

Diagnostic Value of Adenosine Stress-resting Gated Myocardial Perfusion Imaging in the Diagnosis of Three-vessel Coronary Heart Disease
-
摘要:
目的 评价腺苷负荷-静息门控心肌灌注显像对冠心病三支病变的诊断价值。 方法 回顾性纳入2021年1月至2022年12月于昆明医科大学附属延安医院行冠脉造影并确诊为冠心病的患者318例,根据冠脉造影结果,将318例冠心病患者分为三支病变组166例与非三支病变组(单支与双支病变组)152例,所有入组对象于两周内行腺苷负荷-静息GMPI,收集患者的腺苷负荷-静息GMPI心肌灌注参数(SSS、SRS、SDS)、心功能参数(LVEF、LVEDV、LVESV)、左心室机械收缩同步性参数(PSD、PHB)等。探讨腺苷负荷-静息门控心肌灌注显像对冠心病三支病变的诊断价值。 结果 灌注参数中SSS具有最高的AUC为0.781,心功能参数中sLVEF具有最高的AUC为0.748,同步性参数中sPHB具有最高的AUC为0.724;联合参数的AUC均高于灌注参数、心功能参数及同步性参数(P均 < 0.05)。比较三支病变组与非三支病变组负荷较静息的变化值:三支病变组与非三支病变组ΔLVESV、ΔLVEF存在统计学差异(P < 0.05)。 结论 腺苷负荷-静息门控心肌灌注显像灌注、心功能及同步性参数均对冠心病三支病变具有较高诊断价值,三种参数联合检测对冠心病三支病变诊断具有更高的价值。 -
关键词:
- 腺苷 /
- 负荷门控心肌灌注显像 /
- 冠心病 /
- 三支病变
Abstract:Objective To evaluate the diagnostic value of adenosine load - resting gated myocardial perfusion imaging for three-vessel disease in coronary artery disease (CAD) patients using coronary angiography as the gold standard. Methods A retrospective study was conducted, including 318 patients diagnosed with CAD who underwent coronary angiography at Yanan Hospital Affiliated to Kunming Medical University from January 2021 to December 2022. Based on the results of coronary angiography, the 318 CAD patients were divided into a three-vessel disease group (n = 166) and a non-three-vessel disease group (single and double vessel disease group, n = 152). All the subjects underwent adenosine stress-resting GMPI within two weeks. Adenosine stress-resting GMPI myocardial perfusion parameters (SSS, SRS, SDS), cardiac function parameters (LVEF, LVEDV, LVSV) and left ventricular mechanical contraction synchronization parameters (PSD, PHB) were collected. The diagnostic value of adenosine stress - resting gated myocardial perfusion imaging for three-vessel disease in CAD was explored. Results Among the perfusion parameters, SSS had the highest AUC of 0.781, while sLVEF had the highest AUC of 0.748 among cardiac function parameters, and sPHB had the highest AUC of 0.724 among synchrony parameters. The AUCs of combined parameters were all higher than those of perfusion parameters, cardiac function parameters, and synchrony parameters (P < 0.05). The changes in ΔLVESV and ΔLVEF between the three-vessel disease group and the non-three vessel disease group showed statistical significance (P < 0.05). Conclusion The perfusion, cardiac function and synchronization parameters of adenosine stress-resting gated myocardial perfusion imaging have high diagnostic value for three-vessel coronary heart disease, and the combined detection of the three parameters provides even greater diagnostic value for three-vessel coronary heart disease. -
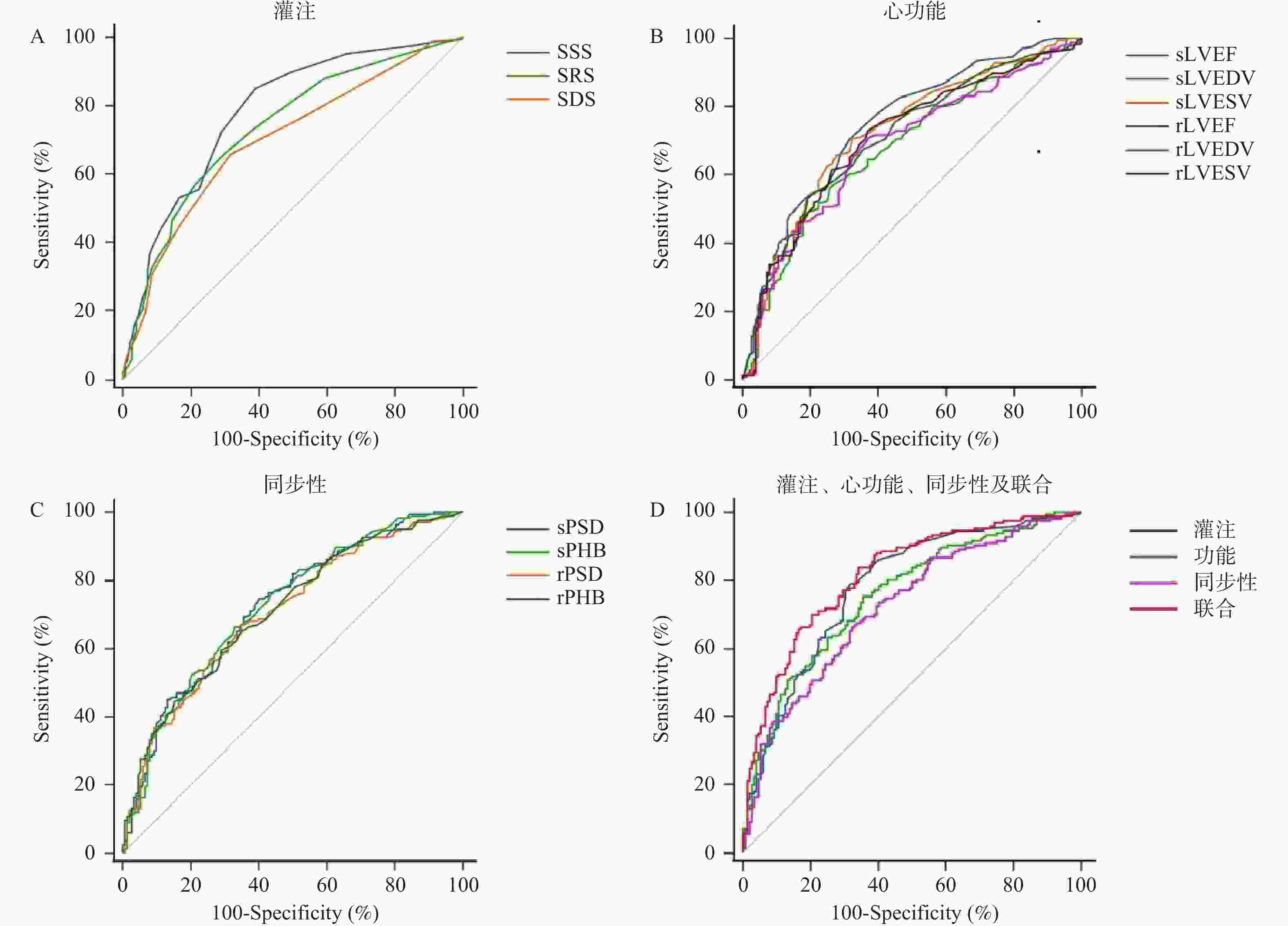
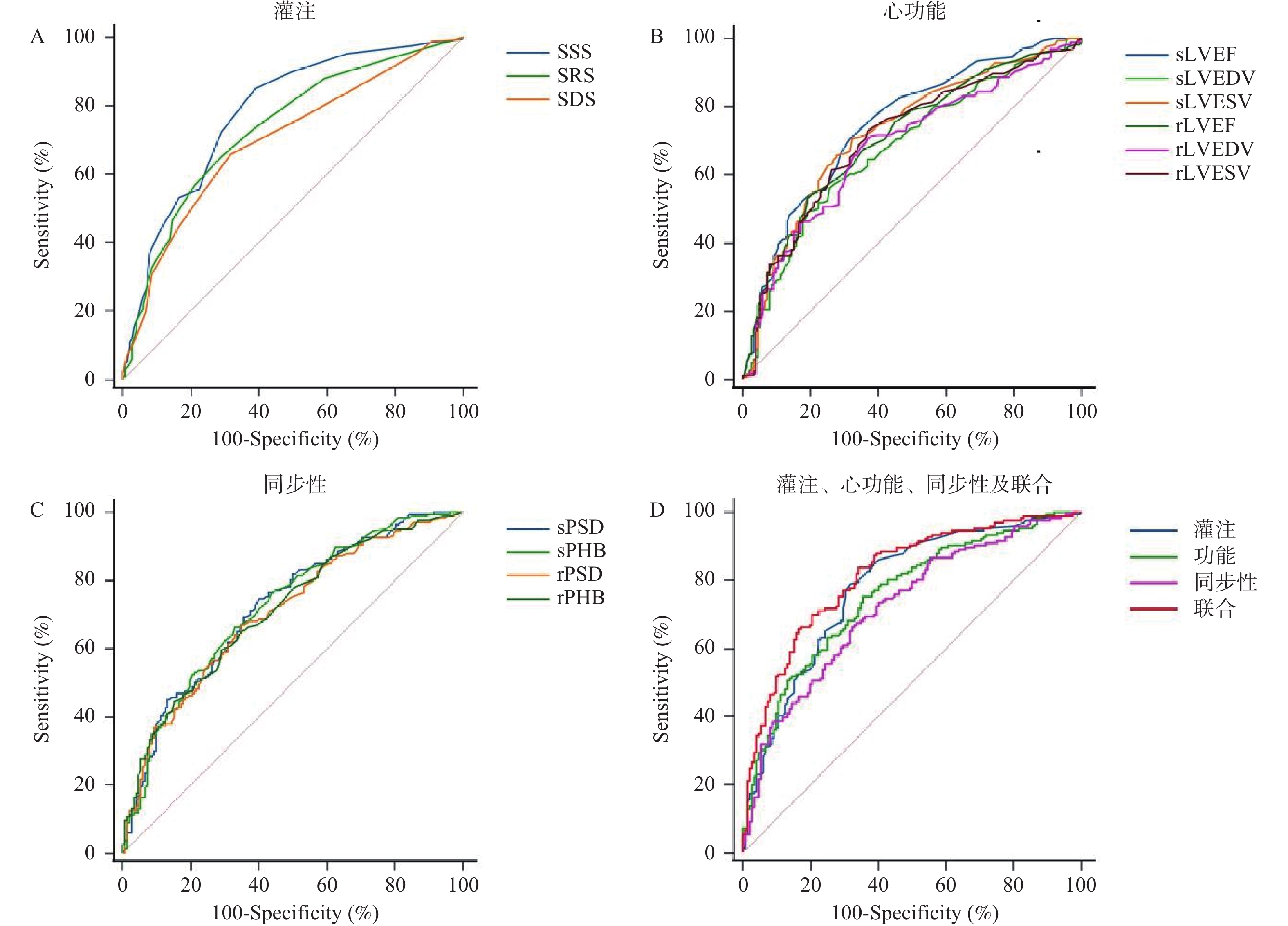
图 1 腺苷负荷门控心肌灌注显像
A:腺苷负荷GMPI灌注参数;B:左心功能参数;C:同步性参数诊断冠心病三支病变的ROC曲线;D:为灌注参数(SSS + SRS + SDS)、左心功能参数(sLVEF + sLVEDV + sLVESV + rLVEF + rLVEDV + rLVESV)、同步性参数(sPSD + sPHB + rPSD + rPHB)及联合参数诊断冠心病三支病变的ROC曲线:联合代表灌注参数 + 左心功能参数 + 同步性参数。
Figure 1. Adenosine stress perfusion parameters
表 1 三支病变组与非三支病变组一般资料的比较[($\bar x \pm s $)/n(%)]
Table 1. Comparison of general data between the three-vessel disease group and the non-three-vessel disease group [($\bar x \pm s $)/n(%)]
一般资料 三支病变组(n = 166) 非三支病变组(n = 152) 检验值 P 性别(男/女) 132/34 110/42 2.230a 0.135 年龄(岁) 59.7 ± 9.3 60.5 ± 9.8 0.765b 0.445 BMI(kg/m2) 24.56 ± 3.16 24.90 ± 3.46 0.926b 0.355 吸烟[n(%)] 85(51.2) 55(36.2) 7.265a 0.007* 高血压[n(%)] 105(63.3) 99(65.1) 0.122a 0.727 既往心梗[n(%)] 31(18.7) 9(5.9) 11.737a 0.001* 糖尿病[n(%)] 60(36.1) 40(26.3) 3.556a 0.059 高胆固醇血症[n(%)] 14(8.4) 11(7.2) 0.157a 0.692 高甘油三酯血症[n(%)] 85(51.2) 60(39.5) 4.402a 0.036* a为χ2值,b为t值;*P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 三支病变组与非三支病变组腺苷负荷GMPI参数的比较[M(P25,P75)]
Table 2. Comparison of GMPI parameters of adenosine stress between three-vessel disease group and non-three-vessel disease group [M(P25,P75)]
项目 三支病变组(n = 166) 非三支病变组(n = 152) 检验值(Z) P SSS(分) 13(9,19) 6(5,11) 8.676 <0.001* SRS(分) 5(2,11) 2(1,4) 7.264 <0.001* SDS(分) 7(5,9) 5(3,6) 6.178 <0.001* sPSD (°) 27.6(19.4,56.7) 17.5(13.1,26.0) 6.868 <0.001* sPHB(°) 82.0(56.0,172) 53.0(39.0,72.5) 6.888 <0.001* rPSD (°) 20.3(13.8 ,47.2) 13.8(10.6 ,19.2) 6.312 <0.001* rPHB(°) 56.5(42.0,137.0) 41.0(33.0,55.0) 6.504 <0.001* sLVEF(%) 52(26,61) 63(56,68) 7.649 <0.001* sLVEDV(mL) 115(87,162) 88(73,110) 5.533 <0.001* sLVESV(mL) 56(35,116) 32(23,46) 6.965 <0.001* sSV(mL) 49(38,61) 53(44,61) 2.362 <0.001* rLVEF(%) 53(32,62) 64(57,69) 6.494 <0.001* rLVEDV(mL) 108(82,155) 82(70,106) 5.643 <0.001* rLVESV(mL) 50(32,109) 29(22,44) 6.442 <0.001* rSV(mL) 49(38,60) 51(44,58) 1.228 0.219 *P < 0.05。
下载: 导出CSV
表 3 腺苷负荷/静息GMPI参数对冠心病三支病变的诊断效能
Table 3. Diagnostic efficacy of adenosine stress/rest GMPI parameters in three-vessel coronary heart disease
项目 AUC P 95%CI 灵敏度(%) 特异度(%) SSS≥7(分) 0.781 <0.001* 0.731~0.825 84.94 61.18 SRS≥3(分) 0.734 <0.001* 0.682~0.782 65.06 71.05 SDS≥5(分) 0.699 <0.001* 0.646~0.749 65.66 68.42 sLVEF≤59(%) 0.748 <0.001* 0.697~0.795 70.48 68.42 sLVEDV≥108(mL) 0.680 <0.001* 0.625~0.731 56.02 74.34 sLVESV≥38(mL) 0.726 <0.001* 0.673~0.774 70.48 67.76 rLVEF≤54(%) 0.711 <0.001* 0.657~0.760 53.01 80.92 rLVEDV≥89(mL) 0.683 <0.001* 0.629~0.734 70.48 63.16 rLVESV≥33(mL) 0.709 <0.001* 0.656~0.758 72.89 63.16 sPSD≥19.5(°) 0.723 <0.001* 0.670~0.771 74.70 59.87 sPHB≥62(°) 0.724 <0.001* 0.671~0.772 66.27 67.11 rPSD≥16(°) 0.705 <0.001* 0.651~0.754 66.87 65.13 rPHB≥50(°) 0.711 <0.001* 0.658~0.760 59.64 71.05 灌注 0.781* <0.001* 0.731~0.825 78.92 68.42 功能 0.756* <0.001* 0.705~0.802 75.3 64.50 同步性 0.723* <0.001* 0.670~0.771 66.3 67.80 联合 0.816 <0.001* 0.769~0.857 83.73 65.79 *P < 0.05。
下载: 导出CSV
表 4 三支组和非三支组患者负荷与静息GMPI指标的比较[M(P25,P75)]
Table 4. Comparison of patients' stress and rest GMPI indexes between three-vessel group and non-three-vessel group [M(P25,P75)]
项目 负荷GMPI 静息GPMI 检验值(Z) P 三支组 LVEF(%) 52(26,61) 53(32,62) 4.357 <0.001* LVEDV(mL) 115(87,162) 108(82,155) 5.474 <0.001* LVESV(mL) 56(35,116) 50(32,109) 7.631 <0.001* SV(mL) 49(38,61) 49(38,60) 0.896 0.370 PSD(°) 27.6(19.4,56.7) 20.3(13.8,47.2) 6.567 <0.001* PHB(°) 82.0(56.0,172) 56.5(42.0,137.0) 6.879 <0.001* 非三支组 LVEF(%) 63(56,68) 64(57,69) 1.456 0.146 LVEDV(mL) 88(73,110) 82(70,106) 6.107 <0.001* LVESV(mL) 32(23,46) 29(22,44) 5.744 <0.001* SV(mL) 53(44,61) 51(44,58) 3.707 <0.001* PSD(°) 17.5(13.1,26.0) 13.8(10.6 ,19.2) 5.695 <0.001* PHB(°) 53.0(39.0,72.5) 41.0(33.0,55.0) 7.076 <0.001*
下载: 导出CSV
表 5 三支病变与非三支病变组GMPI参数负荷较静息的变化量比较[M(P25,P75)]
Table 5. Comparison of GMPI parameter stress changes between three-vessel disease group and non-three-vessel disease group compared to rest [M(P25,P75)]
项目 三支病变组(166例) 非三支病变组(152例) 检验值 P ΔLVEF(%) −2.64 ± 7.24 −0.64 ± 5.51 2.777a 0.006 ΔLVEDV(mL) 6.5(−3,19.0) 5.0(−1.0,13.0) 0.931b 0.352 ΔLVESV(mL) 5.0(1.0,14.0) 3.0(−1.0,6.0) 3.793b <0.001* ΔSV(mL) 2.0(−7.0,10.0) 3.0(−2.0,8.5) 1.305b 0.192 ΔPSD(°) 5.4(−0.5,12.2) 3.5(−1.3,10.3) 1.435b 0.151 ΔPHB(°) 16.5(0.0,63.0) 9.5(2.0,26.5) 1.666b 0.096 注:a为t值,b为Z值;*P < 0.05。
下载: 导出CSV
-
[1] 胡盛寿,高润霖,刘力生,等. 《中国心血管病报告2018》概要[J]. 中国循环杂志,2019,34(3):209-220. doi: 10.3969/j.issn.1000-3614.2019.03.001 [2] Jie L,Feng X X,Duan Y F,et al. Using machine learning to aid treatment decision and risk assessment for severe three-vessel coronary artery disease[J]. J Geriatr Cardiol,2022,19(5):367-376. [3] Glazier J J,Ramos-Parra B,Kaki A. Therapeutic options for left main,left main equivalent,and three-vessel disease[J]. International Journal of Angiology,2021,30(1):76-82. doi: 10.1055/s-0041-1723977 [4] Sirajuddin A,Mirmomen S M,Kligerman S J,et al. Ischemic heart disease: Noninvasive imaging techniques and findings[J]. Radiographics,2021,41(4):990-1021. doi: 10.1148/rg.2021200125 [5] Knuuti J,Wijns W,Saraste A,et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes[J]. Eur Heart J,2020,41(3):407-477. doi: 10.1093/eurheartj/ehz425 [6] Society of Nuclear Medicine of Chinese Medical A,Society of Cardiology of Chinese Medical A. [Guideline for the clinical use of myocardial radionuclide imaging (2018)][J]. Zhonghua Xin Xue Guan Bing Za Zhi,2019,47(7):519-527. [7] Schlattmann P,Wieske V,Bressem K K,et al. The effectiveness of coronary computed tomography angiography and functional testing for the diagnosis of obstructive coronary artery disease: Results from the individual patient data Collaborative Meta-Analysis of Cardiac CT (COME-CCT)[J]. Insights Imaging,2024,15(1):208. doi: 10.1186/s13244-024-01702-y [8] Gulati M,Levy P D,Mukherjee D,et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [J]. Circulation,2021,144(22):455. [9] Herner M,Agasthi P. Cardiac Stress Imaging [M]. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Pradyumna Agasthi declares no relevant financial relationships with ineligible companies. StatPearls Publishing Copyright © 2024,StatPearls Publishing LLC. 2024. [10] Gopal S,Murphy C. Nuclear Medicine Stress Test [M]. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Christie Murphy declares no relevant financial relationships with ineligible companies. StatPearls Publishing Copyright © 2024,StatPearls Publishing LLC. 2024. [11] 中华医学会核医学分会,中华医学会心血管病学分会. 核素心肌显像临床应用指南(2018)[J]. 中华心血管病杂志,2019,47(7):519-527. [12] 中华医学会心血管病学分会介入心脏病学组,中华医学会心血管病学分会动脉粥样硬化与冠心病学组,中国医师协会心血管内科医师分会血栓防治专业委员会,et al. 稳定性冠心病诊断与治疗指南[J]. 中华心血管病杂志,2018,46(9):680-694. [13] Neumann F J,Sousa-Uva M,Ahlsson A,et al. 2018 ESC/EACTS Guidelines on myocardial revascularization[J]. Eur Heart J,2019,40(2):87-165. doi: 10.1093/eurheartj/ehy394 [14] 中华医学会心血管病学分会介入心脏病学组,中国医师协会心血管内科医师分会血栓防治专业委员会,中华心血管病杂志编辑委员会. 中国经皮冠状动脉介入治疗指南(2016)[J]. 中华心血管病杂志,2016,44(5):382-400. [15] Bax J J,Achenbach S,Valgimigli M,et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes[J]. European Heart Journal,2020,41(3):407-477. [16] Garcia-Cardenas M,Espejel-Guzman A,Antonio-Villa N E,et al. Diagnosis,performance and added value of assessing ventricular dyssynchrony by phase analysis in patients with three-vessel disease: A single-center cross-sectional study in Mexico[J]. J Nucl Cardiol,2023,30(3):1219-1229. doi: 10.1007/s12350-022-03136-9 [17] Gimelli A,Liga R,Duce V,et al. Accuracy of myocardial perfusion imaging in detecting multivessel coronary artery disease: A cardiac CZT study[J]. J Nucl Cardiol,2017,24(2):687-695. doi: 10.1007/s12350-015-0360-8 [18] Hida S,Chikamori T,Tanaka H,et al. Diagnostic value of left ventricular dyssynchrony after exercise and at rest in the detection of multivessel coronary artery disease on single-photon emission computed tomography[J]. Circ J,2012,76(8):1942-1952. doi: 10.1253/circj.CJ-11-1392 [19] Patel J J,Alzahrani T. Myocardial Perfusion Scan [M]. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Talal Alzahrani declares no relevant financial relationships with ineligible companies. StatPearls Publishing Copyright © 2024,StatPearls Publishing LLC. 2024. [20] Alexánderson-Rosas E,Hernández-Sandoval S. Gated SPECT beyond myocardial perfusion: Assessment of mechanical left ventricular synchrony[J]. J Nucl Cardiol,2022,29(3):975-977. doi: 10.1007/s12350-020-02518-1 [21] Khidir M J,Delgado V,Ajmone Marsan N,et al. Mechanical dyssynchrony in patients with heart failure and reduced ejection fraction: How to measure?[J]. Curr Opin Cardiol,2016,31(5):523-530. doi: 10.1097/HCO.0000000000000314 [22] Lima R S L,Watson D D,Goode A R,et al. Incremental value of combined perfusion and function over perfusion alone by gated SPECT myocardial perfusion imaging for detection of severe three-vessel coronary artery disease[J]. Journal of the American College of Cardiology,2003,42(1):64-70. doi: 10.1016/S0735-1097(03)00562-X [23] Camilletti J,Erriest J,Espinola-Zavaleta N,et al. Left ventricular dyssynchrony and abnormalities in wall motion,assessed by gated-SPECT as ischemic auxiliary markers[J]. Journal of Nuclear Cardiology,2018,27(6):2261-2268. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 362
- HTML全文浏览量: 206
- PDF下载量: 11
- 被引次数: 0
