刘杨从,李妍,张耕. 18例苯溴马隆不良反应/事件分析[J]. 中国医院药学杂志,2016,36(6):507-510. doi: 10.13286/j.cnki.chinhosppharmacyj.2016.06.20 [6] 朱飞燕,孟群. 苯溴马隆致重度药物性肝损伤1例[J]. 肝脏,2017,22(10):973-974. doi: 10.3969/j.issn.1008-1704.2017.10.036 [7] 潘鑫,谢攀,常欢,等. 别嘌醇过敏可能成为肾衰竭的免疫学转机吗?[J]. 免疫学杂志,2022,38(1):88-92. [8] 陈一萍,张劼,周嘉,等. 别嘌醇药物不良反应风险因素研究进展[J]. 广西医科大学学报,2019,36(1):137-141. [9] 赵德杰,解广东,乔全来,等. 聚乙二醇4000治疗便秘的研究进展[J]. 中国中西医结合外科杂志,2018,24(5):659-662. doi: 10.3969/j.issn.1007-6948.2018.05.033 [10] 余炳取,侯陈凤,陈佳圆,等. 揿针、聚乙二醇4000散联合生物反馈疗法治疗功能性便秘临床研究[J]. 新中医,2020,52(2):130-133. [11] Ichijima R,Suzuki S,Esaki M,et al. Efficacy of macrogol 4000 plus electrolytes in bowel preparation for colonoscopy in patients with chronic constipation[J]. BMC Gastroenterology,2021,21(1):387. doi: 10.1186/s12876-021-01976-2 [12] Yu Y,Zhang N,Dong X,et al. Uricase-deficient rat is generated with CRISPR/Cas9 technique[J]. PeerJ,2020,8(4):8971. [13] 张谭畅,闵红燕,刘晓园. 非布司他对比别嘌醇在治疗痛风中不良反应的发生率[J]. 北方药学,2020,17(5):152-153. doi: 10.3969/j.issn.1672-8351.2020.05.113 [14] 郭钦惠,方宏,陈俊文,等. 非布司他药物相关不良反应文献分析[J]. 中国医学创新,2020,17(22):104-107. doi: 10.3969/j.issn.1674-4985.2020.22.027 [15] 钟燕,姜怡雯,蒋娅莉,等. 非布司他心脏不良反应信号的数据挖掘和分析[J]. 中国药房,2022,33(2):225-229. doi: 10.6039/j.issn.1001-0408.2022.02.16 [16] Hosomi A,Nakanishi T,Fujita T,et al. Extra-renal elimination of uric acid via intestinal efflux transporter BCRP/ABCG2[J]. S. R. Singh. PLoS ONE,2012,7(2):30456. doi: 10.1371/journal.pone.0030456 [17] Kelly S J,Delnomdedieu M,Oliverio M I,et al. Diabetes insipidus in uricase-deficient mice:A model for evaluating therapy with poly(ethylene glycol)-modified uricase[J]. Journal of the American Society of Nephrology:JASN,2001,12(5):1001-1009. doi: 10.1681/ASN.V1251001 [18] Lyseng-Williamson K A. Macrogol (polyethylene glycol) 4000 without electrolytes in the symptomatic treatment of chronic constipation:A profile of its use[J]. Drugs & Therapy Perspectives:For Rational Drug Selection and Use,2018,34(7):300-310. [19] 关向阳,李彩霞. 聚乙二醇4000联合麻仁软胶囊治疗儿童便秘的临床疗效分析[J]. 中国现代药物应用,2021,15(10):157-159. doi: 10.14164/j.cnki.cn11-5581/r.2021.10.059 [20] 林存侠,罗建平. 成人功能性便秘经聚乙二醇4000治疗效果及安全性分析[J]. 临床研究,2018,26(1):108-110. doi: 10.3969/j.issn.1004-8650.2018.01.056 [21] Yun Y,Yin H,Gao Z,et al. Intestinal tract is an important organ for lowering serum uric acid in rats[J]. G. Kunze. PLOS ONE,2017,12(12):0190194. doi: 10.1371/journal.pone.0190194 [22] 范楠,段为钢,云宇. 雄性Kunming-DY大鼠血尿酸水平的主要影响因素[J]. 云南中医学院学报,2020,43(6):12-17. doi: 10.19288/j.cnki.issn.1000-2723.2020.06.003 [23] Nakatochi M,Kanai M,Nakayama A,et al. Genome-wide meta-analysis identifies multiple novel loci associated with serum uric acid levels in Japanese individuals[J]. Communications Biology,2019,2(1):115. doi: 10.1038/s42003-019-0339-0 [24] Meng J,Lv Q,Sui A,et al. Hyperuricemia induces lipid disturbances by upregulating the CXCL-13 pathway[J]. American Journal of Physiology. Gastrointestinal and Liver Physiology,2022,322(2):256-267. doi: 10.1152/ajpgi.00285.2021 [25] Matsuo H,Ishikawa E,Machida H,et al. Efficacy of xanthine oxidase inhibitor for chronic kidney disease patients with hyperuricemia[J]. Clinical and Experimental Nephrology,2020,24(4):307-313. doi: 10.1007/s10157-019-01829-z 期刊类型引用(2)
1. 侯肖霖,杨建红,李宁,段为钢. 论“血浊伤脉”. 云南中医药大学学报. 2025(01): 24-34 .  百度学术
百度学术2. 李丹,万绪莲,李律宇,云宇,罗光云,刘韦兵,林公府,李宁,黎勇坤,段为钢. 尿酸酶缺失大鼠肠道菌群的变化. 昆明医科大学学报. 2023(02): 27-32 . 本站查看其他类型引用(0)
-

 下载:
下载:


















 点击查看大图
点击查看大图
计量
- 文章访问数: 3326
- HTML全文浏览量: 2062
- PDF下载量: 123
- 被引次数: 2
