

Manual Therapy Combined with Rehabilitation Training Accelerates Recovery After Knee Replacement
-
摘要:
目的 观察肌筋膜触发点(myofascial trigger points,MTrPs)手法按摩联合周期性阶段性康复训练对全膝关节置换术后(total knee arthroplasty,TKA)康复的加速效果。 方法 选取2020年1月至2025年1月于佛山市中医院行TKA的患者116例,采用随机数字表法分为对照组(周期性阶段性康复训练)、试验组(周期性阶段性康复训练联合MTrPs手法按摩),各58例。主要、次要分析分别采用意向性治疗(intention-to-treat,ITT)原则、符合方案集(per-protocol,PP)分析。比较两组康复进程、疼痛情况、关节活动度、运动功能、膝关节功能及不良反应。 结果 ITT与PP分析结果一致:试验组屈曲90° 达成时间、独立行走时间、独立上下楼梯时间均短于对照组(P < 0.05);干预2、6、12周后试验组疼痛视觉模拟量表(visual analogue scale,VAS)评分均低于对照组(P < 0.05),两组VAS均随时间降低(P < 0.05);干预2、6、12周后试验组膝关节最大主动关节活动度(active range of motion,AROM)均大于对照组(P < 0.05),六分钟步行试验(six-minute walk test,6MWT)均长于对照组(P < 0.05),西安大略大学和麦克马斯特大学骨关节炎指数(western ontario and universities mcmaster osteoarthritis index,WOMAC)均低于对照组(P < 0.05);随着时间延长,两组AROM均呈增大趋势(P < 0.05),6MWT均呈延长趋势(P < 0.05),WOMAC评分均呈降低趋势(P < 0.05)。 结论 MTrPs手法按摩联合周期性阶段性康复训练可有效缩短TKA术后康复进程,减轻疼痛,改善膝关节功能及运动功能。 Abstract:Objective To observe the accelerated rehabilitation effects of myofascial trigger point (MTrPs) manual massage combined with periodic phased rehabilitation training following total knee arthroplasty (TKA). Methods A total of 116 patients who underwent TKA at Foshan Hospital of Traditional Chinese Medicine from January 2020 to January 2025 were selected and randomly divided into a control group (periodic phased rehabilitation training) and an experimental group (periodic phased rehabilitation training combined with MTrPs manual massage), with 58 cases in each group. The intention-to-treat (ITT) principle and per-protocol (PP) analysis were applied for the primary and secondary analyses, respectively. The rehabilitation process, pain status, range of motion, motor function, knee joint function, and adverse reactions were compared between the two groups. Results The results of the ITT and PP analyses were consistent: the time to achieve 90° of flexion, independent walking time, and independent stair-climbing time in the experimental group were all shorter than those in the control group (P < 0.05). At 2, 6, and 12 weeks after the intervention, the Visual Analogue Scale (VAS) scores in the experimental group were lower than those in the control group (P < 0.05), and the VAS scores in both groups decreased over time (P < 0.05). At 2, 6, and 12 weeks after the intervention, the maximum active range of motion (AROM) of the knee joint in the experimental group was greater than that in the control group (P < 0.05), the six-minute walk test (6MWT) distance was longer than that in the control group (P < 0.05), and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores were lower than those in the control group (P < 0.05). Over time, the AROM in both groups showed an increasing trend (P < 0.05), the 6MWT distance showed a lengthening trend (P < 0.05), and the WOMAC scores showed a decreasing trend (P < 0.05). Conclusion MTrPs manual massage combined with periodic phased rehabilitation training can effectively shorten the postoperative rehabilitation process, alleviate pain, and improve knee joint function and motor function in patients following TKA. -
Key words:
- Osteoarthritis /
- Myofascial Pain Syndrome /
- Massage /
- Rehabilitation /
- Pain
-
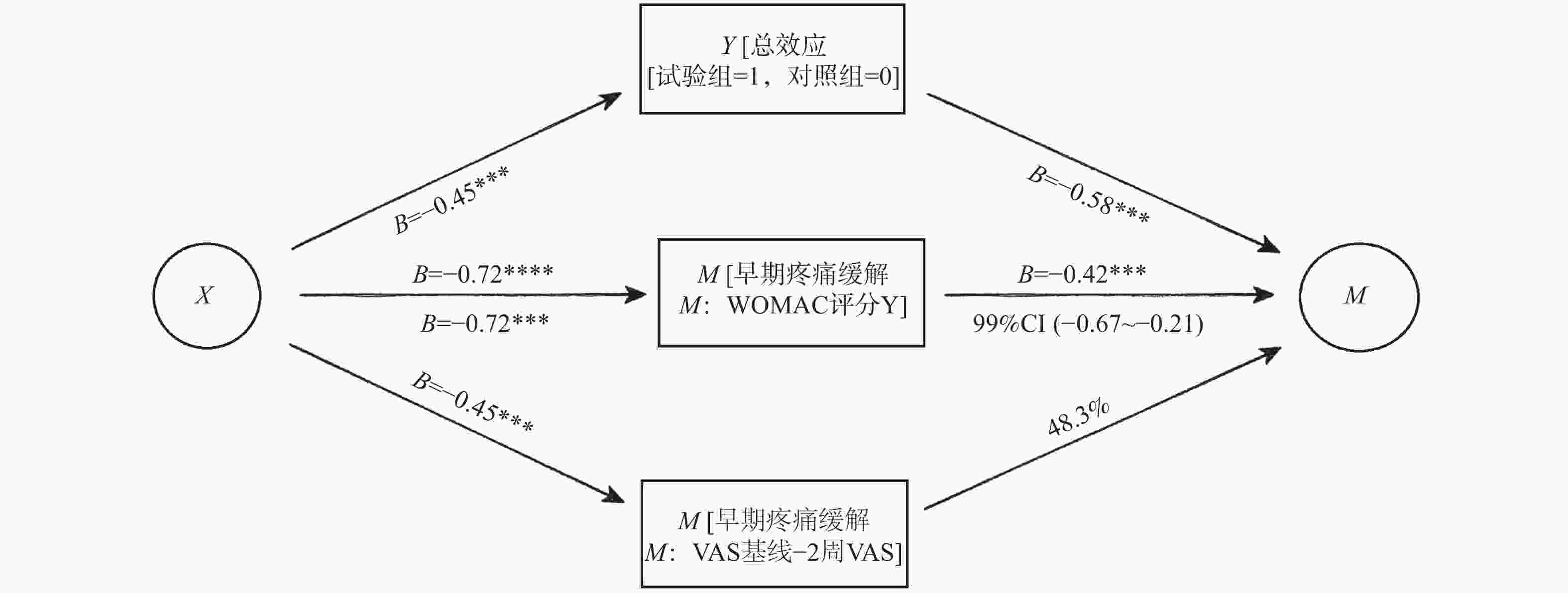
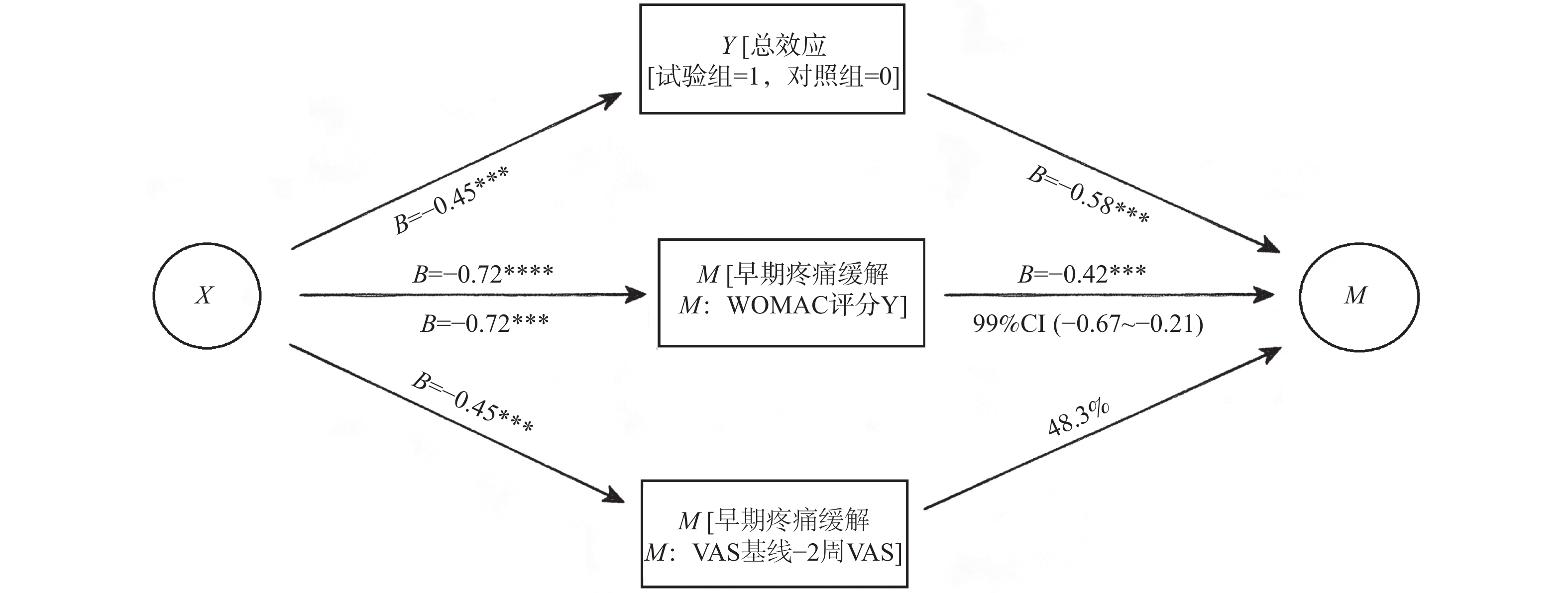
图 1 早期疼痛缓解在分组与膝关节功能之间的中介效应路径图
**P < 0.001,*P < 0.01。
Figure 1. Path diagram of the mediating effect of early pain relief between group allocation and knee function
表 1 两组基线资料比较 [n(%)/($ \bar x \pm s $)]
Table 1. Comparison of baseline data between the two groups [n(%)/($ \bar x \pm s $)]
组别 n 性别 年龄(岁) 体质量指数(kg/m2) ASA分级 男 女 I Ⅱ 对照组 53 22(41.51) 31(58.49) 69.05 ± 8.44 23.47 ± 4.01 18(33.96) 35(66.04) 试验组 53 19(35.85) 34(64.15) 70.17 ± 9.18 23.16 ± 3.74 20(37.74) 33(62.26) χ2/t 0.358 0.654 0.412 0.164 P 0.550 0.515 0.681 0.685  下载: 导出CSV
下载: 导出CSV
表 2 两组康复进程比较(PP分析,$ \bar x \pm s $,d)
Table 2. Comparison of rehabilitation progress between the two groups (PP analysis,$ \bar x \pm s $,d)
组别 n 屈曲90°达成时间 独立行走时间 独立上下楼梯时间 对照组 53 18.54 ± 3.65 27.38 ± 5.16 32.48 ± 6.12 试验组 53 16.81 ± 3.41 25.07 ± 4.61 29.17 ± 5.34 t 2.521* 2.430* 2.967* P 0.013* 0.017* 0.004* *P < 0.05。
下载: 导出CSV
表 3 两组康复进程比较(ITT分析,$ \bar x \pm s $,d)
Table 3. Comparison of rehabilitation progress between the two groups (ITT analysis,$ \bar x \pm s $,d)
组别 n 屈曲90°达成时间 独立行走时间 独立上下楼梯时间 对照组 58 18.67 ± 3.70 27.52 ± 5.23 32.61 ± 6.18 试验组 58 16.92 ± 3.45 25.19 ± 4.67 29.31 ± 5.40 t 2.634* 2.531* 3.062* P 0.010* 0.013* 0.003* *P < 0.05。
下载: 导出CSV
表 4 比较两组运动疼痛情况(PP分析,$ \bar x \pm s $,分)
Table 4. Comparison of exercise-induced pain between the two groups (PP analysis,$ \bar x \pm s $,point)
组别 n VAS 干预前 干预2周后 干预6周后 干预12周后 对照组 53 6.24 ± 1.13 5.01 ± 0.94b 3.80 ± 0.74bc 2.12 ± 0.54bcd 试验组 53 6.33 ± 1.09 4.31 ± 0.85ab 3.01 ± 0.65abc 1.73 ± 0.29abcd F F组间=18.465*,F时间=20.365*,F交互=11.252* P P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001* *P < 0.05;与对照组比较,aP < 0.05;与干预前比较,bP < 0.05;与干预2周后比较,cP < 0.05;与干预6周后比较,dP < 0.05。校正后的显著性水平统一设为0.05/6≈0.0083,表中标注的P校正后均低于此阈值。
下载: 导出CSV
表 5 比较两组运动疼痛情况(ITT分析,$ \bar x \pm s $,分)
Table 5. Comparison of exercise-induced pain between the two groups (ITT analysis,$ \bar x \pm s $,point)
组别 n VAS 干预前 干预2周后 干预6周后 干预12周后 对照组 58 6.27 ± 1.17 5.07 ± 0.96b 3.86 ± 0.77bc 2.18 ± 0.57bcd 试验组 58 6.34 ± 1.19 4.38 ± 0.87ab 3.08 ± 0.68abc 1.78 ± 0.32abcd F F组间=17.255*,F时间=19.875*,F交互=10.214* P P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001* *P < 0.05;与对照组比较,aP < 0.05;与干预前比较,bP < 0.05;与干预2周后比较,cP < 0.05;与干预6周后比较,dP < 0.05。校正后的显著性水平统一设为0.05/6≈0.0083,表中标注的P校正后均低于此阈值。
下载: 导出CSV
表 6 干预前、后两组关节活动度、运动功能、膝关节功能比较(PP分析,$ \bar x \pm s $)(1)
Table 6. Comparison of joint range of motion,motor function,and knee function between the two groups before and after intervention (PP analysis,$ \bar x \pm s $)(1)
组别 n AROM(°) 6MWT(m) 干预前 干预6周后 干预12周后 干预前 干预6周后 干预12周后 对照组 53 85.54 ± 8.49 104.47 ± 10.58b 120.54 ± 9.31bc 215.47 ± 30.36 280.14 ± 46.98b 372.54 ± 60.21bc 试验组 53 86.04 ± 8.53 115.66 ± 7.48ab 130.24 ± 8.12abc 218.67 ± 31.09 320.41 ± 39.98ab 421.15 ± 51.27abc F F组间 = 16.587*,F时间 = 20.351*,F交互 = 17.213* F组间 = 15.287*,F时间 = 19.654*,F交互 = 17.241* P P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001* P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001*
下载: 导出CSV
表 6 干预前、后两组关节活动度、运动功能、膝关节功能比较(PP分析,$ \bar x \pm s $)(2)
Table 6. Comparison of joint range of motion,motor function,and knee function between the two groups before and after intervention (PP analysis,$ \bar x \pm s $)(2)
组别 n WOMAC(分) 干预前 干预6周后 干预12周后 对照组 53 65.98 ± 8.21 42.16 ± 6.13b 28.69 ± 4.13bc 试验组 53 64.87 ± 7.93 34.75 ± 5.81ab 18.46 ± 3.46abc F F组间 = 18.459*,F时间 = 17.542*,F交互 = 20.001* P P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001* *P < 0.05;与对照组比较,aP < 0.05(组间比较仅两组,未校正)。组内不同时间点两两比较采用Bonferroni校正(同一组内共3次比较,校正后显著性水平α'=0.05/3≈0.0167)。与干预前比较,bP校正后 < 0.0167;与干预6周后比较,cP校正后 < 0.0167。
下载: 导出CSV
表 7 干预前、后两组关节活动度、运动功能、膝关节功能比较(ITT分析,$ \bar x \pm s $)(1)
Table 7. Comparison of joint range of motion,motor function,and knee function between the two groups before and after intervention (ITT analysis,$ \bar x \pm s $)(1)
组别 n AROM(°) 6MWT(m) 干预前 干预6周后 干预12周后 干预前 干预6周后 干预12周后 对照组 58 85.49 ± 7.35 103.89 ± 10.72b 119.83 ± 9.52bc 215.77 ± 30.18 278.52 ± 47.31b 369.87 ± 61.03bc 试验组 58 86.01 ± 8.24 114.97 ± 7.65ab 129.51 ± 8.34abc 217.93 ± 31.17 318.76 ± 40.22ab 418.62 ± 52.16abc F F组间 = 15.987*,F时间 = 21.575*,F交互 = 16.447* F组间 = 14.852*,F时间 = 20.611*,F交互 = 18.305* P P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001* P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001*
下载: 导出CSV
表 7 干预前、后两组关节活动度、运动功能、膝关节功能比较(ITT分析,$ \bar x \pm s $)(2)
Table 7. Comparison of joint range of motion,motor function,and knee function between the two groups before and after intervention (ITT analysis,$ \bar x \pm s $)(2)
组别 n WOMAC(分) 干预前 干预6周后 干预12周后 对照组 58 65.25 ± 8.13 42.68 ± 6.25b 29.15 ± 4.28bc 试验组 58 64.97 ± 7.87 35.21 ± 5.94ab 19.03 ± 3.57abc F F组间 = 17.895*,F时间 = 16.954*,F交互 = 21.325* P P组间 < 0.001*,P时间 < 0.001*,P交互 < 0.001* *P < 0.05;与对照组比较,aP < 0.05(组间比较仅两组,未校正)。组内不同时间点两两比较采用Bonferroni校正(同一组内共3次比较,校正后显著性水平α'=0.05/3≈0.0167)。与干预前比较,bP校正后 < 0.0167;与干预6周后比较,cP校正后 < 0.0167。
下载: 导出CSV
表 9 两组股四头肌肌力等级分布比较[ITT分析,n(%)]
Table 9. Comparison of quadriceps muscle strength grade distribution between the two groups [ITT analysis,n(%)]
组别 n 时间点 1级 2级 3级 4级 5级 Z P 对照组 58 干预前 16(27.59) 27(46.55) 11(18.97) 4(6.90) 0(0.00) 干预6周后 5(8.62) 20(34.48) 24(41.38) 9(15.52) 0(0.00) 干预12周后 2(3.45) 9(15.52) 22(37.93) 22(37.93) 3(5.17) 试验组 58 干预前 15(25.86) 29(50.00) 10(17.24) 4(6.90) 0(0.00) 0.310a 0.757 干预6周后 3(5.17) 13(22.41) 26(44.83) 16(27.59) 0(0.00) 2.583a 0.011 干预12周后 1(1.72) 5(8.62) 15(25.86) 29(50.00) 8(13.79) 3.764a <0.001 *P < 0.05;a为与对照组同时间点比较的Mann-Whitney U检验统计量Z值。组内比较(Friedman M检验):对照组χ2 = 78.564,P < 0.001;试验组χ2 = 85.431,P < 0.001。两两比较(Wilcoxon符号秩检验,Bonferroni校正)显示各时间点间差异均有统计学意义(P < 0.0167 )。
下载: 导出CSV
表 8 两组股四头肌肌力等级分布比较[PP分析,n(%)]
Table 8. Comparison of quadriceps muscle strength grade distribution between the two groups [n(%)]
组别 n 时间点 1级 2级 3级 4级 5级 Z P 对照组 53 干预前 15(28.30) 25(47.17) 10(18.87) 3(5.66) 0(0.00) 干预6周后 4(7.55) 18(33.96) 22(41.51) 9(16.98) 0(0.00) 干预12周后 1(1.89) 8(15.09) 20(37.74) 21(39.62) 3(5.66) 试验组 53 干预前 14(26.42) 27(50.94) 9(16.98) 3(5.66) 0(0.00) 0.317a 0.751 干预6周后 2(3.77) 11(20.75) 24(45.28) 16(30.19) 0(0.00) 2.641a 0.008 干预12周后 0(0.00) 4(7.55) 13(24.53) 27(50.94) 9(16.98) 3.892a <0.001 *P < 0.05;a为与对照组同时间点比较的Mann-Whitney U检验统计量Z值。组内比较(Friedman M检验):对照组χ2 = 78.564,P < 0.001;试验组χ2 = 85.431,P < 0.001。两两比较(Wilcoxon符号秩检验,Bonferroni校正)显示各时间点间差异均有统计学意义(P < 0.0167)。
下载: 导出CSV
表 10 中介效应分析结果:早期疼痛缓解在分组与膝关节功能之间的中介作用
Table 10. Mediation analysis results: the mediating role of early pain relief between group allocation and knee function
效应类型 效应值(B) 标准误 95%CI 占比(%) 总效应 −0.87 0.11 −1.09~−0.65 100.0 直接效应 −0.45 0.12 −0.69~−0.21 51.7 间接效应(中介) −0.42 0.12 −0.67~−0.21 48.3
下载: 导出CSV
-
[1] Pagan C A, Karasavvidis T, Cohen-Rosenblum A R, et al. Technology in total knee arthroplasty in 2023[J]. J Arthroplasty, 2024, 39(9): S54-S59. doi: 10.1016/j.arth.2024.07.028 [2] GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: A systematic analysis for the Global Burden of Disease Study 2021[J]. Lancet Rheumatol, 2023, 5(9): e508-e522. doi: 10.1016/S2665-9913(23)00163-7 [3] Monsegue A P, Emans P, van Loon L J C, et al. Resistance exercise training to improve post-operative rehabilitation in knee arthroplasty patients: A narrative review[J]. Eur J Sport Sci, 2024, 24(7): 938-949. doi: 10.1002/ejsc.12114 [4] Lam C, Francio V T, Gustafson K, et al. Myofascial pain–A major player in musculoskeletal pain[J]. Best Pract Res Clin Rheumatol, 2024, 38(1): 101944. doi: 10.1016/j.berh.2024.101944 [5] Müggenborg F, de Castro Carletti E M, Dennett L, et al. Effectiveness of manual trigger point therapy in patients with myofascial trigger points in the orofacial region—a systematic review[J]. Life, 2023, 13(2): 336. doi: 10.3390/life13020336 [6] Bingölbali Ö, Taşkaya C, Alkan H, et al. The effectiveness of deep tissue massage on pain, trigger point, disability, range of motion and quality of life in individuals with myofascial pain syndrome[J]. Somatosens Mot Res, 2024, 41(1): 11-17. doi: 10.1080/08990220.2023.2165054 [7] 胡雯, 江秀贵, 曹铨, 等. 周期性阶段性康复训练对老年膝骨性关节炎置换术后患者下肢肌力和膝关节功能的影响[J]. 浙江医学, 2024, 46(22): 2426-2429+2439. doi: 10.12056/j.issn.1006-2785.2024.46.22.2024-1265 [8] Glowalla C, Langer S, von Eisenhart-Rothe R. Modern knee replacement and aftercare[J]. MMW Fortschr Med, 2024, 166(21-22): 52-55. [9] 中华医学会骨科学分会关节外科学组. 骨关节炎诊疗指南(2018年版)[J]. 中华骨科杂志, 2018, 38(12): 705-715. [10] Hurwitz E E, Simon M, Vinta S R, et al. Adding examples to the ASA-physical status classification improves correct assignment to patients[J]. Anesthesiology, 2017, 126(4): 614-622. doi: 10.1097/ALN.0000000000001541 [11] Jiao S, Feng Z, Huang J, et al. Enhanced recovery after surgery combined with quantitative rehabilitation training in early rehabilitation after total knee replacement: a randomized controlled trial[J]. Eur J Phys Rehabil Med, 2024, 60(1): 74-83. doi: 10.23736/s1973-9087.23.07899-1 [12] Faiz K W. VAS--visuell analog skala[J]. Tidsskr Nor Laegeforen, 2014, 134(3): 323. [13] 严攀, 刘波, 阴俊, 等. 西安大略和麦克马斯特大学骨关节炎指数用于膝退行性骨关节炎患者评定的反应度研究[J]. 中国康复医学杂志, 2016, 31(2): 215-216. doi: 10.3969/j.issn.1001-1242.2016.02.019 [14] Meert L, Mertens M G, Meeus M, et al. Identification of metabolic factors and inflammatory markers predictive of outcome after total knee arthroplasty in patients with knee osteoarthritis: A systematic review[J]. Int J Environ Res Public Health, 2023, 20(10): 5796. doi: 10.3390/ijerph20105796 [15] Lützner J, Beyer F, Lützner C, et al. Increased inflammatory response is associated with less favorable functional results 5 years after total knee arthroplasty[J]. Knee Surg Sports Traumatol Arthrosc, 2023, 31(4): 1316-1322. doi: 10.1007/s00167-021-06836-w [16] Ferembach B, Pina C, Fata Nahhas O, et al. Total knee arthroplasty and persistent pain: A neuropathic perspective on peroneal and saphenous nerve compression[J]. Int Orthop, 2025, 49(4): 835-844. doi: 10.1007/s00264-025-06466-8 [17] Koga M, Maeda A, Morioka S. Description of pain associated with persistent postoperative pain after total knee arthroplasty[J]. Sci Rep, 2024, 14: 15217. doi: 10.1038/s41598-024-66122-w [18] Duarte F C K, Chien R, Ghazinour G, et al. Myofascial pain as an unseen comorbidity in osteoarthritis: A scoping review[J]. Clin J Pain, 2023, 39(4): 188-201. doi: 10.1097/AJP.0000000000001102 [19] Konnyu K J, Thoma L M, Cao W, et al. Rehabilitation for total knee arthroplasty: A systematic review[J]. Am J Phys Med Rehabil, 2023, 102(1): 19-33. doi: 10.1097/PHM.0000000000002008 [20] Agarwal S, Bedekar N, Shyam A, et al. Comparison between effects of instrument-assisted soft tissue mobilization and manual myofascial release on pain, range of motion and function in myofascial pain syndrome of upper trapezius - A randomized controlled trial[J]. Physiother J, 2024, 44(1): 57-67. [21] 张子龙, 张世卿, 王喆, 等. 推拿联合肌筋膜触发点针刺原发性痛经疗效研究[J]. 陕西中医, 2024, 45(7): 975-979. [22] Aftab S, Ali H N, Saeed B, et al. Early physiotherapy for post-total knee arthroplasty recovery: A systematic review of randomized controlled trials on quality of life, pain, and range of motion outcomes[J]. Musculoskeletal Care, 2025, 23(3): e70158. doi: 10.1002/msc.70158 [23] Churchill L, John Bade M, Koonce R C, et al. The past and future of peri-operative interventions to reduce arthrogenic quadriceps muscle inhibition after total knee arthroplasty: A narrative review[J] Osteoarthr Cartil Open, 2023, 6(1): 100429. [24] Larsen J B, Skou S T, Laursen M, et al. Exercise and pain neuroscience education for patients with chronic pain after total knee arthroplasty: A randomized clinical trial[J]. JAMA Netw Open, 2024, 7(5): e2412179. doi: 10.1001/jamanetworkopen.2024.12179 [25] Zhao C, Liao Q, Yang D, et al. Advances in perioperative pain management for total knee arthroplasty: a review of multimodal analgesic approaches[J]. J Orthop Surg Res, 2024, 19(1): 843. doi: 10.1186/s13018-024-05324-4 [26] Lim W. Effect of PNF stretching performed in the AKE position on hip, knee, and ankle flexibility[J]. J Back Musculoskelet Rehabil, 2024, 37(2): 389-394. doi: 10.3233/BMR-230110 [27] 王鹏云, 李晨, 沈茂荣, 等. 肌筋膜触发点手法按摩联合等速肌力训练治疗髌骨软化症的疗效观察[J]. 广东医学, 2024, 45(9): 1172-1176. [28] Chen R, Jin Y, Jin Z, et al. Massage for rehabilitation after total knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials[J]. J Orthop Surg Res, 2024, 19(1): 307. doi: 10.1186/s13018-024-04798-6 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 116
- HTML全文浏览量: 61
- PDF下载量: 21
- 被引次数: 0
