

Risk Factors and Drug Resistance Analysis of Central Venous Catheter-related Fungal Infections in Maintenance Hemodialysis Patients
-
摘要:
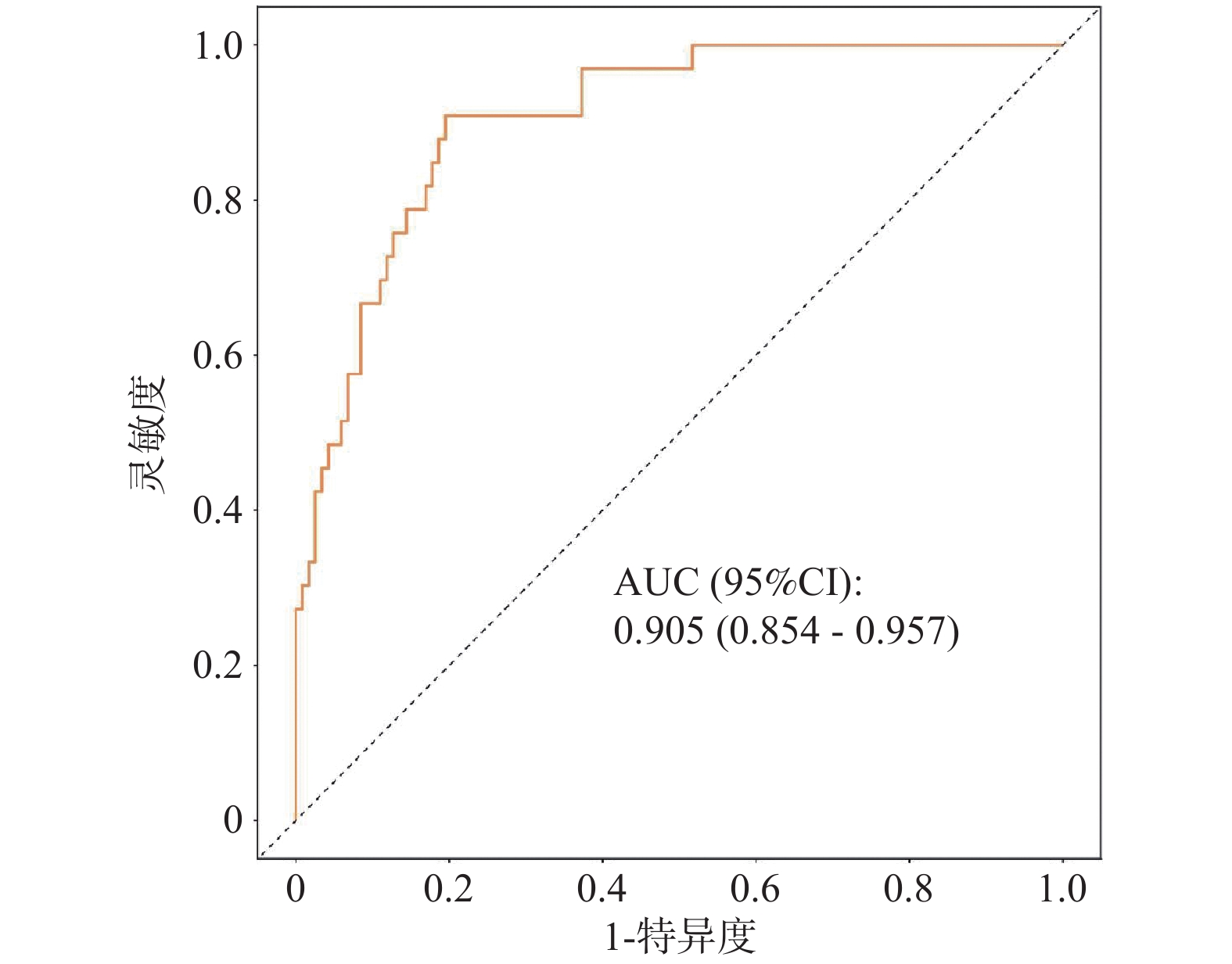
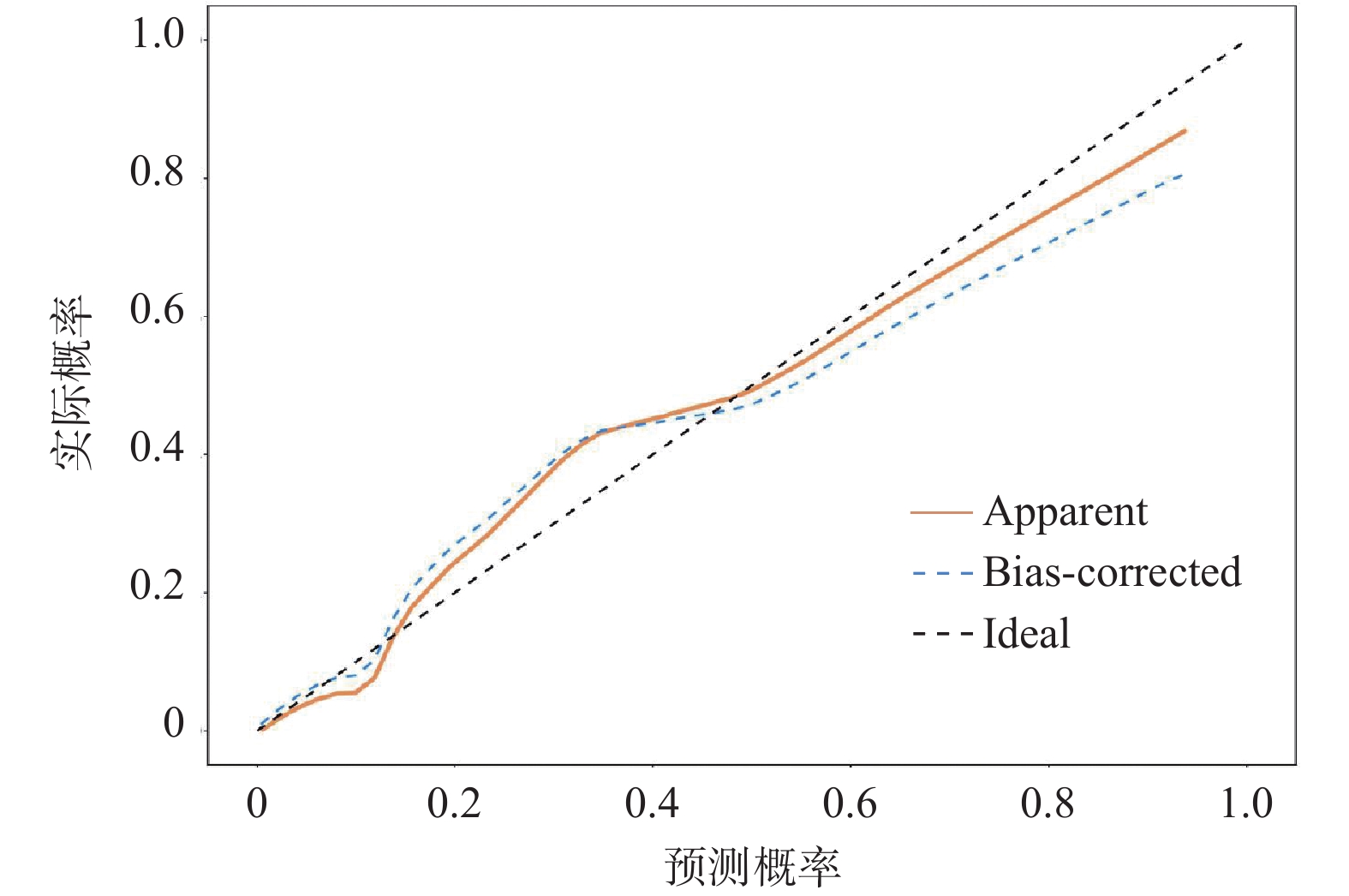
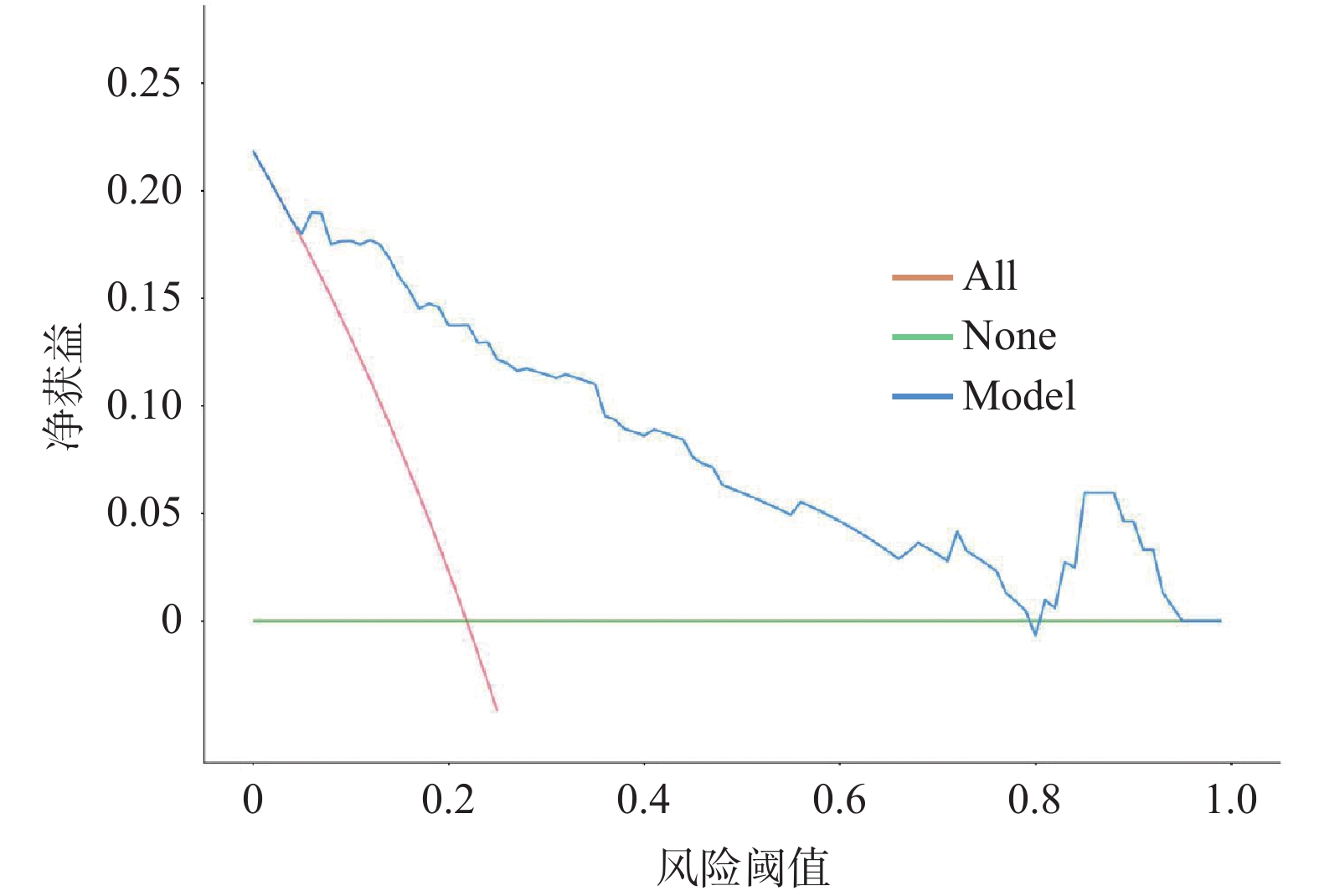
目的 探讨维持性血液透析(maintenance hemodialysis,MHD)患者中心静脉导管相关真菌感染的危险因素,构建风险列线图预测模型,并分析病原菌的分布及耐药特征。 方法 回顾性选取2024年1月至2025年1月于空军军医大学第一附属医院收治的216例行中心静脉置管的MHD患者,根据是否发生导管相关真菌感染分为感染组(n = 54例)和非感染组(n = 162例)。收集两组患者的临床基线资料,采用多因素Logistic回归分析确定真菌感染的独立危险因素,利用R软件构建Nomogram列线图预测模型,结合ROC曲线、校准曲线及决策曲线综合评估模型效能。同时对分离出的54株真菌进行病原学分布及药敏试验分析。 结果 共检出真菌54株,以白假丝酵母菌(44.44%)、热带假丝酵母菌(22.22%)和光滑假丝酵母菌(18.52%)为主;主要感染部位为肺部(44.44%)和泌尿道(27.78%)。多因素Logistic回归分析显示,置管时间、重复置管、抗菌药物使用类别、激素/免疫抑制剂使用史、白细胞计数(white blood cell count,WBC)为MHD患者发生真菌感染的独立危险因素(P < 0.05)。基于上述因素构建的列线图模型预测真菌感染的ROC曲线下面积(area under the curve,AUC)为0.905(95% CI:0.854~0.957);校准曲线显示拟合优度良好(χ2 = 2.689,P = 0.952);决策曲线分析显示,模型在风险阈值0.03~0.90范围内净获益较高,其中最大净获益值为0.12(对应风险阈值0.15)。检出真菌对两性霉素B的敏感率为100.00%,对卡泊芬净和5-氟胞嘧啶的敏感率均为98.15%,对氟康唑(77.78%)和伊曲康唑(75.93%)敏感率相对较低。 结论 置管时间、重复置管、抗菌药物类别、激素/免疫抑制剂使用史及WBC是MHD患者导管相关真菌感染的独立危险因素,基于上述指标构建的列线图模型具有良好的预测价值。感染以白假丝酵母菌为主,需警惕唑类耐药,经验性治疗可优先选用两性霉素B或卡泊芬净。 Abstract:Objective To investigate the risk factors for central venous catheter-related fungal infections in maintenance hemodialysis (MHD) patients, construct a risk nomogram prediction model, and analyze the distribution and drug resistance characteristics of pathogenic fungi.. Methods A retrospective study was conducted on 216 MHD patients with central venous catheterization admitted to the First Affiliated Hospital of Air Force Medical University from January 2024 to January 2025. Patients were divided into an infection group (n = 54) and a non-infection group (n = 162) based on the presence or absence of catheter-related fungal infection. Clinical baseline data were collected from both groups. Multivariate logistic regression analysis was used to identify independent risk factors for fungal infection. A nomogram prediction model was constructed using R software. The model performance was comprehensively evaluated by ROC curve, calibration curve, and decision curves. Simultaneously, pathogenic distribution and antimicrobial susceptibility testing were performed on 54 isolated fungal strains. Results A total of 54 fungal strains were detected, predominantly Candida albicans (44.44%), Candida tropicalis (22.22%), and Candida glabrata (18.52%). The primary infection sites were the lungs (44.44%) and urinary tract (27.78%). Multivariate Logistic regression analysis showed that catheterization duration, repeated catheterization, antimicrobial drug usage category, history of corticosteroid/immunosuppressant use, and white blood cell count(WBC) were independent risk factors for fungal infections in MHD patients (P < 0.05). The nomogram model based on these factors achieved an area under the receiver operating characteristic curve (AUC) of 0.905(95% CI: 0.854~0.957)for predicting fungal infection. The calibration curve demonstrated good goodness of fit (χ2 = 2.689, P = 0.952). Decision curve analysis showed that the model provided high net benefit across risk threshold of 0.03-0.90, with a maximum net benefit of 0.12 (at risk threshold 0.15). Detected fungi demonstrated 100.00% sensitivity to amphotericin B, 98.15% sensitivity to caspofungin and 5-fluorocytosine, while showing relatively lower sensitivity to fluconazole (77.78%) and itraconazole (75.93%). Conclusion Catheterization duration, repeated catheterization, antimicrobial drug category, history of corticosteroid/immunosuppressant use, and WBC are independent risk factors for catheter-related fungal infections in MHD patients. The nomogram model established based on these indicators shows good predictive value. Since Candida albicans is the predominant pathogen, vigilance regarding azole resistance is warranted. Empirical therapy should prioritize amphotericin B or caspofungin. -
Key words:
- Maintenance hemodialysis /
- Central venous catheter /
- Fungal infection /
- Drug resistance /
- Intensive care
-
表 1 病原菌分布及感染部位
Table 1. Distribution of pathogenic bacteria and sites of infection
项目 n 构成比(%) 病原菌 白假丝酵母菌 24 44.44 热带假丝酵母菌 12 22.22 光滑假丝酵母菌 10 18.52 近平滑假丝酵母菌 4 7.41 其他 4 7.41 感染部位 泌尿道 15 27.78 胃肠道 8 14.81 肺部 24 44.44 其他 7 12.96  下载: 导出CSV
下载: 导出CSV
表 2 两组患者临床指标对比
Table 2. Comparison of clinical indicators between the two groups of patients
临床指标 真菌感染组(n=54) 非真菌感染组(n=162) χ2 P 性别 0.026 0.872 男 32(59.26) 98(60.49) 女 22(40.74) 64(39.51) 年龄(岁) 60.14 ± 7.21 58.77 ± 7.26 1.203 0.230 BMI(kg/m2) 22.54 ± 2.10 22.75 ± 2.15 0.625 0.533 原发病类型 0.149 0.928 慢性肾小球肾炎 28(51.85) 88(54.32) 高血压肾病 12(22.22) 36(22.22) 糖尿病肾病 14(25.93) 38(23.46) 置管时间(d) 21.77 ± 3.36 16.03 ± 3.22 11.222* 0.000 MHD时间(年) 3.11 ± 0.65 2.92 ± 0.62 1.927 0.055 重复置管 10.399* 0.001 是 36(66.67) 67(41.36) 否 18(33.33) 95(58.64) 抗菌药物使用类别 10.227* 0.001 ≥ 2 42(77.78) 86(53.09) < 2 12(22.22) 76(46.91) 激素/免疫抑制剂使用史 11.582* 0.001 是 25(46.30) 36(22.22) 否 29(53.70) 126(77.78) 侵入性操作 2.059 0.151 是 30(68.18) 91(56.17) 否 14(31.82) 71(43.83) 既往导管感染史 1.262 0.261 是 25(46.30) 61(37.65) 否 29(53.70) 101(62.35) 导管类型 0.516 0.473 隧道式 34(62.96) 93(57.41) 非隧道式 20(37.04) 69(42.59) 置管部位 0.035 0.852 颈静脉 41(75.93) 125(77.16) 股静脉 13(24.07) 37(22.84) 透析频率(2次/周) 0.165 0.685 是 19(35.19) 57(38.27) 否 35(64.81) 105(61.73) 临床指标 Alb(g/L) 28.45 ± 7.04 30.12 ± 6.85 1.541 0.125 WBC(×109/L) 12.32 ± 4.57 9.52 ± 3.31 4.865* 0.000 Hb(g/L) 95.21 ± 10.63 97.63 ± 11.25 1.388 0.167 PLT(×109/L) 205.44 ± 55.32 216.47 ± 54.68 1.280 0.202 BUN(mmol/L) 22.65 ± 4.57 21.54 ± 4.31 1.614 0.108 Scr(μmol/Ls) 455.47 ± 24.32 448.62 ± 24.51 1.782 0.076 PTH(pg/mL) 316.44 ± 90.36 319.62 ± 88.74 0.227 0.821 注:*P<0.05。
下载: 导出CSV
表 3 自变量赋值说明
Table 3. Assignment of independent variables
自变量 变量说明 赋值 置管时间 连续变量 / 重复置管 分类变量 是=1,否=0 抗菌药物使用类别 分类变量 ≥ 2=1,< 2=0 激素/免疫抑制剂使用史 分类变量 是=1,否=0 WBC 连续变量 /
下载: 导出CSV
表 4 MHD患者中心静脉导管相关真菌感染的多因素Logistic分析
Table 4. Multivariate Logistic regression analysis of central venous catheter-related fungal infection in MHD patients
因素 B SE Wald P OR 95%CI 置管时间 0.471 0.083 5.688 0.000 1.602 1.362~1.885 重复置管 1.042 0.330 9.987 0.002 2.836 1.486~5.413 抗菌药物使用类别 1.129 0.363 9.664 0.002 3.093 1.518~6.303 激素/免疫抑制剂使用史 1.104 0.332 11.067 0.001 3.017 1.574~5.783 WBC 0.198 0.046 18.659 0.000 1.219 1.114~1.334
下载: 导出CSV
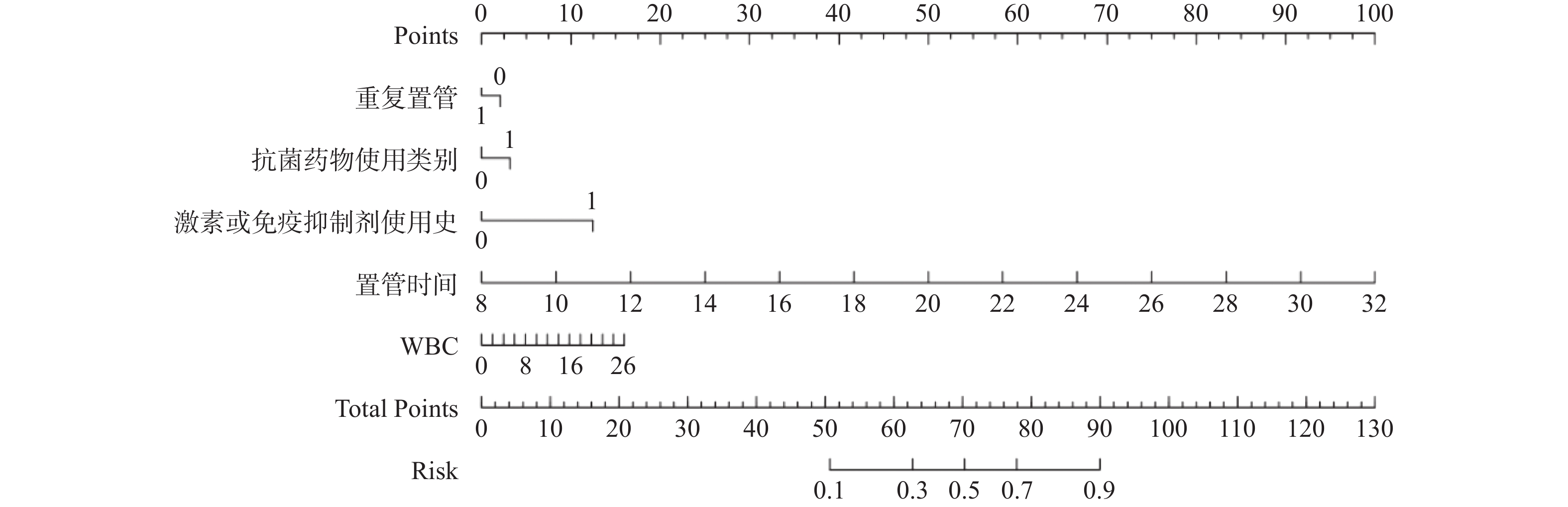
表 5 列线图各影响因素赋分标准表
Table 5. Scoring standards for each influencing factor for the nomogram
影响因素 变量状态 对应分值 备注 置管时间(周) 7 0 置管时间每增加1d,评分增加约4~5 分;
评分基于标准化回归系数线性换算14 32 27 63 28 95 31 100 重复置管 否(0) 0 是(1) 7 抗菌药物使用类别 <2 种(0) 0 ≥2 种(1) 11 激素/免疫抑制剂使用史 否(0) 0 是(1) 7 WBC(×10⁹/L) ≤9.5 0 以临床正常值上限为起点,低于此值风险视为基线;
高于此值后每升高1×10⁹/L 增加约1.3分12 4 15 8 18 12
下载: 导出CSV
表 6 主要真菌菌株对抗真菌药物的敏感及耐药情况[ n(%) ]
Table 6. Sensitivity and drug resistance of major fungal strains to antifungal agents[ n(%) ]
抗菌药物 真菌
(n = 54)白假丝酵母菌
(n = 24)热带假丝酵母菌
(n = 12)光滑假丝酵母菌
(n = 10)近平滑假丝酵母菌
(n = 4)其他
(n = 4)两性霉素B 敏感 54(100.00) 24(100.00) 12(100.00) 10(100.00) 4(100.00) 4(100.00) 耐药 0(100.00)* 0(100.00) 0(100.00) 0(100.00) 0(100.00) 0(100.00) 氟康唑 敏感 42(77.78) 22(91.67) 9(75.00) 5(50.00) 3(75.00) 3(75.00) 耐药 12(22.22) 2(8.33) 3(25.00) 5(50.00) 1(25.00) 1(25.00) 伏立康唑 敏感 48(88.89) 23(95.83) 10(83.33) 8(80.00) 4(100.00) 4(100.00) 耐药 6(11.11) 1(4.17) 2(16.67) 2(20.00) 0(0.00) 0(0.00) 卡泊芬净 敏感 53(98.15) 24(100.00) 12(100.00) 9(90.00) 4(100.00) 4(100.00) 耐药 1(1.85)# 0(0.00) 0(0.00) 1(10.00) 0(0.00) 0(0.00) 伊曲康唑 敏感 41(75.93) 21(87.50) 8(66.67) 6(60.00) 3(75.00) 3(75.00) 耐药 13(24.07) 3(12.50) 4(33.33) 4(40.00) 1(25.00) 1(25.00) 5-氟胞嘧啶 敏感 53(98.15) 23(95.83) 12(100.00) 10(100.00) 4(100.00) 4(100.00) 耐药 1(1.85)# 1(4.17) 0(0.00) 0(0.00) 0(0.00) 0(0.00) 注:*P < 0.05表示为两性霉素B分别与3种唑类药物(氟康唑、伏立康唑、伊曲康唑)耐药率比较;#P < 0.05表示为卡泊芬净和5-氟胞嘧啶分别与氟康唑、伊曲康唑耐药率比较。
下载: 导出CSV
-
[1] Cheng M, He M, Ning L, et al. Association between frailty and adverse outcomes in patients undergoing maintenance hemodialysis: A systematic review and meta-analysis[J]. Ren Fail, 2024, 46(2): 2367716. doi: 10.1080/0886022X.2024.2367716 [2] 马遥, 郜同心, 彭彦平, 等. MHD患者发生CAADVT的影响因素分析及风险评估模型构建[J]. 中国医药导刊, 2025, 27(10): 1066-1070. [3] Li X, Yu B, Li H, et al. Drug clues for the treatment of fungal catheter-related bloodstream infection with antifungal lock therapy[J]. Drug Des Dev Ther, 2025, 19: 683-701. doi: 10.2147/DDDT.S501664 [4] Bond A, Kopczynska M, Conley T, et al. Long-term survival following fungal catheter-related bloodstream infection for patients with intestinal failure receiving home parenteral support[J]. J Parenter Enteral Nutr, 2023, 47(1): 159-164. doi: 10.1002/jpen.2451 [5] 赵令君, 刘玉峰, 吴淋淋, 等. 糖尿病肾病最新国际病理诊断标准的临床应用研究[J]. 中国实验诊断学, 2014(5): 847-848. [6] 中国中西医结合学会肾脏疾病专业委员会. 慢性肾衰竭中西医结合诊疗指南[J]. 中国中西医结合杂志, 2015, 35(9): 313-317. [7] 中国医师协会血液科医师分会, 中国侵袭性真菌感染工作组. 血液病/恶性肿瘤患者侵袭性真菌病的诊断标准与治疗原则(第七次修订版)[J]. 中华内科杂志, 2025, 64(12): 1155-1168. doi: 10.3760/cma.j.cn112138-20250808-00468 [8] 崔丽红, 孙长喜, 师军华. 维持血液透析患者中心静脉导管相关血流感染影响因素及肿瘤坏死因子-α基因多态性[J]. 中华医院感染学杂志, 2023, 33(9): 1333-1337. doi: 10.11816/cn.ni.2023-221526 [9] 中华人民共和国卫生部医政司. 全国临床检验操作规程(第3版)(精)[M]. 南京: 东南大学出版社, 2006: 571. [10] 林洪丽. 中心静脉导管血栓的防治[J]. 肾脏病与透析肾移植杂志, 2024, 33(3): 239-240. doi: 10.3969/j.issn.1006-298X.2024.03.007 [11] 陈倩, 钟清, 李曼丽, 等. 维持性血液透析患者并发真菌感染的危险因素及耐药性分析[J]. 临床肾脏病杂志, 2021, 21(2): 147-152. [12] 陶玮, 李红波, 李红兵, 等. 维持性血液透析患者导管相关性感染影响因素及其列线图预测模型构建[J]. 中华医院感染学杂志, 2024, 34(19): 3022-3025. [13] 祁奇, 董浩楠, 李亚娟. 采用自体动静脉内瘘维持性血液透析患者真菌感染的菌种分布及相关易感因素研究[J]. 中国真菌学杂志, 2025, 20(2): 159-165. doi: 10.3969/j.issn.1673-3827.2025.02.010 [14] 宋洁妮, 戚超翔, 朱琳, 等. 慢性肾衰竭维持性血液透析患者肺部感染病原菌及其危险因素模型构建[J]. 中华医院感染学杂志, 2024, 34(7): 993-997. doi: 10.11816/cn.ni.2024-231140 [15] He Y, Jiang H, Huang X, et al. Solutions to stuck tunneled cuffed catheters in patients undergoing maintenance hemodialysis[J]. J Vasc Access, 2021, 22(2): 203-208. doi: 10.1177/1129729820928163 [16] 张在卉, 吕园园, 王志红. 多囊肾病患者的致病基因变异分析[J]. 昆明医科大学学报, 2026, 47: 1-8. [17] 庞婷, 吴伟莉, 杨斌姣. 维持性血液透析患者导管相关感染的病原菌情况、危险因素与预测模型构建[J]. 实用临床医药杂志, 2024, 28(21): 60-65. [18] 龙颂, 李甫良, 杨金有, 等. 血清超敏C反应蛋白、降钙素原及白细胞计数检测对维持性血液透析合并感染的诊断价值[J]. 中国血液净化, 2024, 23(8): 601-604. doi: 10.3969/j.issn.1671-4091.2024.08.006 [19] 张炎, 高志伟, 廉秀花, 等. 维持性血液透析患者导管相关性血流感染发生季节、病原菌特点及药敏分析[J]. 中国血液净化, 2024, 23(12): 943-946. [20] 何国念, 金永梅, 田波, 等. HIV/AIDS患者血液透析状态下的精神障碍及临床特征调查[J]. 昆明医科大学学报, 2026, 47(1): 70-78. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 13
- HTML全文浏览量: 8
- PDF下载量: 1
- 被引次数: 0
