

The Relationship between Serum sTREM-1,CCR1,LGALS3BP Expression and HBV-DNA Load,Liver Function,and Degree of Liver Fibrosis in Patients with Chronic Hepatitis B
-
摘要:
目的 探究血清可溶性髓样细胞触发受体-1(soluble triggering receptor expressed on myeloid cells-1,sTREM-1)、CC 趋化因子受体1(CC chemokine receptor 1,CCR1)、半乳糖凝集素-3结合蛋白(lectin galactoside binding,soluble 3 binding protein,LGALS3BP)表达与慢性乙型肝炎(chronic hepatitis B,CHB)患者HBV-DNA载量、肝功能及肝纤维化程度的关系。 方法 回顾性纳入2024年3月至2025年3月期间于西安市第一医院就诊的120例CHB患者作为样本,检测患者血清 HBV-DNA 载量。采用ELISA检测血清sTREM-1、CCR1、LGALS3BP水平;采集肝功能[天冬氨酸转氨酶(aspartate aminotransferase,AST)、丙氨酸转氨酶(alanine aminotransferase,ALT)、γ-谷氨酰转移酶(gamma-glutamyl transferase,GGT)、总胆红素(total bilirubin,TBIL)]、肝纤维化血清学指标[透明质酸(hyaluronic Acid,HA)、层粘连蛋白(laminin,LN)、Ⅳ型胶原(collagen type Ⅳ,Ⅳ-C)、Ⅲ型前胶原氨基末端肽(procollagen III amino terminal propeptide,PC-Ⅲ)]及肝脏硬度值(liver stiffness measurement,LSM)。比较不同HBV-DNA载量及不同肝纤维化程度患者的各项指标差异,并使用Pearson或Spearman相关分析探讨指标间的相关性。通过ROC曲线评估sTREM-1、CCR1、LGALS3BP及LSM对肝纤维化的诊断效能。 结果 与低HBV-DNA载量组相比,中、高载量组患者血清sTREM-1、CCR1、LGALS3BP水平,肝功能指标(ALT、AST、GGT、TBIL),肝纤维化血清学指标(HA、LN、IV-C、PC-III)及LSM均显著升高(P < 0.05)。Pearson相关性分析显示,sTREM-1、CCR1、LGALS3BP与HBV-DNA载量、ALT、AST、GGT、TBIL、HA、LN、Ⅳ-C、PC-Ⅲ均呈正相关关系(r > 0,P < 0.05),且三者之间程正相关(r > 0,P < 0.05)。随着肝纤维化程度加重,HBV-DNA载量、sTREM-1、CCR1、LGALS3BP及LSM水平均递增(P < 0.05)。ROC曲线分析表明,sTREM-1、CCR1、LGALS3BP单项指标对肝纤维化均具有良好的预测价值,三者联合的诊断效能与LSM相当。 结论 血清sTREM-1、CCR1和LGALS3BP水平与CHB患者的HBV-DNA载量、肝功能损伤、肝纤维化程度及LSM密切相关。 -
关键词:
- 慢性乙型肝炎 /
- 肝纤维化 /
- 可溶性髓样细胞触发受体-1 /
- CC 趋化因子受体1 /
- 半乳糖凝集素-3结合蛋白
Abstract:Objective To explore the relationship between the expression of soluble triggering receptor expressed on myeloid cell-1 (sTREM-1), CC chemokine receptor 1 (CCR1), and lectin galectin-3 binding protein (LGALS3BP) in serum and the HBV-DNA load, liver function, and degree of liver fibrosis in patients with chronic hepatitis B (CHB). Methods Retrospective inclusion of 120 CHB patients who visited Xi'an First Hospital from March 2024 to March 2025 as samples, and detection of serum HBV-DNA load in patients. ELISA was used to detect the serum levels of sTREM-1, CCR1, and LGALS3BP. Collect liver function [aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma glutamyl transferase (GGT), total bilirubin (TBIL)], serum indicators of liver fibrosis [hyaluronic acid (HA), laminin (LN), collagen type IV(IV-C), procollagen III amino terminal peptide(PC-III)], and liver stiffness measurement(LSM) were collected. The differences in various indicators among patients with different HBV-DNA loads and degrees of liver fibrosis were compared, and Pearson or Spearman correlation analysis was used to explore the correlation between indicators. The diagnostic efficacy of sTREM-1, CCR1, LGALS3BP, and LSM for liver fibrosis using ROC curves was evaluated. Results Compared with the low HBV-DNA load group, the serum levels of sTREM-1, CCR1, LGALS3BP, liver function indicators (ALT, AST, GGT, TBIL), liver fibrosis serological indicators (HA, LN, IV-C, PC-III), and LSM were significantly increased in the medium and high load groups (P < 0.05). Pearson correlation analysis showed that sTREM-1, CCR1, LGALS3BP were positively correlated with HBV-DNA load, ALT, AST, GGT, TBIL, HA, LN, IV-C, and PC-III(r > 0, P < 0.05), and there was a positive correlation (r > 0, P < 0.05). As the degree of liver fibrosis worsened, the levels of HBV-DNA load, sTREM-1, CCR1, LGALS3BP, and LSM increased (P < 0.05). ROC curve analysis showed that single indicators sTREM-1, CCR1, and LGALS3BP had a good predictive value for liver fibrosis, and the combined diagnostic efficacy of the three parameters was comparable to LSM. Conclusion The levels of serum sTREM-1, CCR1, and LGALS3BP are closely related to HBV-DNA load, liver function damage, degree of liver fibrosis, and LSM in CHB patients. -
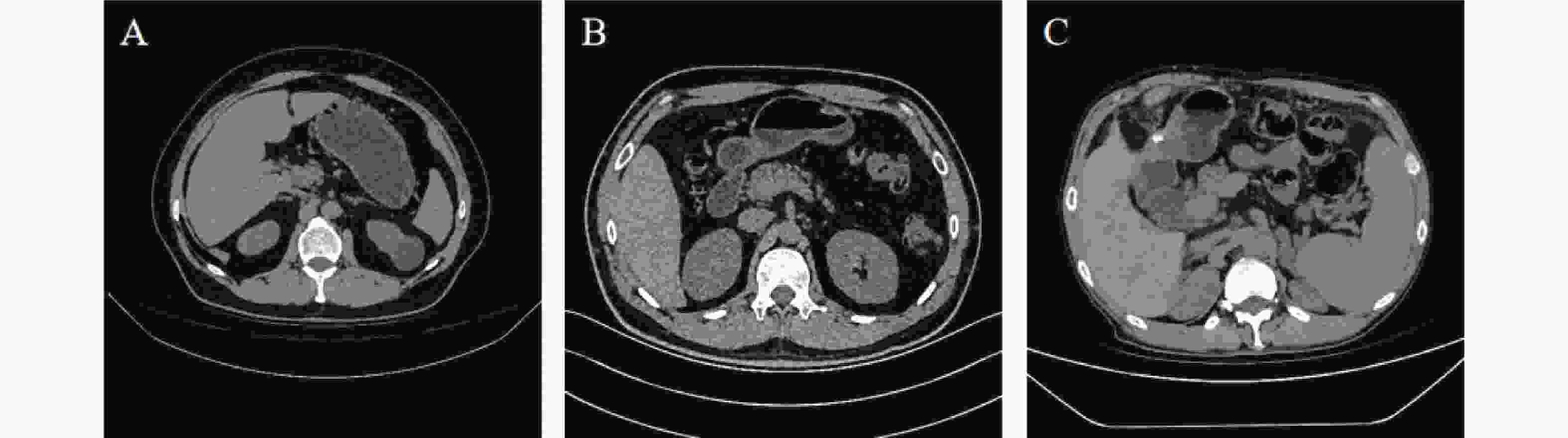
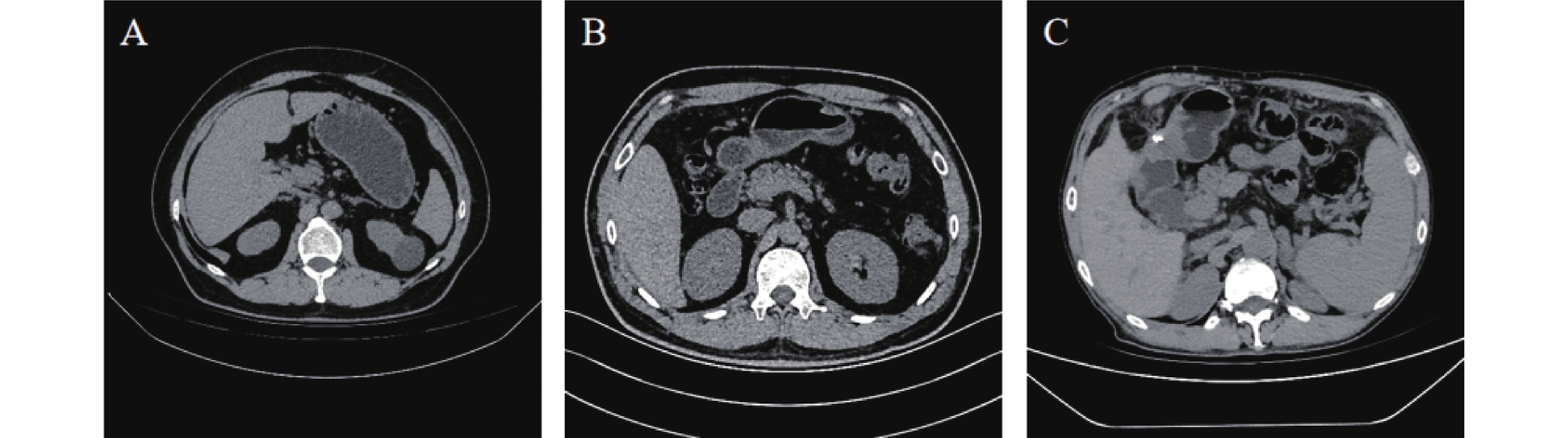
图 1 不同HBV-DNA载量患者典型CT影像
A:低载量,男,52岁,肝脏大小形态如常,表面光滑,各叶比例协调,内可见小结节状低密度影;B:中载量,男,46岁,肝脏大小、形态未见明显异常,表面欠光滑,肝实质内未见明显异常密度影;C:高载量,男,58岁,肝脏体积缩小,左右叶比例失调,轮廓部分欠规整,肝缘区见多个斑片状致密影。
Figure 1. Typical CT images of patients with different HBV-DNA loads
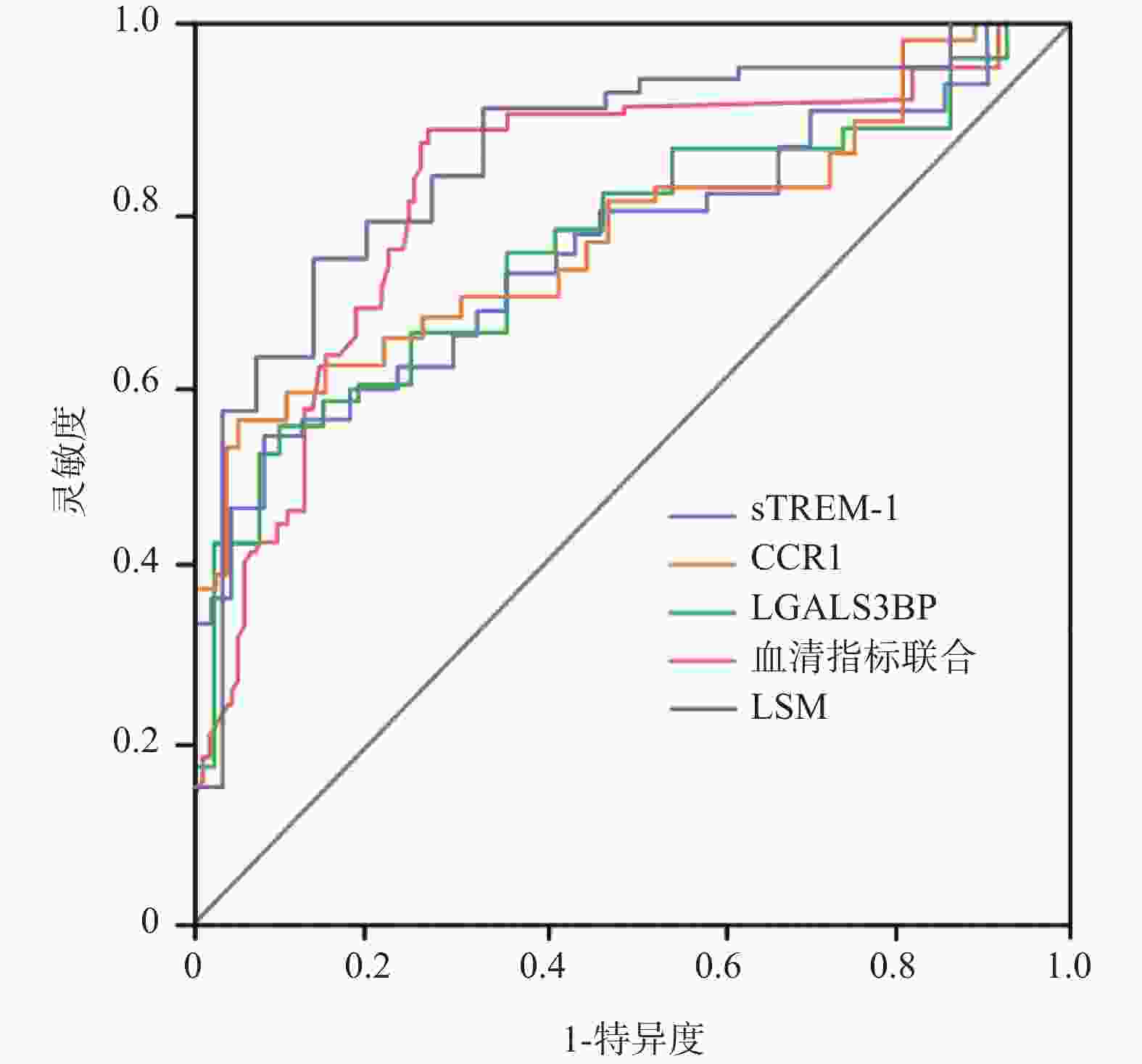
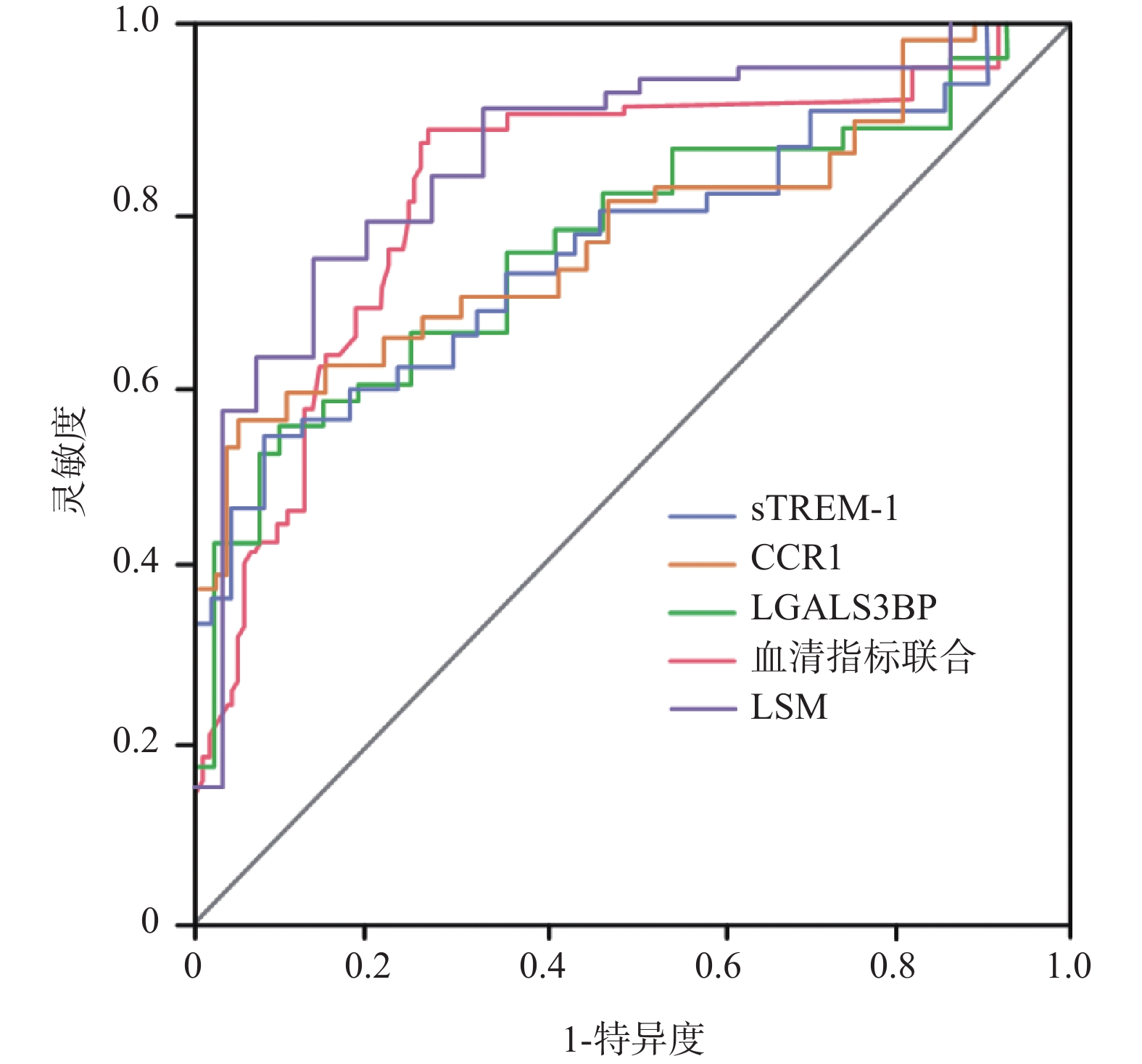
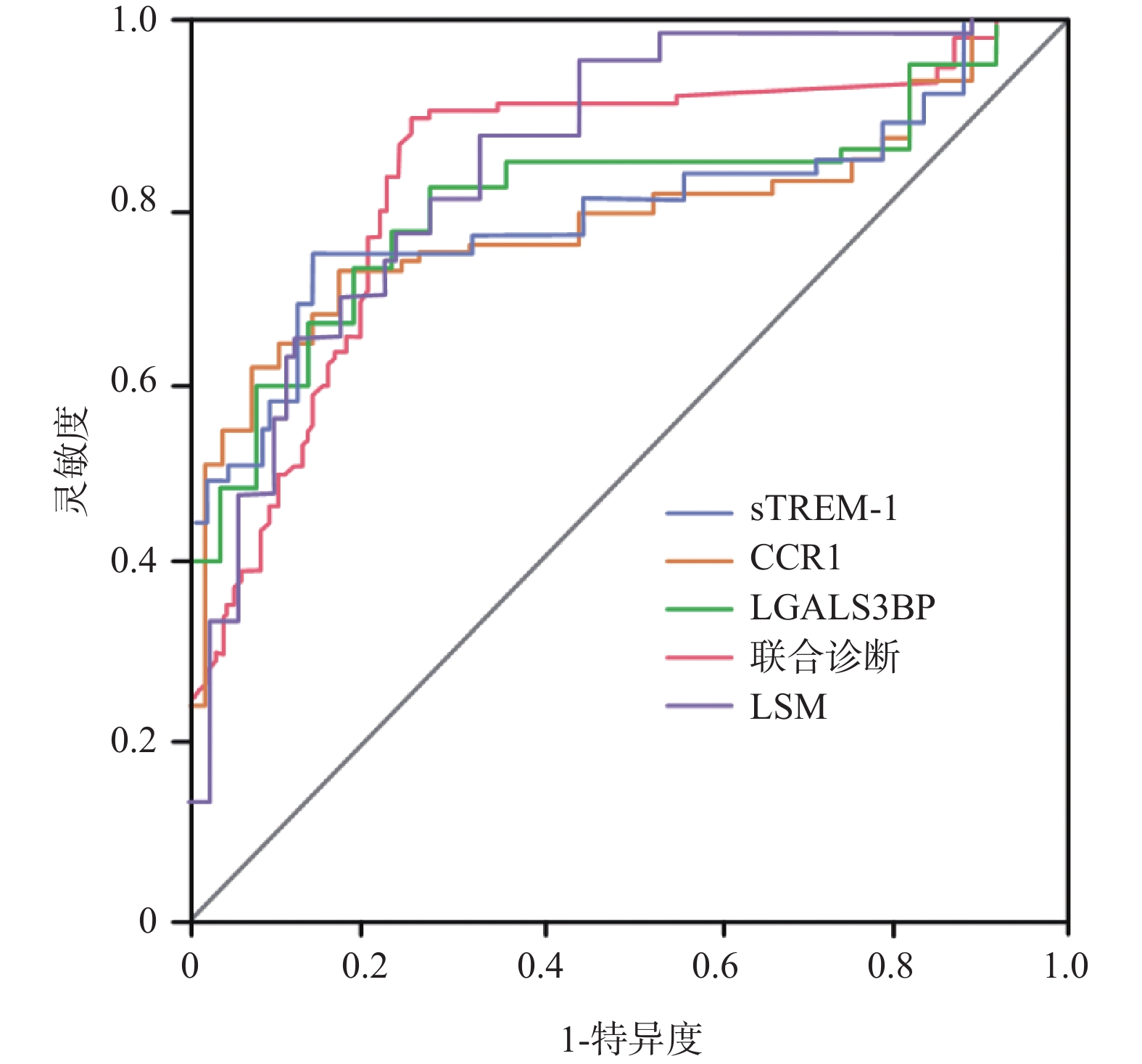
图 2 各指标及联合模型评估肝纤维化的ROC曲线
Figure 2. ROC curves for evaluating liver fibrosis using various indicators and combined models
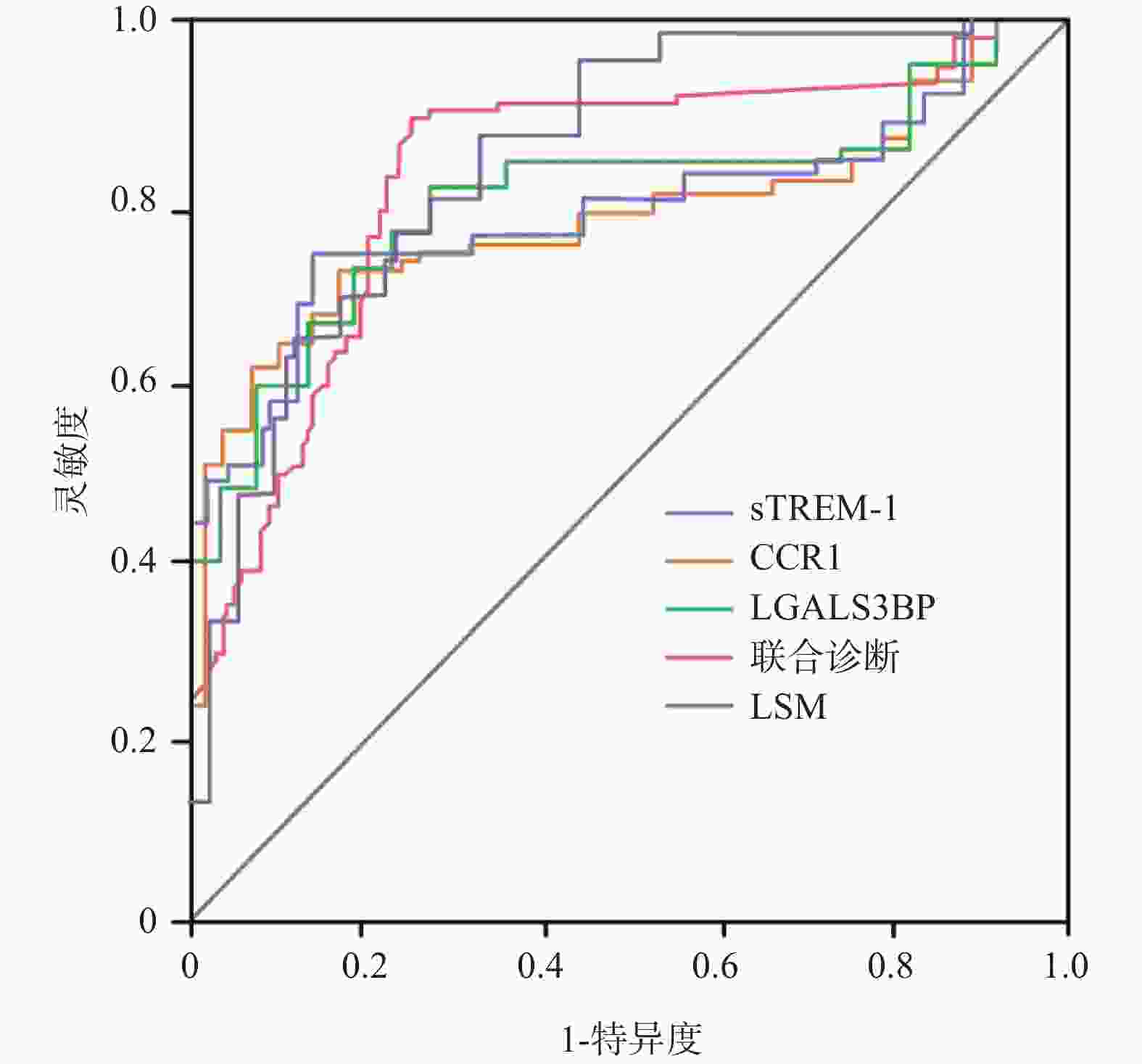
图 3 各指标及联合模型评估重度肝纤维化的ROC曲线
Figure 3. ROC curve for evaluating severe liver fibrosis using various indicators and combined models
表 1 不同HBV-DNA载量患者的临床资料比较[n(%)/($\bar x \pm s $)]
Table 1. Comparison of baseline data of patients with different HBV-DNA loads[n(%)/($\bar x \pm s $)]
项目 低载量组(n = 42) 中载量组(n = 37) 高载量组(n = 41) χ2/F P 年龄(岁) 52.63 ± 6.82 50.91 ± 7.24 52.75 ± 7.05 0.823 0.442 性别 0.128 0.938 男 24(57.14) 22(59.46) 25(60.98) 女 18(42.86) 15(40.54) 16(39.02) BMI(kg/m2) 23.17 ± 2.86 22.94 ± 3.12 23.45 ± 2.97 0.287 0.751 病程(月) 28.42 ± 7.36 31.05 ± 8.28 31.83 ± 8.94 1.959 0.146 婚姻情况 2.083 0.721 已婚 35(83.33) 31(83.78) 33(80.49) 未婚 5(11.90) 6(16.22) 6(14.63) 离异、丧偶 2(4.76) 0 2(4.88) 吸烟史 0.095 0.954 有 19(45.24) 18(48.65) 19(46.34) 无 23(54.76) 19(51.35) 22(53.66) 饮酒史 0.704 0.703 有 15(35.71) 16(43.24) 18(43.90) 无 27(64.29) 21(56.76) 23(56.10) 高血压史 0.251 0.882 有 11(26.19) 9(24.32) 12(29.27) 无 31(73.81) 28(75.68) 29(70.73) 高血脂史 0.163 0.922 有 8(19.05) 6(16.22) 8(19.51) 无 34(80.95) 31(83.78) 33(80.49) 糖尿病史 0.219 0.896 有 6(14.29) 5(13.51) 7(17.07) 无 36(85.71) 32(86.49) 34(82.93) 抗病毒治疗史 16.977 <0.001* 有 38(90.48) 25(67.57) 20(48.78) 无 4(9.52) 12(32.43) 21(51.22) *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 不同HBV-DNA载量患者血清及影像学资料比较($\bar x \pm s $)
Table 2. Comparison of serum and imaging data of patients with different HBV-DNA loads($\bar x \pm s $)
项目 低载量组(n = 42) 中载量组(n = 37) 高载量组(n = 41) F P sTREM-1(pg/mL) 125.36 ± 18.24 158.73 ± 22.65# 196.85 ± 28.47#△ 96.212 <0.001* CCR1(ng/mL) 3.25 ± 0.68 4.17 ± 0.82# 5.36 ± 0.95#△ 68.453 <0.001* LGALS3BP(ng/mL) 28.45 ± 5.32 35.62 ± 6.18# 44.83 ± 7.25#△ 70.488 <0.001* ALT(U/L) 52.16 ± 8.37 68.24 ± 10.56* 138.93 ± 23.42#△ 354.25 <0.001* AST(U/L) 48.75 ± 9.26 61.38 ± 19.45# 127.82 ± 21.38#△ 243.764 <0.001* GGT(U/L) 45.82 ± 9.13 72.47 ± 11.28# 85.69 ± 14.37#△ 123.123 <0.001* TBIL(μmol/L) 46.28 ± 3.45 56.53 ± 4.27# 73.95 ± 5.18#△ 426.903 <0.001* HA(ng/mL) 95.42 ± 16.37 157.68 ± 26.45# 228.53 ± 29.16#△ 306.66 <0.001* LN(ng/mL) 51.35 ± 13.28 68.46 ± 17.35# 95.72 ± 24.18#△ 58.474 <0.001* Ⅳ-C(ng/mL) 38.63 ± 9.25 65.87 ± 12.36# 82.45 ± 16.28#△ 121.238 <0.001* PC-Ⅲ(ng/mL) 36.28 ± 7.15 52.43 ± 9.84# 79.86 ± 13.27#△ 186.003 <0.001* LSM(kPa) 6.51 ± 1.53 9.82 ± 2.34# 15.20 ± 3.62#△ 185.750 <0.001* *P < 0.05;与低载量组比较,#P < 0.05;与中载量组比较,△P < 0.05。
下载: 导出CSV
表 3 sTREM-1、CCR1、LGALS3BP与HBV-DNA载量、肝功能及肝纤维化指标的相关性
Table 3. The correlation between sTREM-1,CCR1,LGALS3BP and HBV-DNA load,liver function,and liver fibrosis indicators
相关指标 sTREM-1 CCR1 LGALS3BP r P r P r P sTREM-1 1.000 - 0.683 <0.001* 0.725 <0.001* CCR1 0.683 <0.001* 1.000 - 0.647 <0.001* LGALS3BP 0.725 <0.001* 0.647 <0.001* 1.000 - HBV-DNA载量 0.732 <0.001* 0.706 <0.001* 0.728 <0.001* ALT 0.592 <0.001* 0.538 <0.001* 0.615 <0.001* AST 0.563 <0.001* 0.524 <0.001* 0.587 <0.001* GGT 0.527 <0.001* 0.486 <0.001* 0.553 <0.001* TBIL 0.498 <0.001* 0.452 <0.001* 0.518 <0.001* HA 0.635 <0.001* 0.572 <0.001* 0.658 <0.001* LN 0.607 <0.001* 0.543 <0.001* 0.629 <0.001* Ⅳ-C 0.586 <0.001* 0.528 <0.001* 0.605 <0.001* PC-Ⅲ 0.618 <0.001* 0.557 <0.001* 0.642 <0.001* *P < 0.05。
下载: 导出CSV
表 4 不同纤维化程度患者临床资料比较[n(%)/($\bar x \pm s $)]
Table 4. Comparison of clinical data of patients with different degrees of fibrosis[n(%)/($\bar x \pm s $)]
项目 无纤维化组(n = 37) 轻中度纤维化组(n = 48) 重度纤维化组(n = 35) χ2/F P 年龄(岁) 51.93 ± 7.25 51.76 ± 8.24 52.13 ± 9.21 0.020 0.980 性别 0.368 0.832 男 22(59.45) 27(56.25) 22(62.86) 女 15(40.55) 21(43.75) 13(37.14) BMI(kg/m2) 23.25 ± 2.74 23.13 ±3.08 23.02 ± 3.95 0.045 0.956 病程(月) 29.46 ± 7.82 30.96 ± 8.47 31.25 ± 7.63 0.535 0.587 婚姻情况 3.912 0.418 已婚 31(83.78) 37(77.08) 31(88.57) 未婚 6(16.22) 8(16.67) 3(8.67) 离异、丧偶 0 3(6.25) 1(2.86) 吸烟史 0.507 0.776 有 16(43.24) 22(45.83) 18(51.43) 无 21(56.76) 26(54.67) 17(48.57) 饮酒史 0.368 0.832 有 15(40.54) 21(43.75) 13(37.14) 无 22(59.45) 27(56.25) 22(62.86) 高血压史 0.578 0.749 有 9(24.32) 12(25.00) 11(31.43) 无 28(75.68) 36(75.00) 24(68.57) 高血脂史 0.181 0.913 有 6(16.22) 9(18.75) 7(20.00) 无 31(83.78) 39(81.25) 28(80.00) 糖尿病史 0.197 0.906 有 5(13.51) 7(14.58) 6(17.14) 无 32(86.49) 41(85.42) 29(82.86) HBV-DNA载量(Log10 IU/mL) 3.72 ± 0.65 4.54 ± 0.35# 6.23 ± 0.28#△ 291.906 <0.001* sTREM-1(pg/mL) 112.46 ± 16.83 158.27 ± 22.54# 203.69 ± 29.17#△ 139.049 <0.001* CCR1(ng/mL) 2.87 ± 0.61 4.23 ± 0.79# 5.68 ± 0.92#△ 116.19 <0.001* LGALS3BP(ng/mL) 25.38 ± 4.87 36.45 ± 6.32# 47.82 ± 7.86#△ 109.669 <0.001* ALT(U/L) 48.25 ± 7.42 69.83 ± 10.27# 132.46 ± 13.85#△ 601.177 <0.001* AST(U/L) 45.62 ± 6.83 63.47 ± 9.26# 121.28 ± 12.43#△ 604.494 <0.001* GGT(U/L) 41.35 ± 8.27 65.82 ±11.45# 89.73 ± 15.28#△ 148.791 <0.001* TBIL(μmol/L) 44.82 ± 3.16 54.57 ± 4.38# 76.64 ± 5.72#△ 472.047 <0.001* HA(ng/mL) 78.35 ± 15.24 162.68 ± 23.57# 285.42 ± 30.83#△ 682.227 <0.001* LN(ng/mL) 45.28 ± 10.47 67.35 ± 18.92# 118.63 ± 25.74#△ 137.930 <0.001* Ⅳ-C(ng/mL) 33.27 ± 8.36 68.84 ± 13.25# 84.57 ± 17.43#△ 140.282 <0.001* PC-Ⅲ(ng/mL) 32.46 ± 6.28 58.73 ±10.42# 81.25 ± 14.36#△ 185.878 <0.001* LSM(kPa) 5.83 ± 1.21 9.54 ± 2.13# 16.32 ± 3.84#△ 215.743 <0.001* *P < 0.05;与低载量组比较,#P < 0.05;与中载量组比较,△P < 0.05。
下载: 导出CSV
表 5 LSM与肝功能、肝纤维化指标的相关性分析
Table 5. Correlation analysis between LSM and liver function,liver fibrosis indicators
相关指标 LSM r P ALT 0.698 <0.001* AST 0.625 <0.001* GGT 0.584 <0.001* TBIL 0.573 <0.001* HA 0.652 <0.001* LN 0.649 <0.001* Ⅳ-C 0.622 <0.001* PC-Ⅲ 0.637 <0.001* *P < 0.05。
下载: 导出CSV
表 6 sTREM-1、CCR1、LGALS3BP与纤维化程度及LSM的相关性分析
Table 6. Correlation analysis of sTREM-1,CCR1,LGALS3BP with fibrosis degree and LSM
指标 rs(与肝纤维化程度) P r(与LSM) P sTREM-1 0.712 <0.001* 0.701 <0.001* CCR1 0.683 <0.001* 0.665 <0.001* LGALS3BP 0.725 <0.001* 0.688 <0.001* *P < 0.05。
下载: 导出CSV
表 7 各指标及联合模型对肝纤维化的预测价值
Table 7. The predictive value of various indicators and combined models for liver fibrosis
项目 AUC(95% CI) 灵敏度(%) 特异度(%) P sTREM-1 0.876(0.812~0.940) 82.76 85.19 <0.001* CCR1 0.862(0.795~0.929) 79.31 87.04 <0.001* LGALS3BP 0.891(0.832~0.950) 86.20 81.48 <0.001* LSM 0.954(0.897~0.986) 92.26 94.38 0.621 血清指标联合 0.942(0.908~0.976) 91.95 92.59 - *P < 0.05。
下载: 导出CSV
表 8 各指标及联合模型对重度肝纤维化的预测价值
Table 8. The predictive value of various indicators and combined models for severe liver fibrosis
项目 AUC(95% CI) 灵敏度(%) 特异度(%) P sTREM-1 0.893(0.832~0.954) 84.62 88.89 <0.001* CCR1 0.885(0.821~0.949) 80.76 90.74 <0.001* LGALS3BP 0.916(0.867~0.965) 88.47 85.18 <0.001* LSM 0.963(0.912~0.984) 95.71 96.49 0.105 血清指标联合 0.958(0.928~0.988) 92.31 94.45 - *P < 0.05。
下载: 导出CSV
-
[1] Wang J, Zhu L, Zhang S, et al. Clinical outcomes of treatment-naïve HBeAg-negative patients with chronic hepatitis B virus infection with low serum HBsAg and undetectable HBV DNA[J]. Emerg Microbes Infect, 2024, 13(1): 2339944. doi: 10.1080/22221751.2024.2339944 [2] 马世河, 刘文艳, 陈冲, 等. 血清GP73水平联合腹部超声检查对慢性乙型肝炎肝纤维化程度的评估价值[J]. 山东医药, 2022, 62(1): 25-29. [3] 黄平, 曾霞, 张亚萍, 等. 肝静脉波形分型联合肝脏超声半定量评分对慢性乙型肝炎患者肝纤维化程度评估价值研究[J]. 实用肝脏病杂志, 2022, 25(2): 187-190. [4] Deghdegh K, Boukadoum N, Terra B, et al. Characteristics of bronchiectasis asociated with chronic obstructive pulmonary disease[J]. Open Respir Med J, 2022, 16: e187430642203311. [5] 吴清艳, 陈柳虹, 王日, 等. HBeAg(+)与(-)HBV感染者HBV-DNA 载量及其与肝纤维化和MELD评分的关系[J]. 中华医院感染学杂志, 2023, 33(14): 2096-2099. [6] Wong G L, Lemoine M. The 2024 updated WHO guidelines for the prevention and management of chronic hepatitis B: Main changes and potential implications for the next major liver society clinical practice guidelines[J]. J Hepatol, 2025, 82(5): 918-925. doi: 10.1016/j.jhep.2024.12.004 [7] Chen J, Huang Z B, Li H, et al. Early diagnostic diomarkers of sepsis for patients with acute-on-chronic liver failure: A multicenter study[J]. Infect Dis Ther, 2021, 10(1): 281-290. doi: 10.1007/s40121-020-00362-x [8] Tian Q, Yan Z, Guo Y, et al. Inflammatory role of CCR1 in the central nervous system[J]. Neuroimmunomodulation, 2024, 31(1): 173-182. doi: 10.1159/000540460 [9] Kim D H, Sung M, Park M S, et al. Galectin 3-binding protein (LGALS3BP) depletion attenuates hepatic fibrosis by reducing transforming growth factor-β1 (TGF-β1) availability and inhibits hepatocarcinogenesis[J]. Cancer Commun, 2024, 44(10): 1106-1129. doi: 10.1002/cac2.12600 [10] 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2015 年版)[J/OL]. 中华实验和临床感染病杂志(电子版) 2015, 19(5 ): 1-19. [11] 陈春燕, 樊子勉. 慢性乙型肝炎者外周血 SAA/CRP、NLR 水平与HBV-DNA 载量、病情程度的相关性分析[J]. 昆明医科大学学报, 2024, 45(5): 144-150. [12] 王慧, 郝泉水, 肖华, 等. 乙型肝炎患者血清lncRNA XIST 表达与 HBV-DNA 载量、肝纤维化的关系[J]. 中国现代医学杂志, 2025, 35(2): 78-82. doi: 10.3969/j.issn.1005-8982.2025.02.014 [13] 中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会感染病学分 会. 肝纤维 化诊断及治疗共识(2019年)[J]. 中华肝脏病杂志, 2019, 27(9): 657-667. doi: 10.3760/cma.j.issn.1007-3418.2019.09.001 [14] 丁艺文, 操焕坤, 宗方, 等. 二维超声剪切波弹性成像和血清学指 标 评 分 诊 断 慢 性 乙 肝 患 者肝纤维化的价值[J]. 浙江医学, 2023, 45(18): 1937-1942. [15] Berzigotti A, Tsochatzis E, Boursier J, et al. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis–2021 update[J]. J Hepatol, 2021, 75(3): 659-689. doi: 10.1016/j.jhep.2021.05.025 [16] Chen Y C, Hsu C W, Chien R N. Higher HBeAg-reversion virological relapse and lower sustained remission after treatment cessation in tenofovir-treated HBeAg-positive patients[J]. J Med Virol, 2023, 95(11): e29213. doi: 10.1002/jmv.29213 [17] Lai X, Chen H, Dong X, et al. AST to ALT ratio as a prospective risk predictor for liver cirrhosis in patients with chronic HBV infection[J]. Eur J Gastroenterol Hepatol, 2024, 36(3): 338-344. doi: 10.1097/MEG.0000000000002708 [18] 易爱芬, 高明. 不同Child-Pugh分级的慢性乙型肝炎合并肝硬化患者糖代谢和胰岛素分泌情况及与炎症反应相关性研究[J]. 黑龙江医学, 2023, 47(6): 663-665. doi: 10.3969/j.issn.1004-5775.2023.06.005 [19] Dholariya S, Parchwani D N, Singh R, et al. Utility of P-SEP, sTREM-1 and suPAR as novel sepsis biomarkers in SARS-CoV-2 infection[J]. Indian J Clin Biochem, 2022, 37(2): 131-138. doi: 10.1007/s12291-021-01008-6 [20] Khanam A, Tang L S Y, Kottilil S. Programmed death 1 expressing CD8+CXCR5+ follicular T cells constitute effector rather than exhaustive phenotype in patients with chronic hepatitis B[J]. Hepatology, 2022, 75(3): 690-708. doi: 10.1002/hep.32210 [21] El Bannoudi H, Cornwell M, Luttrell-Williams E, et al. Platelet LGALS3BP as a mediator of myeloid inflammation in systemic lupus erythematosus[J]. Arthritis Rheumatol, 2023, 75(5): 711-722. doi: 10.1002/art.42382 [22] 何迪, 陈鹏, 刘锋, 等. 肝纤维化病因与机制研究进展[J]. 昆明医科大学学报, 2022, 43(11): 165-171. doi: 10.12259/j.issn.2095-610X.S20221122 [23] Yu S M, Li H, Deng G H, et al. sTREM-1 as promising prognostic biomarker for acute-on-chronic liver failure and mortality in patients with acute decompensation of cirrhosis[J]. World J Gastroenterol, 2024, 30(9): 1177-1188. doi: 10.3748/wjg.v30.i9.1177 [24] Peng W, Yang Y, Lu H, et al. Network pharmacology combines machine learning, molecular simulation dynamics and experimental validation to explore the mechanism of acetylbinankadsurin A in the treatment of liver fibrosis[J]. J Ethnopharmacol, 2024, 323: 117682. doi: 10.1016/j.jep.2023.117682 [25] Sun B, Abadjian L, Monto A, et al. Hepatitis C virus cure in human immunodeficiency virus coinfection dampens inflammation and improves cognition through multiple mechanisms[J]. J Infect Dis, 2020, 222(3): 396-406. doi: 10.1093/infdis/jiaa109 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 62
- HTML全文浏览量: 43
- PDF下载量: 38
- 被引次数: 0
