

Correlation and Predictive Value of Serum Chemerin,SDF-1α,and MiR-21 with Adjacent Vertebral Re-fracture after Thoracolumbar Fracture Surgery in Elderly Patients
-
摘要:
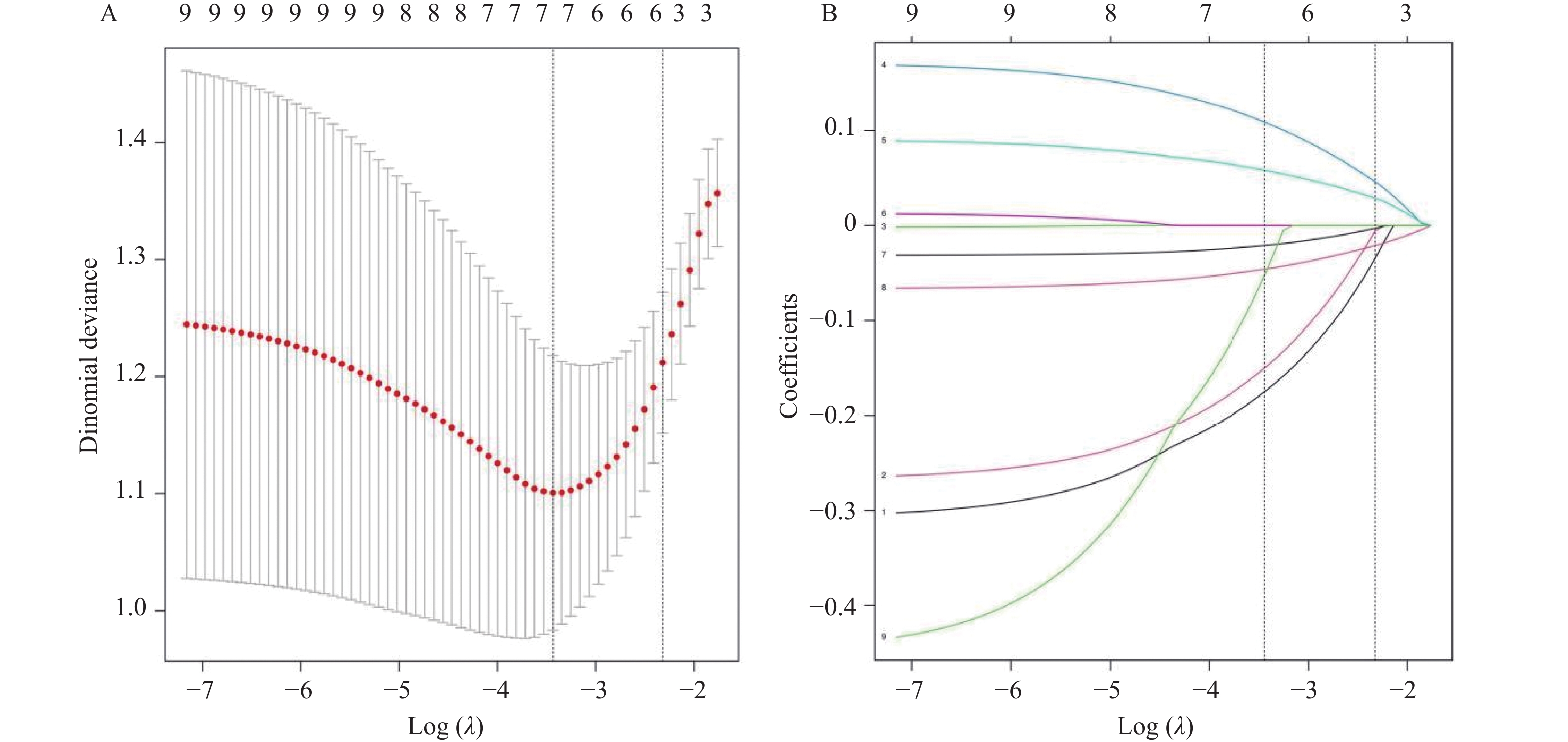
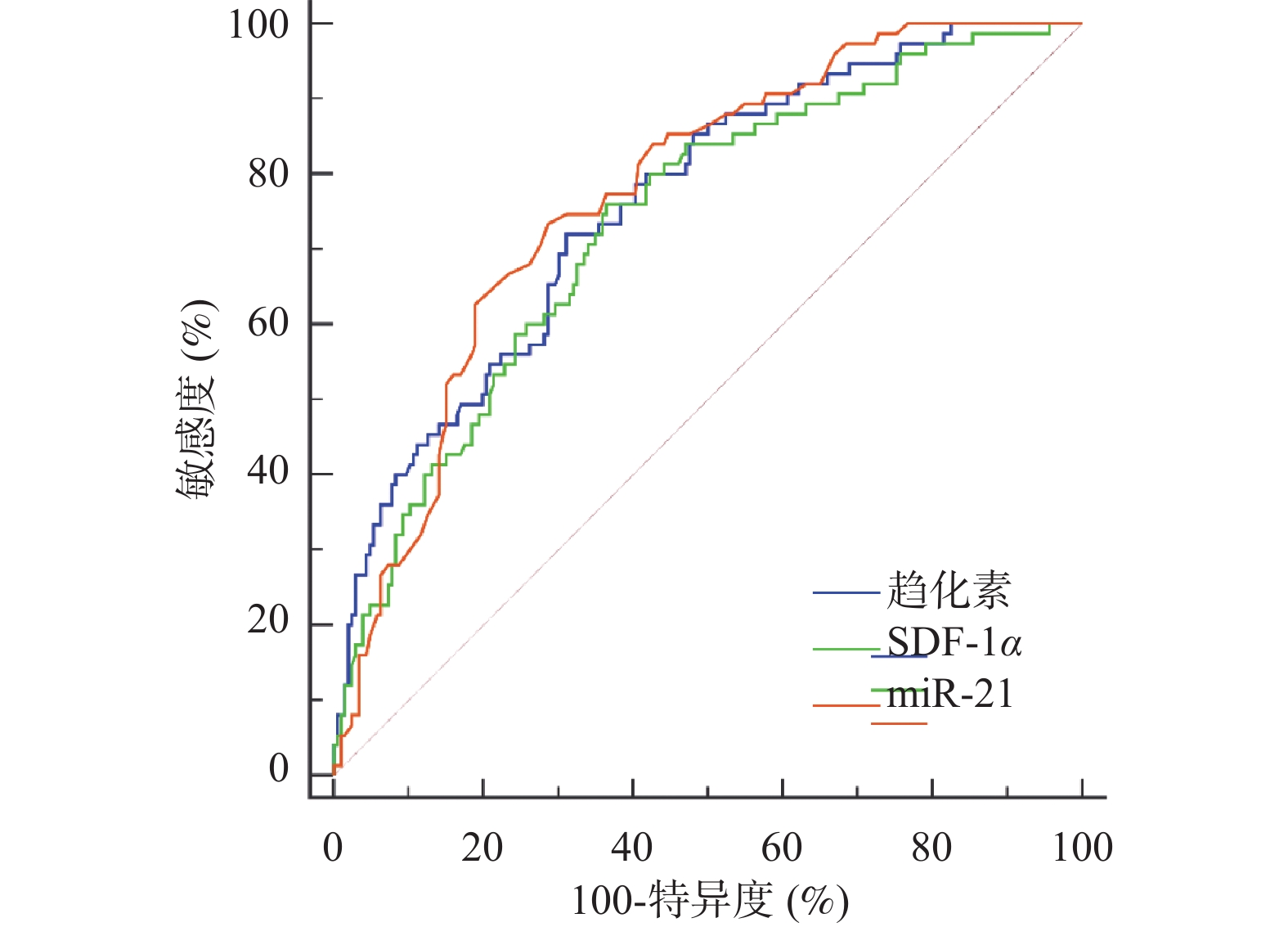
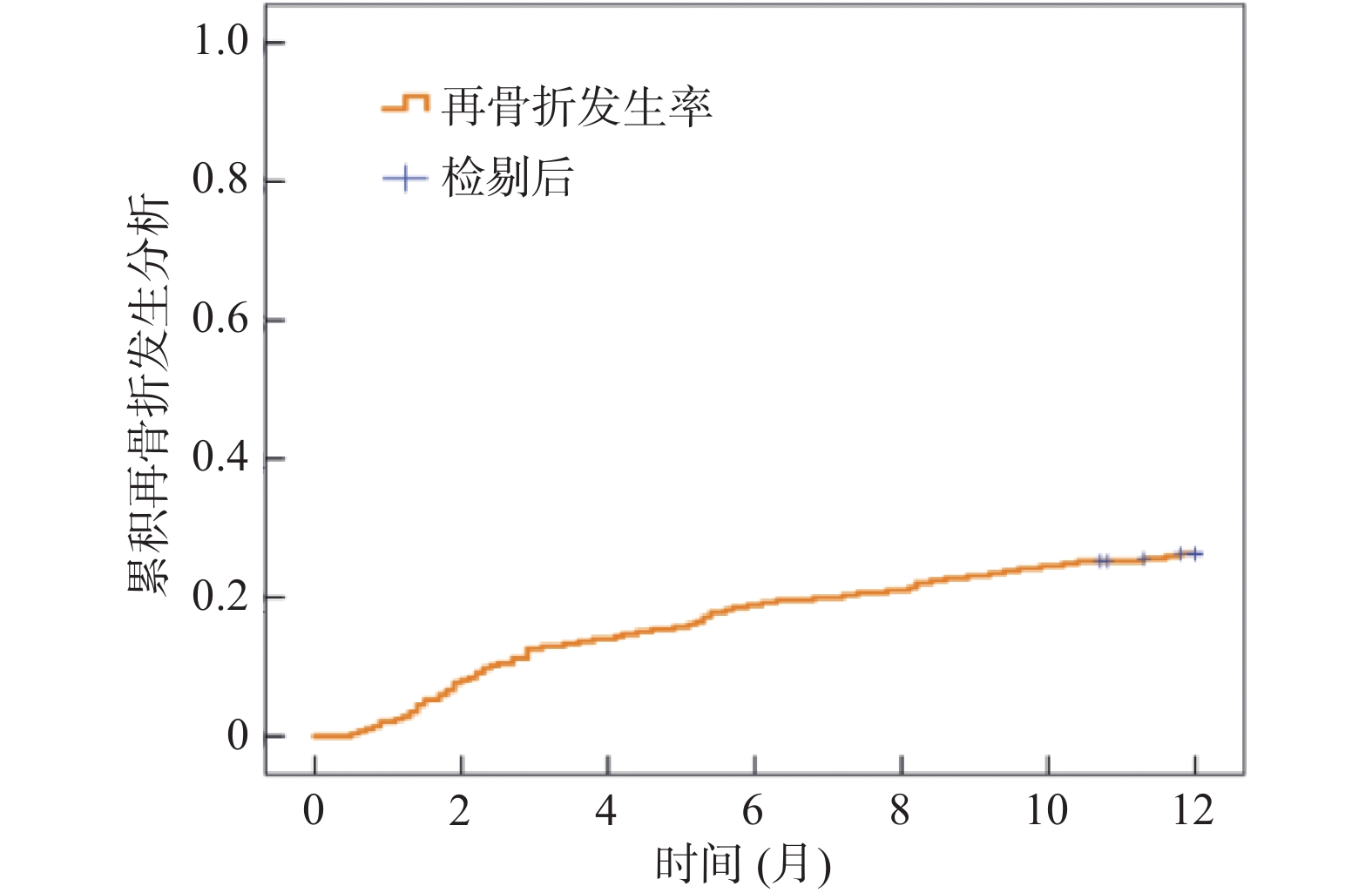
目的 探讨血清趋化素、基质细胞衍生因子1α(stromal cell-derived factor 1α,SDF-1α)和微小核酸核糖-21(micro ribonucleic acid-21,miR-21)与老年胸腰椎骨折术后邻近椎体再骨折的相关性,并探讨三者的预测价值。 方法 选取晋城市人民医院2021年9月至2024年9月285例老年胸腰椎骨折患者作为研究对象,均行经皮椎体成形术(percutaneous vertebroplasty,PVP)或经皮球囊扩张椎体后凸成形术(percutaneous kyphoplasty,PKP)治疗,随访12个月,根据是否发生邻近椎体再骨折分为再骨折组与非再骨折组,比较两组临床资料、血清趋化素、SDF-1α、miR-21水平,评价血清趋化素、SDF-1α、miR-21对术后邻近椎体再骨折的预测价值。 结果 本研究281例老年胸腰椎骨折患者随访12个月,失访4例,邻近椎体再骨折发生率为26.69%(75/281)。再骨折组血清趋化素、SDF-1α水平高于非再骨折组,miR-21水平低于非再骨折组(P < 0.05);Lasso-Logistic回归分析,骨密度、骨水泥外渗、术后椎体高度恢复率、术后Cobb角、血清趋化素、SDF-1α、miR-21是老年胸腰椎骨折术后邻近椎体再骨折的独立影响因素(P < 0.05);受试者工作特征(receiver operating characteristic,ROC)曲线分析,血清趋化素、SDF-1α、miR-21预测邻近椎体再骨折的曲线下面积(area under the curve,AUC)为0.761(95%CI:0.706~0.809)、0.736(95%CI:0.681~0.787)、0.773(95%CI:0.719~0.820);血清趋化素、SDF-1α、miR-21与临床指标联合预测邻近椎体再骨折的AUC为0.934(95%CI:0.898~0.960);10折交叉验证显示,平均AUC为0.926(95%CI:0.892~0.955),各折AUC范围为0.911~0.942;校正曲线显示,该预测模型的校准度良好(Hosmer-Lemeshow检验P > 0.05)。 结论 血清趋化素,SDF-1α和miR-21与老年胸腰椎骨折术后邻近椎体再骨折独立相关,联合检测可有效预测邻近椎体再骨折风险。 Abstract:Objective To investigate the correlation between serum chemokines, stromal cell-derived factor 1α (SDF-1α) and micro ribonucleic acid-21 (miR-21) and adjacent vertebral re-fracture after thoracolumbar fracture surgery in the elderly, and to explore the predictive value of the three. Methods A total of 285 elderly patients with thoracolumbar fractures in Jincheng People's Hospital from September 2021 to September 2024 were selected as the study subjects. All patients underwent percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP), and they were followed up for 12 months. According to the occurrence of adjacent vertebral re-fracture, they were divided into re-fracture group and non-re-fracture group. The clinical data, serum chemerins, SDF-1α and miR-21 levels were compared between the two groups, and the predictive value of serum chemerins, SDF-1α and miR-21 for postoperative adjacent vertebral re-fracture was evaluated. Results In this study, 281 elderly patients with thoracolumbar fractures were followed up for 12 months, and 4 patients were lost to follow-up. The incidence of adjacent vertebral re-fracture was 26.69 % (75/281). The levels of serum chemokine and SDF-1α in the re-fracture group were higher than those in the non-re-fracture group, and the level of miR-21 was lower than that in the non-re-fracture group (P < 0.05). According to Lasso-Logistic regression analysis, bone mineral density, bone cement extravasation, postoperative vertebral height recovery rate, postoperative Cobb angle, serum chemokine, SDF-1α and miR-21 were independent influencing factors of adjacent vertebral refracture after thoracolumbar fracture in the elderly (P < 0.05). Receiver operating characteristic (ROC) curve analysis showed that the area under the curve (AUC) of serum chemerin, SDF-1α and miR-21 in predicting adjacent vertebral re-fracture was 0.761 (95%CI: 0.706-0.809), 0.736 (95%CI: 0.681-0.787) and 0.773 (95%CI: 0.719-0.820). The AUC of serum chemerin, SDF-1α, miR-21 combined with clinical indicators in predicting adjacent vertebral re-fracture was 0.934 (95%CI: 0.898-0.960). The 10-fold cross-validation showed that the average AUC was 0.926 (95%CI: 0.892-0.955), and the AUC range of each fold was 0.911-0.942. The calibration curve showed that the calibration of the prediction model was good (Hosmer-Lemeshow test P > 0.05). Conclusion Serum chemerin, SDF-1α and miR-21 are independently associated with adjacent vertebral re-fracture after thoracolumbar fracture surgery in the elderly. Combined detection can effectively predict the risk of adjacent vertebral re-fracture. -
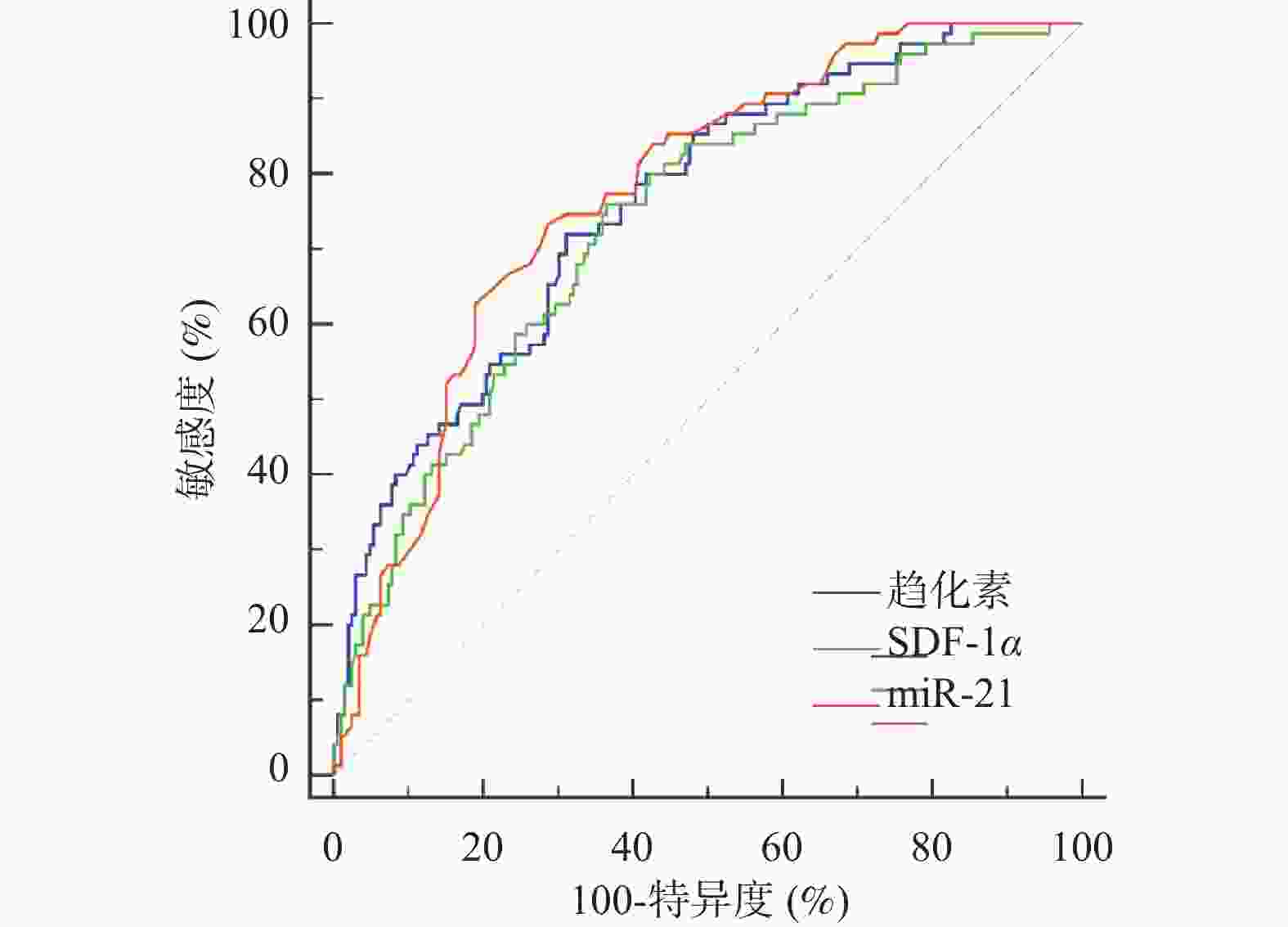
图 3 血清趋化素、SDF-1α、miR-21对邻近椎体再骨折的预测价值
Figure 3. Predictive value of serum chemerin,SDF-1α and miR-21 for adjacent vertebral re-fracture
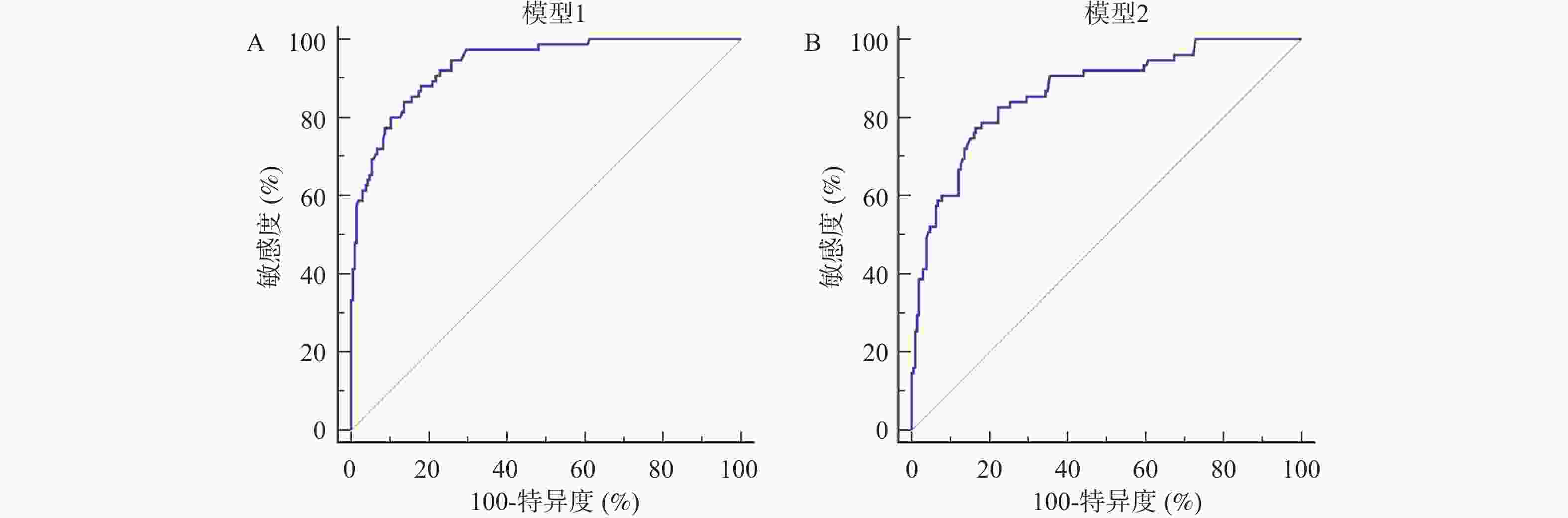
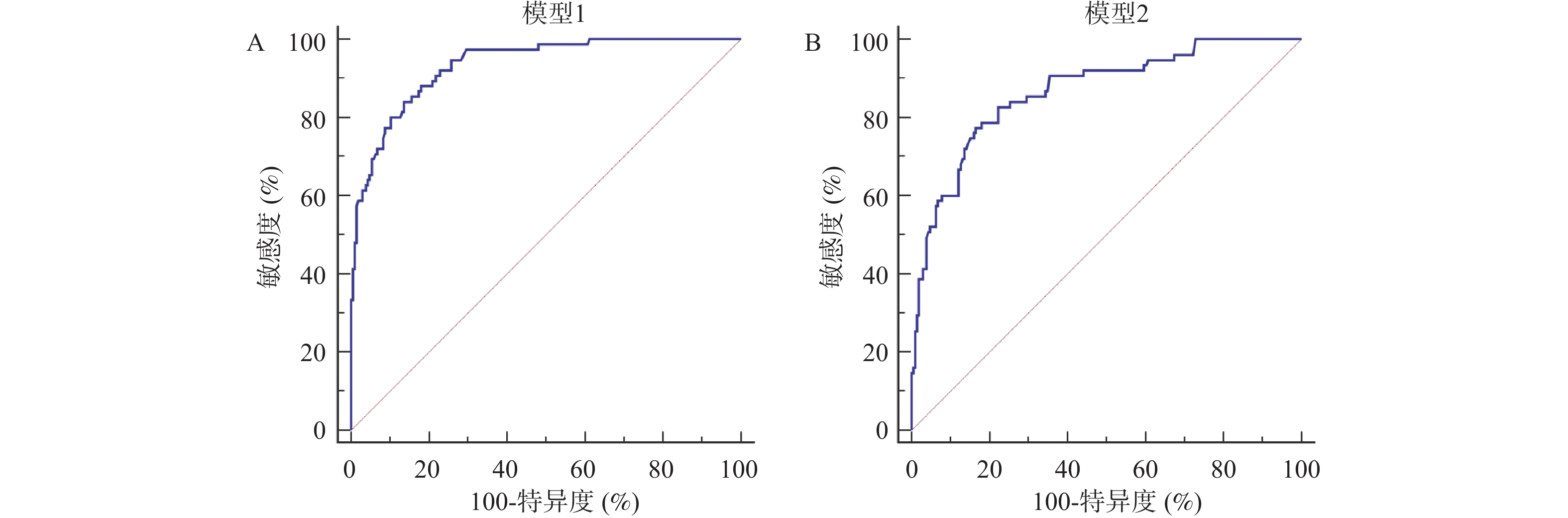
图 4 ROC曲线
A:血清趋化素、SDF-1α、miR-21联合预测模型的ROC曲线;B:血清趋化素、SDF-1α、miR-21与临床指标联合预测模型的ROC曲线
Figure 4. ROC curve
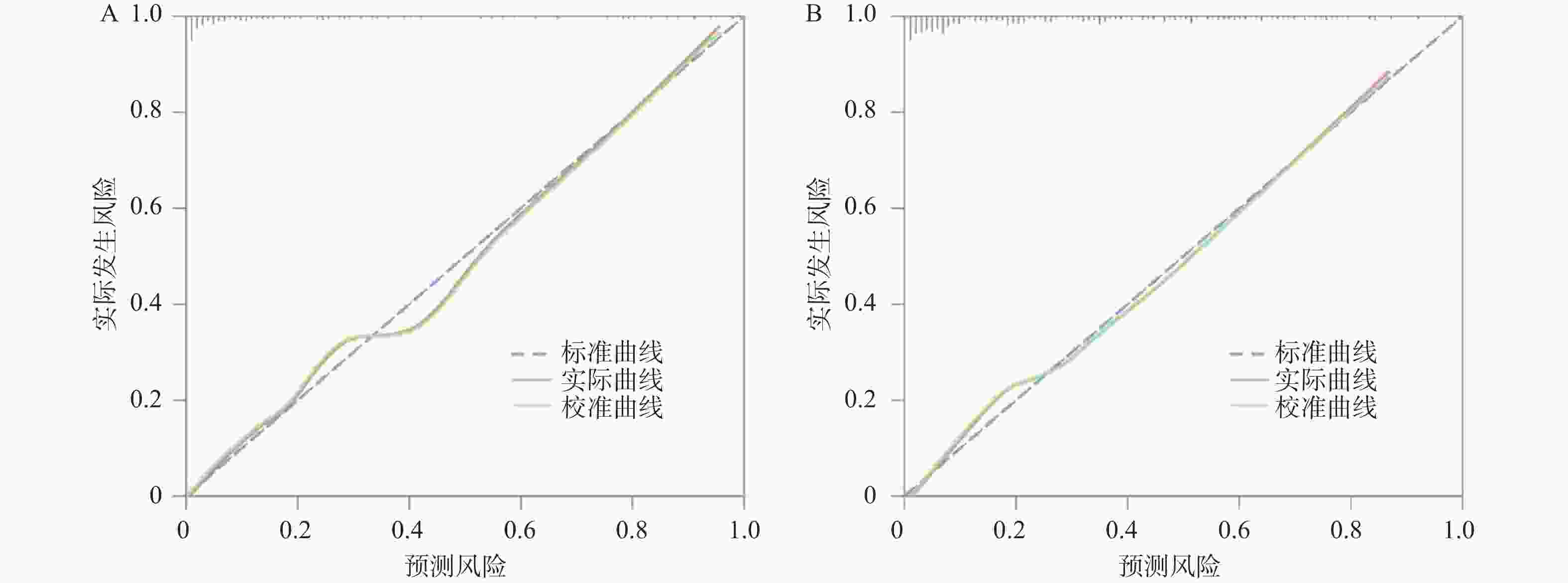
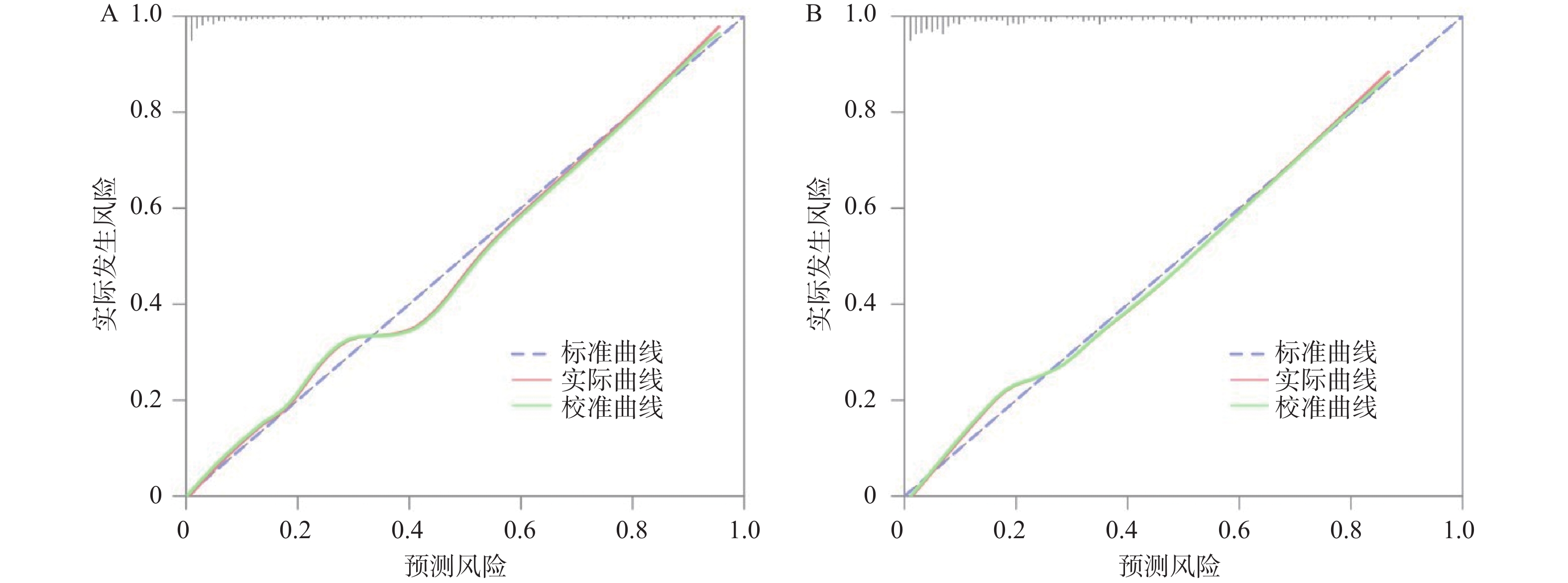
图 5 校正曲线
A:血清趋化素、SDF-1α、miR-21联合预测模型的校正曲线;B:血清趋化素、SDF-1α、miR-21与临床指标联合预测模型的校正曲线
Figure 5. Calibration curve
表 1 miR-21与U6的引物序列
Table 1. Primer sequences of miR-21 and U6
基因 序列(5'→3') miR-21 TAGCTTATCAGACTGATGTTGA AGTGCAGGGTCCGAGGTATT U6 TGCGATAGGCTATAGCGGAGAGATCGAGACTAG AGCGCGATAGGCGGCTAAGCTA  下载: 导出CSV
下载: 导出CSV
表 2 再骨折组与非再骨折组的临床资料比较[n(%)/($\bar x \pm s $)]
Table 2. Comparison of clinical data between re-fracture group and non-re-fracture group [n(%)/($\bar x \pm s $)]
资料 再骨折组(n=75) 非再骨折组(n=206) t/χ2 P 性别 0.023 0.879 男 39(52.00) 105(50.97) 女 36(48.00) 101(49.03) BMI(kg/m2) 23.85 ± 1.09 23.71 ± 1.16 0.909 0.364 年龄(岁) 68.72 ± 2.41 66.15 ± 2.03 8.916 <0.001* 骨密度(SD) −3.84 ± 0.44 −3.38 ± 0.30 9.952 <0.001* 吸烟 34(45.33) 90(43.69) 0.060 0.806 饮酒 30(40.00) 85(41.26) 0.036 0.849 高血压 21(28.00) 55(26.70) 0.047 0.828 糖尿病 13(17.33) 31(15.05) 0.217 0.641 骨折椎体节段 0.088 0.930 T11 5(6.67) 12(5.83) T12 25(33.33) 71(34.47) L1 28(37.33) 79(38.35) L2 17(22.67) 44(21.36) 椎体压缩骨折分级 0.022 0.982 1级 16(21.33) 41(19.90) 2级 26(34.67) 76(36.89) 3级 33(44.00) 89(43.20) 手术方式 0.201 0.654 PVP 47(62.67) 123(59.71) PKP 28(37.33) 83(40.29) 手术时间(min) 130.25 ± 28.64 125.84 ± 24.91 1.260 0.209 骨水泥注入量(mL) 5.43 ± 0.96 4.52 ± 0.85 7.663 <0.001* 骨水泥外渗 61.227 <0.001* 有 29(38.67) 7(3.40) 无 46(61.33) 199(96.60) 术后椎体高度恢复率(%) 13.12 ± 3.04 15.55 ± 3.39 5.459 <0.001* 术后Cobb角(°) 14.58 ± 1.43 13.20 ± 1.21 8.044 <0.001* 术后抗骨质疏松治疗 0.707 0.400 有 71(94.67) 201(97.57) 无 4(5.33) 5(2.43) *P < 0.05。
下载: 导出CSV
表 3 再骨折组与非再骨折组的血清趋化素、SDF-1α、miR-21比较($ \bar x \pm s $)
Table 3. Comparison of serum chemerin,SDF-1α and miR-21 between re-fracture group and non-re-fracture group ($\bar x \pm s $)
组别 n 趋化素(ng/mL) SDF-1α(ng/mL) miR-21 再骨折组 75 86.51 ± 15.24 52.26 ± 14.05 0.68 ± 0.23 非再骨折组 206 73.07 ± 12.55 40.74 ± 11.87 1.02 ± 0.35 t 7.484 6.842 7.816 P <0.001* <0.001* <0.001* *P < 0.05。
下载: 导出CSV
表 4 邻近椎体再骨折的Lasso-Logistic回归分析
Table 4. Lasso-Logistic regression analysis of adjacent vertebral re-fracture
变量 β S.E. Waldχ2 P OR 95%CI 模型1 骨密度 −0.824 0.081 103.454 <0.001* 0.439 0.374~0.514 骨水泥外渗 1.107 0.095 135.805 <0.001* 3.026 2.512~3.645 术后椎体高度恢复率 −0.701 0.087 65.001 0.012* 0.496 0.418~0.588 术后Cobb角 0.773 0.079 95.767 <0.001* 2.166 1.856~2.529 趋化素 0.670 0.067 100.031 <0.001* 1.954 1.714~2.229 SDF-1α 0.726 0.072 101.684 <0.001* 2.067 1.795~2.380 miR-21 −0.723 0.070 106.705 <0.001* 0.485 0.423~0.557 常数项 −1.085 0.101 117.832 <0.001* − − *P < 0.05。
下载: 导出CSV
-
[1] 中华医学会骨质疏松和骨矿盐疾病分会. 中国骨质疏松症流行病学调查及"健康骨骼" 专项行动结果发布[J]. 中华骨质疏松和骨矿盐疾病杂志, 2019, 12(4): 317-318. [2] Lu A Q, Wang X P, Huang D Q, et al. Percutaneous curved vertebroplasty for osteoporotic vertebral compression fracture[J]. Asian J Surg, 2022, 45(10): 2050-2051. [3] Dai C Q, Liang G, Zhang Y S, et al. Risk factors of vertebral re-fracture after PVP or PKP for osteoporotic vertebral compression fractures, especially in Eastern Asia: A systematic review and meta-analysis[J]. J Orthop Surg Res, 2022, 17(1): 161. [4] Goldman-Daleo H, Rachman B, Mhaskar R. Adjacent fracture rates following balloon kyphoplasty in osteoporotic vertebral compression fractures: A case series[J]. Cureus, 2023, 15(6): e40651. [5] Wang J, Xie X, Gou Y, et al. Forearm bone mineral density as a predictor of adjacent vertebral refracture after percutaneous kyphoplasty in patients with osteoporotic vertebral compression fracture: A retrospective analysis[J]. J Orthop Surg Res, 2024, 19(1): 788. [6] Tariq S, Jabbar S, Ahmad A, et al. Bridging the Gap: A narrative review of osteoporosis disability, adipokines, and the role of AI in postmenopausal women[J]. Pak J Med Sci, 2024, 40(7): 1572-1577. [7] Yang X W, Huang H X, Wang F, et al. Elevated plasma CXCL12/SDF-1 levels are linked with disease severity of postmenopausal osteoporosis[J]. Innate Immun, 2020, 26(3): 222-230. [8] Si Z X, Zhou S F, Shen Z L, et al. Increased circulating microRNA-21 level as a potential indicator for predicting a higher risk of incident fragility fractures[J]. J Osteopath Med, 2023, 124(3): 121-125. [9] Wang R J, Xu Y Y, Ma X L. Risk factors and strategies for recovery quality, postoperative pain, and recurrent fractures between percutaneous kyphoplasty and percutaneous vertebroplasty in elderly patients with thoracolumbar compression fractures: A retrospective comparative cohort study[J]. Ann Transl Med, 2023, 11(2): 122. doi: 10.21037/atm-22-6475 [10] 中国康复医学会骨质疏松预防与康复专业委员会. 骨质疏松性椎体压缩骨折诊治专家共识(2021版)[J]. 中华医学杂志, 2021, 101(41): 3371-3379. [11] 中国健康促进基金会基层医疗机构骨质疏松症诊断与治疗专家共识委员会. 基层医疗机构骨质疏松症诊断和治疗专家共识(2021)[J]. 中国骨质疏松杂志, 2021, 27(7): 937-944. [12] Yang F G, Luo Y C, Chen K, et al. Genant grade-based stratification in percutaneous curved kyphoplasty: Superior early analgesic efficacy and cement distribution characteristics in moderate to severe osteoporotic vertebral compression fractures[J]. Neurosurg Rev, 2025, 49(1): 59. [13] 杨勇, 周晓光, 陈其昕, 等. 老年骨质疏松性胸腰椎压缩骨折经皮椎体强化术术后椎体再骨折诊疗指南(2025版)[J]. 中华创伤杂志, 2025, 41(7): 613-626. [14] He L, Li W, Zhai XP, et al. Risk factors for adjacent vertebral fracture after kyphoplasty or percutaneous vertebroplasty in osteoporotic vertebral systematic review and meta-analysis compression fractures[J]. Eur Spine J, 2025, 34(11): 5126-5141. [15] Cheng H W, Wen H L, Ma Y, et al. Development and validation of a nomogram for predicting adjacent vertebral fracture after osteoporotic vertebral compression fracture surgery: A multicenter retrospective cohort study[J]. Neurospine, 2025, 22(2): 592-602. [16] 胡浩, 曹开学, 黄攀, 等. 超高龄骨质疏松性胸腰椎压缩骨折经皮椎体成形术术后邻椎再骨折的危险因素分析[J]. 中国骨伤, 2022, 35(8): 710-714. [17] 王娓娓, 章伟, 杨维杰, 等. 血清Pref-1、趋化素和Apelin-13水平对老年2型糖尿病骨质疏松并发骨折的预测价值[J]. 检验医学与临床, 2022, 19(4): 513-517. [18] 武美荣, 马志强, 杨倩, 等. 血清SDF-1α、CXCR4水平与老年腰椎压缩性骨折患者PKP后再发骨折的关系[J]. 山东医药, 2024, 64(10): 76-79. [19] Ostrowska Z, Morawiecka-Pietrzak M, Pluskiewicz W, et al. The relationship between chemerin, bone metabolism, the RANKL/RANK/OPG system, and bone mineral density in girls with anorexia nervosa[J]. Endokrynol Pol, 2022, 73(1): 26-34. [20] Scheffler J M, Gustafsson K L, Barrett A, et al. ERα signaling in a subset of CXCL12-abundant reticular cells regulates trabecular bone in mice[J]. JBMR Plus, 2022, 6(8): e10657. [21] 李雪光, 陈礼, 张文奎, 等. 血清miR-21、腰椎椎体CT值及骨密度值预测老年骨质疏松性椎体压缩性骨折术后再骨折发生风险的临床价值[J]. 中国老年学杂志, 2023, 43(24): 5930-5932. [22] Cheng J Q, Li Y, Zang T X, et al. MiR-21 accelerates tibial fracture healing in rats by regulating TGF-β1/Smad signaling pathway[J]. Panminerva Med, 2023, 65(1): 121-122. [23] Liu Y, Haibier A, Kayierhan A, et al. Clinical effect analysis of unilateral percutaneous vertebral cement distribution in the repair of osteoporotic thoracolumbar vertebral compression fractures[J]. BMC Surg, 2025, 25(1): 90. doi: 10.1186/s12893-025-02820-0 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 149
- HTML全文浏览量: 105
- PDF下载量: 98
- 被引次数: 0
