

Risk Factor Analysis and Predictive Model Construction for Thrombohemorrhagic Events in Patients with Acute Promyelocytic Leukemia
-
摘要:
目的 分析急性早幼粒细胞白血病(acute promyelocytic leukemia,APL)患者血栓出血性事件发生的危险因素,并构建预测模型。 方法 回顾性分析2020年5月—2023年12月四川大学华西医院收治的275例以出血首发表现的APL患者,按3∶2的比例随机将患者分为训练集(n = 165)和验证集(n = 110),另根据患者是否为发生血栓出血性事件将训练集分为血栓出血组和非血栓出血组。采用多因素Logistic回归筛选APL患者发生血栓出血性事件的相关影响因素,并构建列线图预测模型。 结果 275例APL患者中共有75例发生血栓出血性事件,发生率为27.27%;血栓出血组白细胞计数(white blood cell count,WBC)>10×109/L、纤维蛋白原(fibrinogen,FIB)<1.5 g/L、骨髓早幼粒细胞占比>60%占比、凝血酶原时间(prothrombin time,PT)、乳酸脱氢酶(lactate dehydrogenase,LDH)、D-二聚体水平均高于非血栓出血组(P < 0.05);多因素Logistic分析显示,WBC>10×109/L、骨髓早幼粒细胞占比>60%、LDH、D-二聚体水平升高均为APL患者发生血栓出血性事件的危险因素(P < 0.05);ROC曲线显示,模型在训练集、验证集中预测患者发生血栓出血性事件的AUC分别为0.756(95%CI:0.662~0.835)、0.833(95%CI:0.746~0.899);Bootstrap法重复抽样 1000 次进行内部验证,训练集和验证集的Hosmer-Lemeshow检验结果(P > 0.05),两组拟合度均良好;DCA结果显示,模型预测血栓出血性事件的净获益区间均较大。结论 WBC、骨髓早幼粒细胞占比、LDH、D-二聚体水平均为APL患者发生血栓出血性事件的危险因素,基于上述指标建立的模型预测效能良好。 -
关键词:
- 急性早幼粒细胞白血病 /
- 血栓性出血 /
- 危险因素 /
- 预测模型
Abstract:Objectiv To analyze the risk factors of thrombohemorrhagic events in patients with acute promyelocytic leukemia (APL) and to establish a risk prediction model. Methods 275 APL patients initially presenting with bleeding symptoms, admitted to West China Hospital of Sichuan University between May 2020 and December 2023 were retrospectively analyzed, and the patients were randomly divided into a training set (n = 165) and a validation set (n = 110) in a ratio of 3∶2. Patients in the training set were further categorized into a thrombotic hemorrhage group and a non-thrombotic hemorrhage group based on the occurrence of thrombohemorrhagic events. Multivariate logistic regression was used to identify factors associated with thrombohemorrhagic events, and a nomogram-based predictive model was constructed. Receiver Operating characteristic (ROC) curve, calibration diagram and decision curve analysis (DCA) were drawn to evaluate and verify the model. Result Among the 275 APL patients, 75 experienced thrombotic bleeding events, yielding an incidence rate of 27.27%. Compared with the non-thrombohemorrhagic group, the thrombohemorrhagic group had higher proportions of patients with white blood cell count (WBC) > 10×109/L, fibrinogen (FIB) < 1.5 g/L, the proportion of bone marrow promyelocytes > 60%, as well as higher levels of prothrombin time (PT), lactate dehydrogenase (LDH), and D-dimer (P < 0.05). Multivariate logistic regression showed that WBC > 10×109/L, the proportion of promyelocytes in bone marrow > 60%, increased LDH and D-dimer levels were risk factors for thrombotic and hemorrhagic events in APL patients (P < 0.05). The ROC curve analysis results showed that the model predicted thrombohemorrhagic events with an AUC of 0.756 (95%CI: 0.662~0.835) in the training set and 0.833 (95%CI: 0.746~0.899) in the validation set. Internal validation using 1, 000 bootstrap resampling yielded Hosmer-Lemeshow test P > 0.05 for both sets, indicating good calibration. Decision curve analysis (DCA) showed a favorable net benefit across a wide range of threshold probabilities. Conclusion WBC proportion, LDH and D-dimer risk factors for thrombotic and hemorrhagic events in APL patients. The model based on these indicators good predictive efficiency. -
Key words:
- Acute promyelocytic leukemia /
- Thrombus bleeding /
- Risk factors /
- Predictive model
-
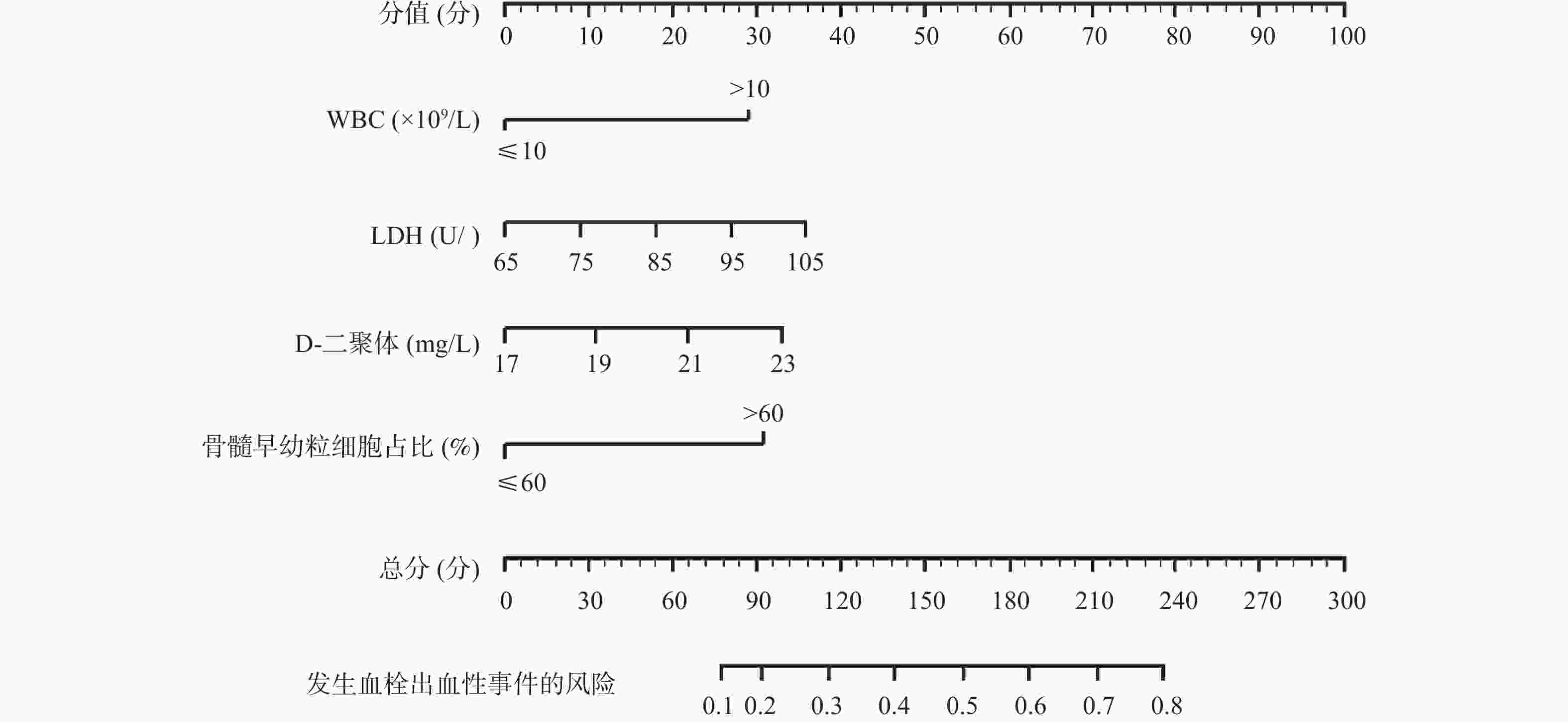
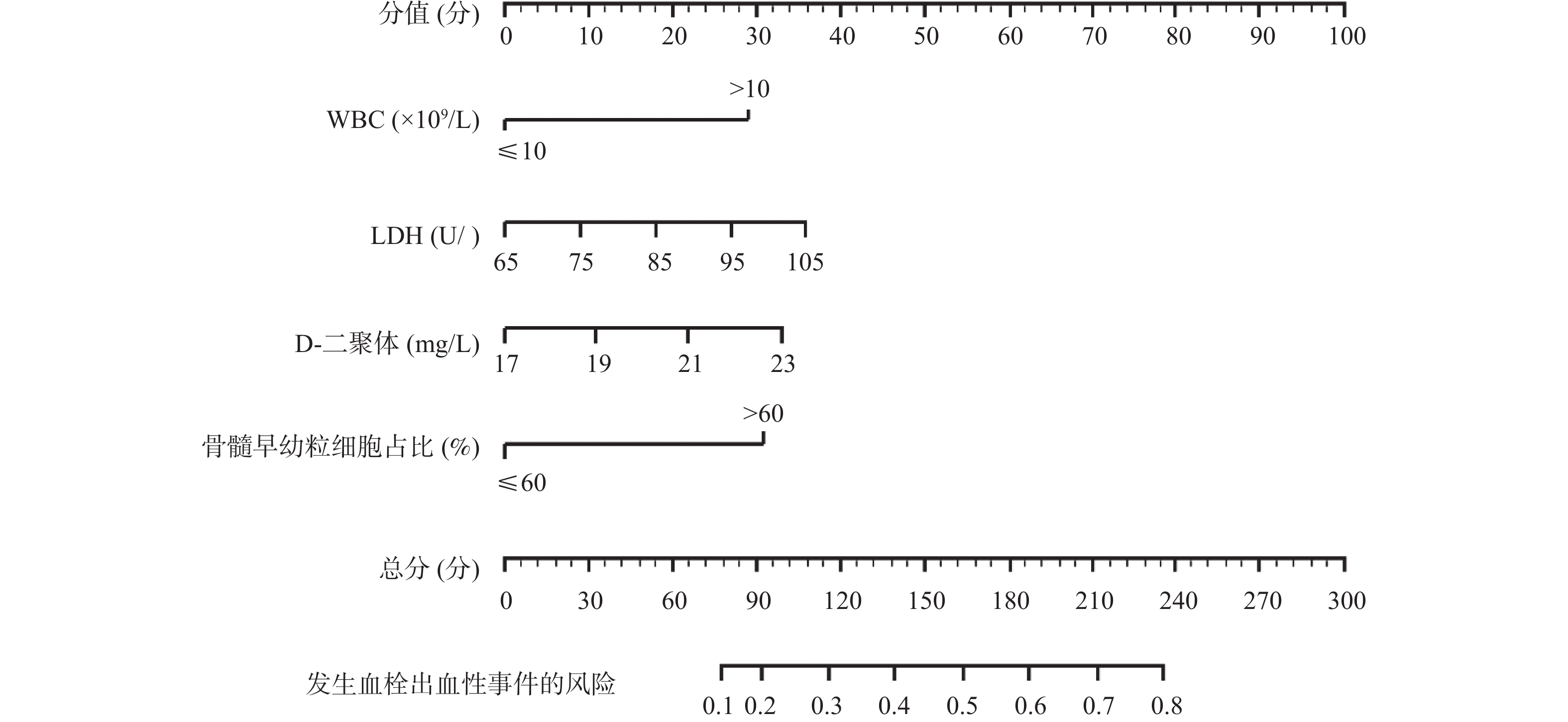
图 1 APL患者发生血栓出血性事件的列线图预测模型
Figure 1. A Nomogram predictive model for thrombohemorrhagic events in APL patients
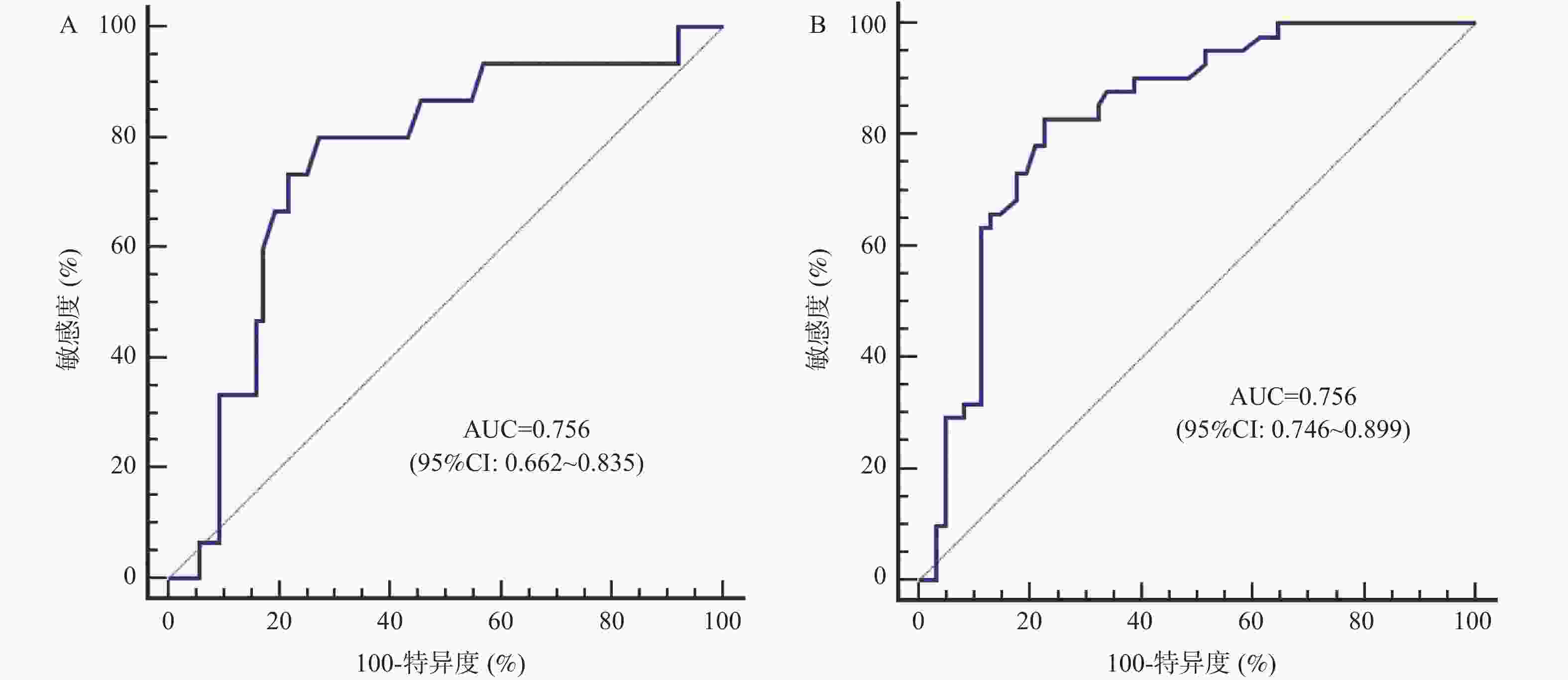
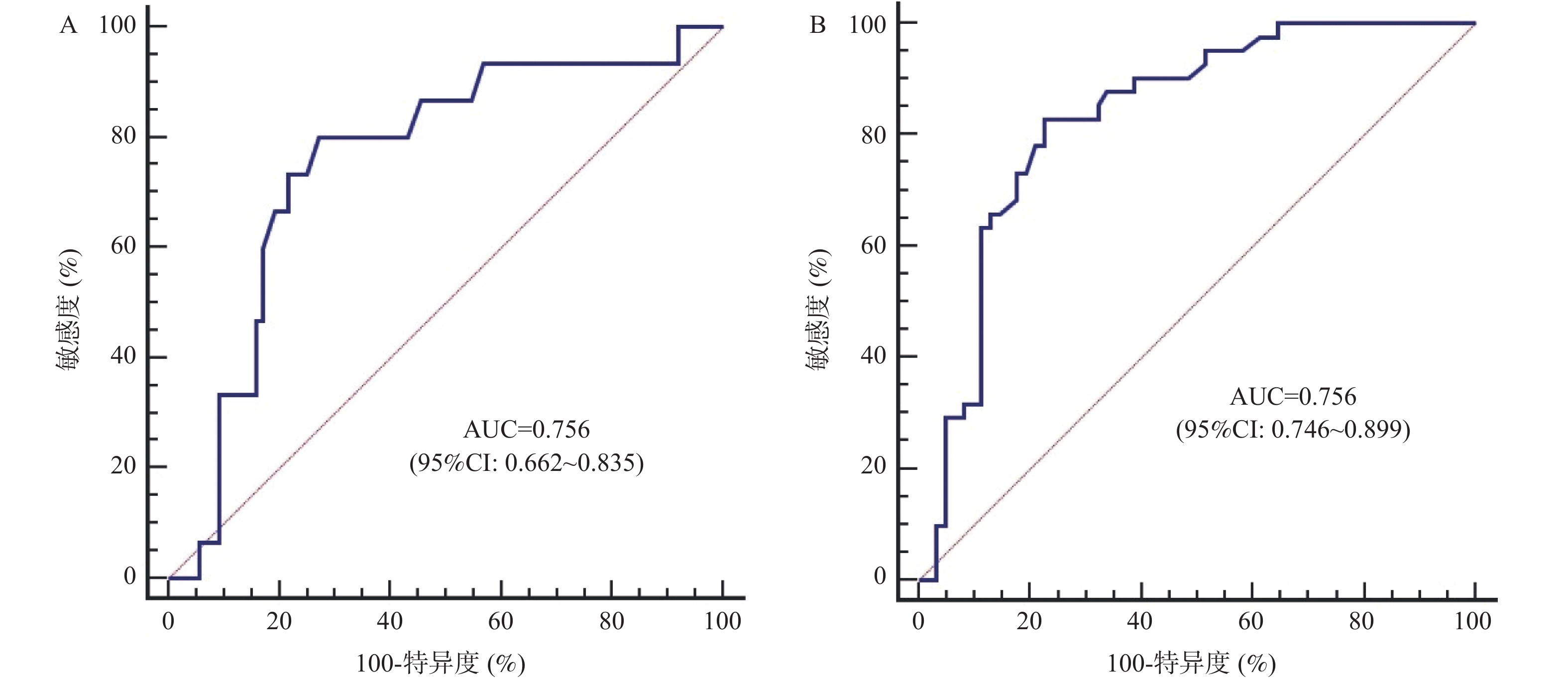
图 2 模型预测患者发生血栓出血性事件的ROC曲线
A:训练集;B:验证集。
Figure 2. ROC curve of the model for predicting thrombohemorrhagic events
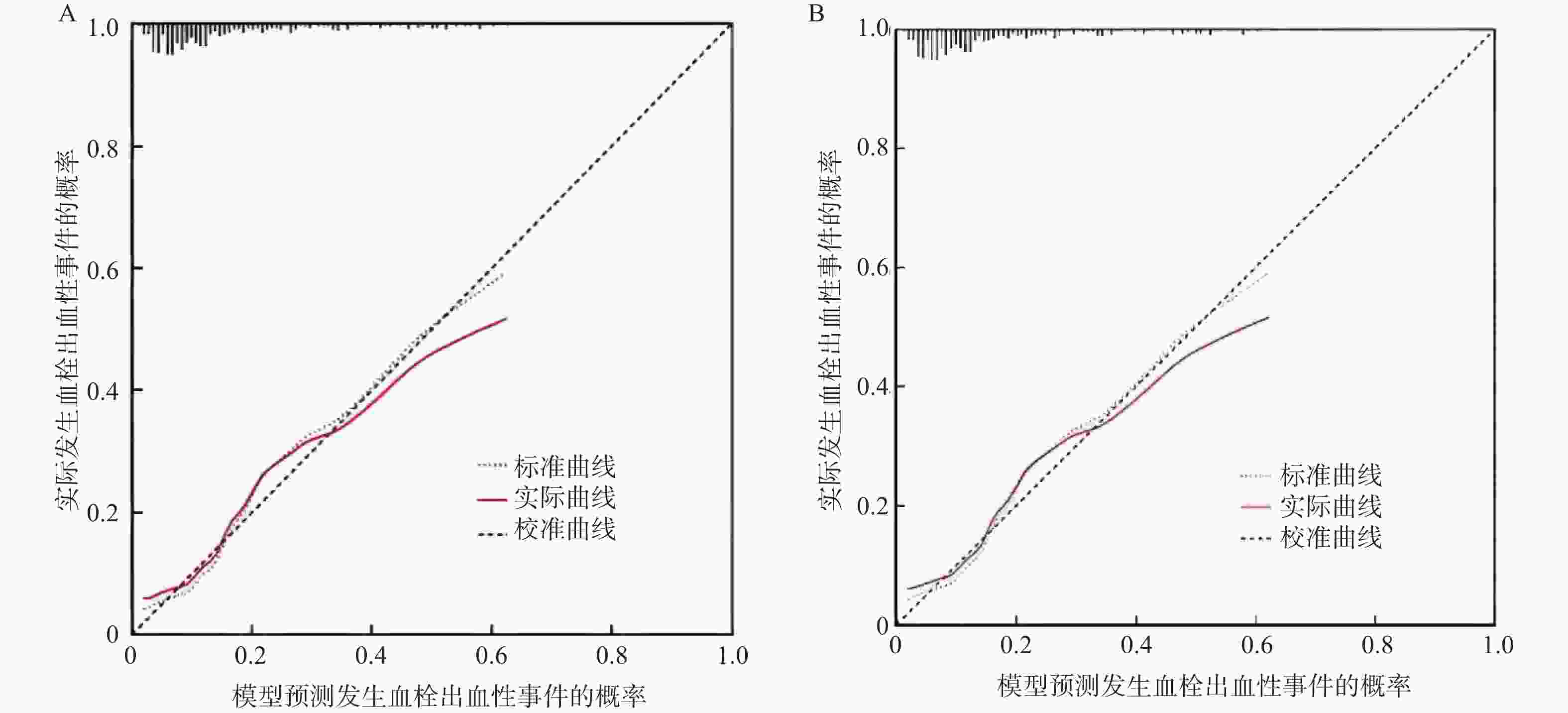
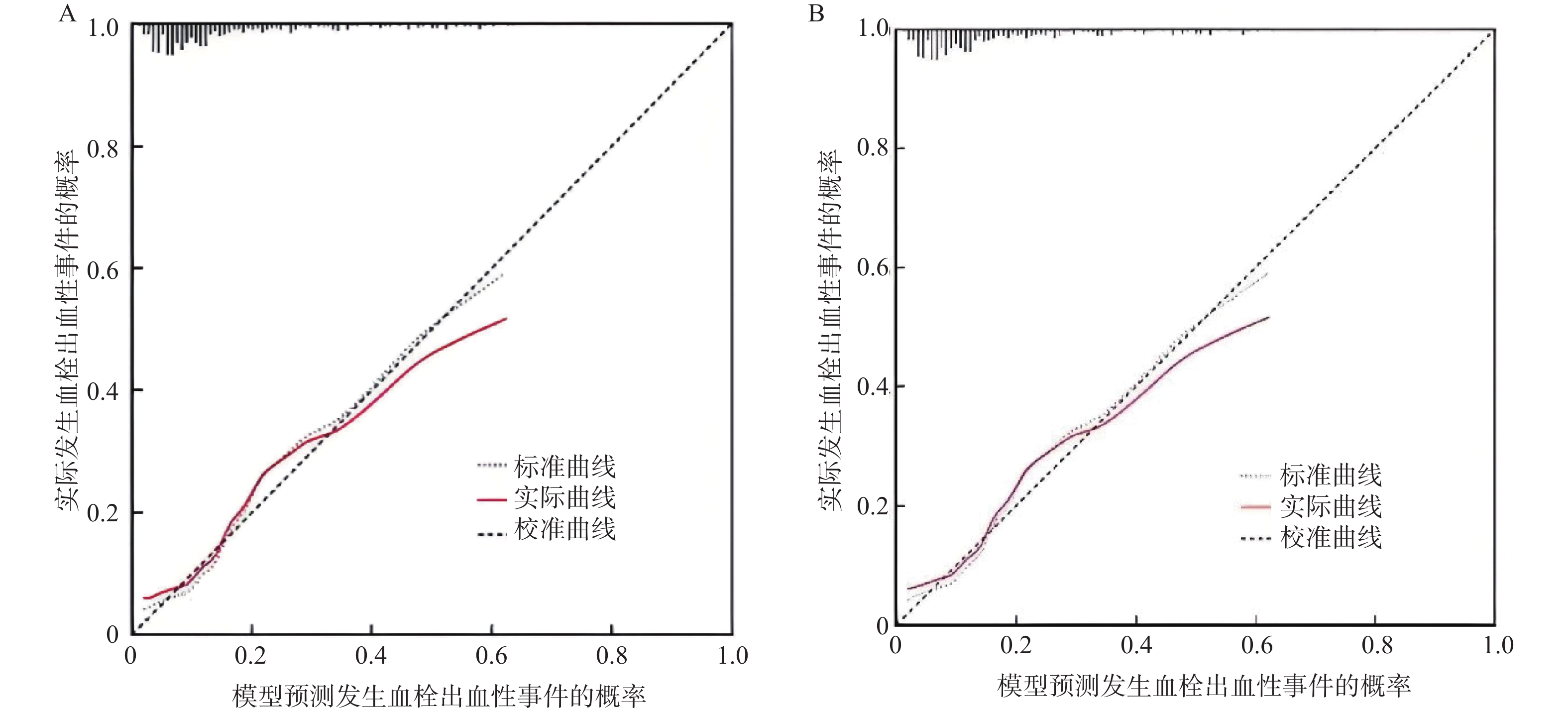
图 3 模型预测发生血栓出血性事件的校准曲线
A:训练集;B:验证集。
Figure 3. Calibration curve of the model for predicting thrombohemorrhagic events
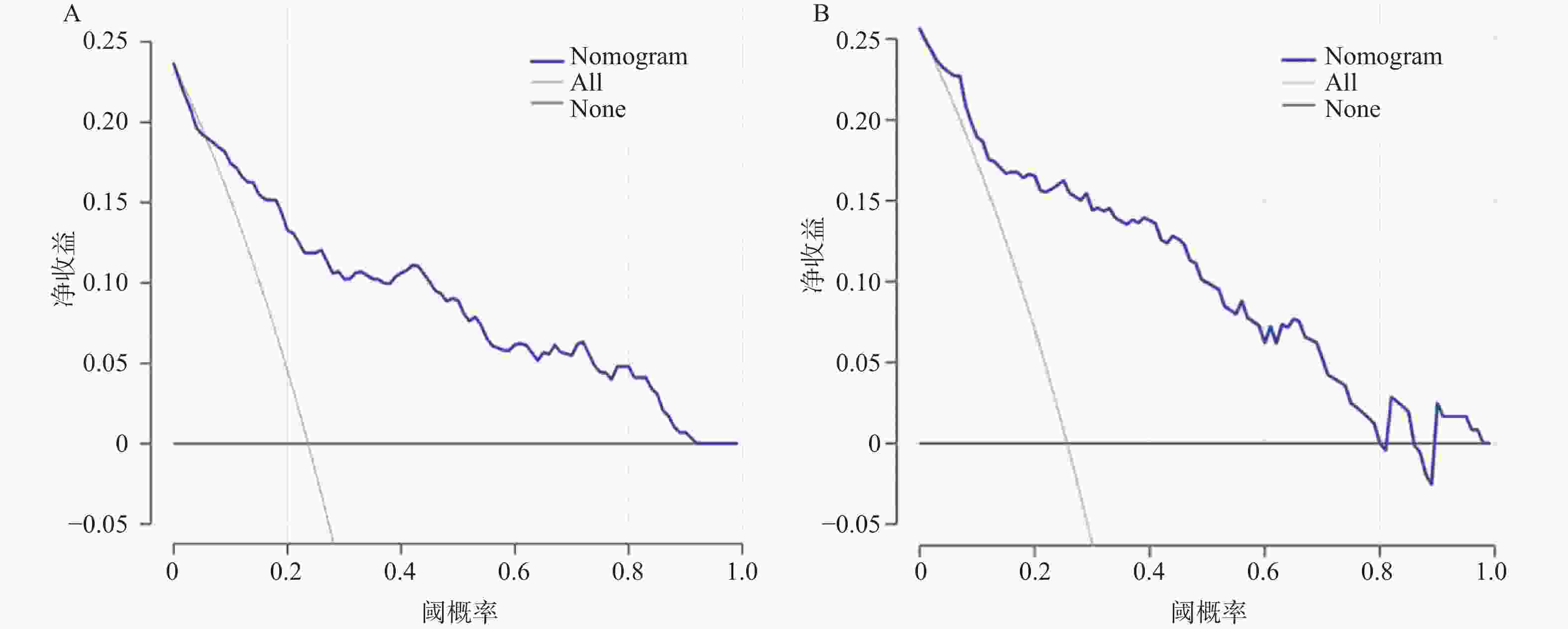
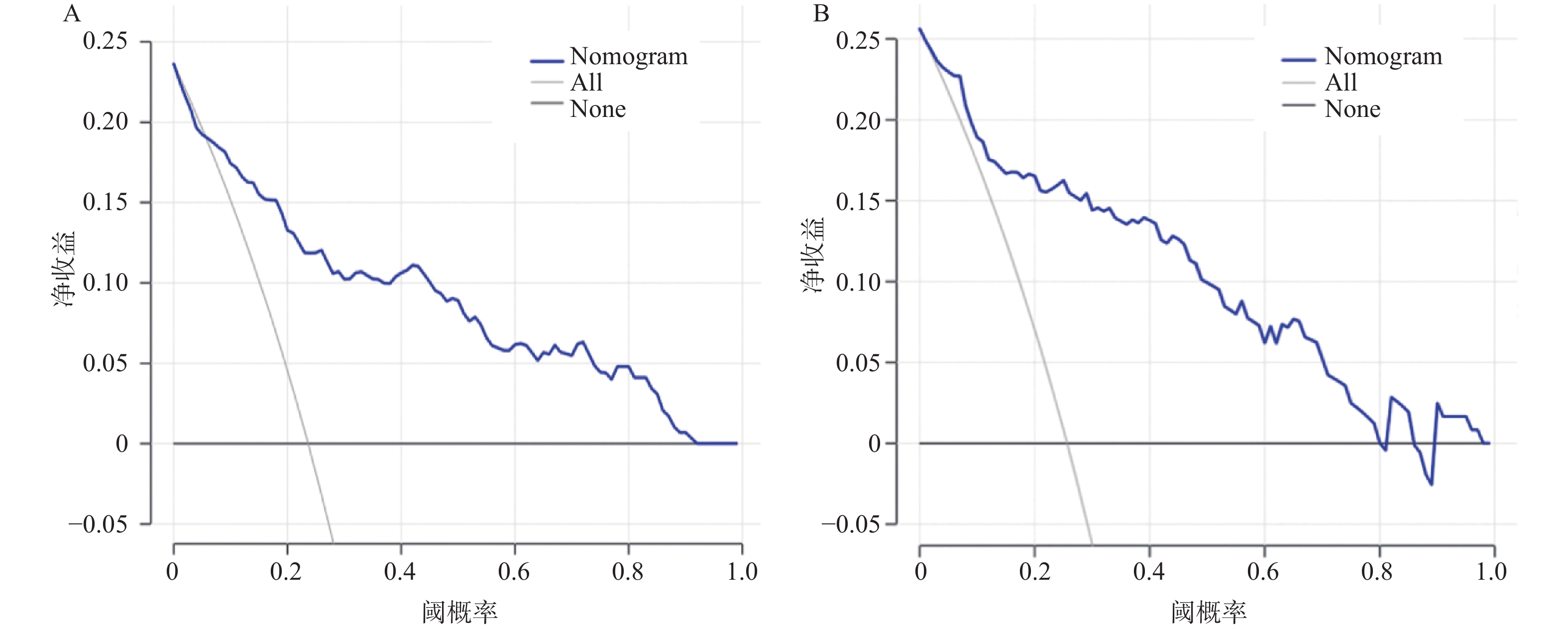
图 4 模型预测发生血栓出血性事件的DCA曲线
A:训练集;B:验证集。
Figure 4. DCA curve of the model for predicting the occurrence of thrombohemorrhagic events
表 1 训练集与验证集临床资料比较[($ \bar x \pm s $)/n(%)]
Table 1. Comparison of clinical characteristics between the training set and validation set [($ \bar x \pm s $)/n(%)]
参数 训练集(n = 165) 验证集(n = 110) t/χ2 P 性别 0.786 0.375 男 81(49.09) 60(54.55) 女 84(50.91) 50(45.45) 年龄(岁) 33.27 ± 5.23 32.17 ± 5.42 1.684 0.093 饮酒史 0.183 0.669 是 52(31.52) 32(29.09) 否 113(68.48) 78(70.91) 吸烟史 0.145 0.703 是 46(27.88) 33(30.00) 否 119(72.12) 77(70.00) WBC 2.528 0.112 >10×109/L 65(39.39) 54(49.09) ≤10×109/L 100(60.61) 56(50.91) PLT 1.578 0.209 >30×109/L 104(63.03) 61(55.45) ≤30×109/L 61(36.97) 49(44.55) PT(s) 13.23 ± 2.12 13.64 ± 2.10 1.577 0.116 APTT(s) 3.19 ± 0.62 3.06 ± 0.65 1.671 0.096 FIB 0.706 0.410 <1.5 g/L 86(52.12) 63(57.27) ≥1.5 g/L 79(47.88) 47(42.73) LDH(U/L) 72.55 ± 12.28 71.75 ± 12.31 0.529 0.597 D-二聚体(mg/L) 17.94 ± 3.42 18.18 ± 3.26 0.581 0.562 SCr(μmol/L) 89.77 ± 13.65 89.43 ± 13.50 0.203 0.839 骨髓早幼粒细胞占比(%) 0.706 0.401 >60 86(52.12) 63(57.27) ≤60 79(47.88) 47(42.73)  下载: 导出CSV
下载: 导出CSV
表 2 血栓出血组和非血栓出血组临床资料比较[($ \bar x \pm s $)/n(%)]
Table 2. Comparison of clinical characteristics between the thrombosis-bloeding group and the non-thrombosis-bloeding group [($ \bar x \pm s $)/n(%)]
参数 非血栓出血组(n = 123) 血栓出血组(n = 42) t/$ {\chi }^{2} $ P 性别 0.725 0.395 男 58(47.15) 23(54.76) 女 65(52.85) 19(45.24) 年龄(岁) 33.62 ± 5.81 32.23 ± 5.60 1.351 0.179 饮酒史 0.740 0.390 是 41(33.33) 11(26.19) 否 82(66.67) 31(73.81) 吸烟史 0.464 0.496 是 36(29.27) 10(23.81) 否 87(70.73) 32(76.19) WBC 17.553 <0.001* >10×109/L 37(30.08) 28(66.67) ≤10×109/L 86(69.92) 14(33.33) PLT 2.742 0.098 >30×109/L 82(66.67) 22(52.38) ≤30×109/L 41(33.33) 20(47.62) PT(s) 12.37 ± 2.19 15.74 ± 2.60 8.198 <0.001* APTT(s) 3.24 ± 0.75 3.05 ± 0.69 1.446 0.150 FIB 10.620 0.001* <1.5 g/L 55(44.72) 31(73.81) ≥1.5 g/L 68(55.28) 11(26.19) LDH(U/L) 62.07 ± 10.58 103.25 ± 16.91 18.466 <0.001* D-二聚体(mg/L) 16.54 ± 3.31 22.05 ± 4.77 8.263 <0.001* SCr(μmol/L) 90.91 ± 16.73 86.45 ± 13.22 1.568 0.119 骨髓早幼粒细胞占比(%) 4.777 0.029* >60 58(47.15) 28(66.67) ≤60 65(55.85) 14(33.33) *P < 0.05。
下载: 导出CSV
表 3 APL患者发生血栓出血性事件的多因素回归分析
Table 3. Multivariate regression analysis of thrombohemorrhagic events in APL patients
因素 B S.E. Wald OR 95%CI P WBC>10×109/L 0.719 0.248 8.401 2.052 1.262~3.336 0.004* LDH 1.115 0.415 7.186 3.050 1.350~6.893 0.007* D-二聚体 0.962 0.302 10.148 2.617 1.448~4.730 0.001* 骨髓早幼粒细胞占比>60% 0.802 0.283 8.031 2.230 1.281~3.883 0.005* 常数 −0.387 0.103 14.117 *P < 0.05。
下载: 导出CSV
-
[1] Hermsen J, Hambley B. The coagulopathy of acute promyelocytic leukemia: An updated review of pathophysiology, risk stratification, and clinical management[J]. Cancers, 2023, 15(13): 3477. doi: 10.3390/cancers15133477 [2] Ferrara F, Molica M, Bernardi M. Drug treatment options for acute promyelocytic leukemia[J]. Expert Opin Pharmacother, 2022, 23(1): 117-127. doi: 10.1080/14656566.2021.1961744 [3] Sabljic N, Thachil J, Pantic N, et al. Hemorrhage in acute promyelocytic leukemia—fibrinolysis in focus[J]. Res Pract Thromb Haemost, 2024, 8(5): 102499. [4] Zhang Q, Huang M J, Wang H Y, et al. A novel prognostic nomogram for adult acute lymphoblastic leukemia: A comprehensive analysis of 321 patients[J]. Ann Hematol, 2023, 102(7): 1825-1835. [5] Mitrovic M, Pantic N, Bukumiric Z, et al. Venous thromboembolism in patients with acute myeloid leukemia: Development of a predictive model[J]. Thromb J, 2024, 22(1): 37. [6] Song X, Chi C, Gao W, et al. Biochemical risk factors and outcomes of acute promyelocytic leukemia patients with thrombotic events: A matched pair analysis[J]. J Thromb Thrombolysis, 2024, 57(5): 828-841. [7] 中华医学会血液学分会, 中国医师协会血液科医师分会. 中国急性早幼粒细胞白血病诊疗指南(2018年版)[J]. 中华血液学杂志, 2018, 39(3): 179-183. [8] Peddi K, Wiggins B, Choudhury O, et al. Intracranial hemorrhage secondary to newly diagnosed acute promyelocytic leukemia: A cautionary tale[J]. Cureus, 2022, 14(3): e23252. [9] Wang H Y, Gong S, Li G H, et al. An effective and chemotherapy-free strategy of all-trans retinoic acid and arsenic trioxide for acute promyelocytic leukemia in all risk groups (APL15 trial)[J]. Blood Cancer J, 2022, 12: 158. [10] Bercier P, de Thé H. History of developing acute promyelocytic leukemia treatment and role of promyelocytic leukemia bodies[J]. Cancers, 2024, 16(7): 1351. [11] Heestermans M, Poenou G, Hamzeh-Cognasse H, et al. Anticoagulants: A short history, their mechanism of action, pharmacology, and indications[J]. Cells, 2022, 11(20): 3214. [12] Wang C, Wang Y, Zuo N, et al. CD44-fibrinogen binding promotes bleeding in acute promyelocytic leukemia by in situ fibrin(ogen) deposition[J]. Blood Adv, 2022, 6(15): 4617-4633. [13] Ono M, Tomaniak M, Koenig W, et al. Impact of white blood cell count on clinical outcomes in patients treated with aspirin-free ticagrelor monotherapy after percutaneous coronary intervention: Insights from the GLOBAL LEADERS trial[J]. Eur Heart J Cardiovasc Pharmacother, 2022, 8(1): 39-47. [14] Foy B H, Sundt T M, Carlson J C T, et al. Human acute inflammatory recovery is defined by co-regulatory dynamics of white blood cell and platelet populations[J]. Nat Commun, 2022, 13: 4705. [15] Xiao M, Zhou P, Liu Y, et al. Predictive factors for differentiating thrombohemorrhagic disorders in high-risk acute promyelocytic leukemia[J]. Thromb Res, 2022, 210: 33-41. [16] Wang Y, Wang C, Zuo N, et al. Extracellular traps increase burden of bleeding by damaging endothelial cell in acute promyelocytic leukaemia[J]. Front Immunol, 2022, 13: 841445. [17] Odetola O, Tallman M S. How to avoid early mortality in acute promyelocytic leukemia[J]. Hematology, 2023, 2023(1): 248-253. [18] 姚强华, 王颖超, 王叨, 等. 儿童急性早幼粒细胞白血病并发血栓四例并文献复习[J]. 中华儿科杂志, 2021, 59(5): 407-411. [19] Zhang J Y, Yan Z S, Sun X J, et al. Association between serum lactate dehydrogenase level and 30-day mortality in patients with intracranial hemorrhage with acute leukemia in the induction phase: A cohort study[J]. Glob Med Genet, 2024, 11(2): 142-149. [20] Anderson D R, Stock W, Karrison T G, et al. D-dimer and risk for thrombosis in adults with newly diagnosed acute lymphoblastic leukemia[J]. Blood Adv, 2022, 6(17): 5146-5151. [21] Owattanapanich W, Rungjirajittranon T, Jantataeme A, et al. Simplified predictive scores for thrombosis and bleeding complications in newly diagnosed acute leukemia patients[J]. Thromb J, 2023, 21(1): 65. [22] Guo Y, Niu Y, Liang H, et al. A nomogram based on clinical features and molecular abnormalities for predicting the prognosis of patients with acute myeloid leukemia[J]. Transl Cancer Res, 2023, 12(12): 3432-3442. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 100
- HTML全文浏览量: 106
- PDF下载量: 64
- 被引次数: 0
