

The Predictive Value of sFlt-1,SDC4,and sST2 on the Therapeutic Effect of Children with Purpuric Nephritis
-
摘要:
目的 探讨紫癜性肾炎(henoch-schnlein purpura nephritis,HSPN)患儿血清可溶性血管内皮生长因子受体-1(soluble vascular endothelial growth factor receptor-1,sFlt-1)、多配体蛋白聚糖-4(polyligand proteoglycan-4,SDC4)、可溶性人基质裂解素2(soluble human stromal lysin 2,sST2)水平与肾组织病理分级相关性,并分析其对治疗效果的预测价值。 方法 回顾性选取2021年4月至2023年4月信阳一五四医院收治的98例HSPN患儿作为研究对象,依据治疗2个月后临床疗效分为有效组(n=78)和无效组(n=20),比较其临床资料及治疗前、治疗1个月后血清sFlt-1、SDC4、sST2水平。多因素Logistic回归分析疗效影响因素。分析治疗1个月后血清sFlt-1、SDC4、sST2水平对治疗2个月后疗效的预测价值。 结果 随着病理分级增加,血清sFlt-1、SDC4、sST2水平呈上升趋势(P < 0.05);无效组治疗1个月后血清sFlt-1、SDC4、sST2水平高于有效组(P < 0.05);紫癜症状评分、免疫球蛋白A(immunoglobulin A,IgA)水平及治疗1个月后血清sFlt-1、SDC4、sST2水平为疗效的独立危险因素(P < 0.05);治疗1个月后血清sFlt-1、SDC4、sST2水平联合预测疗效的AUC大于任意2项联合预测、单项指标预测(P < 0.05)。 结论 HSPN患儿血清sFlt-1、SDC4、sST2水平与肾脏组织病理分级密切相关,联合检测其水平对治疗效果具有一定预测价值。 -
关键词:
- 紫癜性肾炎 /
- 可溶性血管内皮生长因子受体-1 /
- 多配体蛋白聚糖-4 /
- 可溶性人基质裂解素2 /
- 预测
Abstract:Objective To investigate the correlation between the levels of soluble vascular endothelial growth factor receptor-1 (sFlt-1), polyligand proteoglycan-4 (SDC4), soluble human stromal lysin 2 (sST2) in serum and renal histopathological grading in children with Henoch-Schnlein purpura nephritis (HSPN), and analyze their predictive value for therapeutic efficacy. Methods A retrospective study was conducted, in which 98 children with HSPN admitted to Xinyang 154th Hospital from April 2021 to April 2023 were selected as the research subjects. According to the clinical efficacy after 2 months of treatment, they were divided into an effective group of 78 cases and an ineffective group of 20 cases. Their clinical data and the levels of serum sFlt-1, SDC4, and sST2 before and after treatment were compared. Multivariate logistic regression analysis was used to analyze the factors affecting the efficacy. The predictive value of serum sFlt-1, SDC4, and sST2 levels after 1 month of treatment on the efficacy after 2 months of treatment was analyzed. Results As the pathological grade increased, the levels of serum sFlt-1, SDC4, and sST2 showed an upward trend (P < 0.05); the levels of serum sFlt-1, SDC4, and sST2 in the ineffective group after 1 month of treatment were higher than those in the effective group (P < 0.05); the symptom score of purpura, immunoglobulin A (IgA) level, and the levels of serum sFlt-1, SDC4, and sST2 after 1 month of treatment were independent risk factors for efficacy (P < 0.05); the AUC of serum sFlt-1, SDC4, and sST2 levels combined to predict efficacy after 1 month of treatment was greater than that of any two combined predictions or single indicator predictions (P < 0.05). Conclusion The levels of serum sFlt-1, SDC4, and sST2 in children with HSPN are closely related to the pathological grading of the kidney tissue. The combined detection of their levels has certain predictive value for the therapeutic effect. -
紫癜性肾炎(henoch-schnlein purpura nephritis,HSPN)属于毛细血管变态反应性疾病,其为过敏性紫癜(henoch schonlein purpura,HSP)并发症,临床表现为皮肤紫癜、发热、头痛、关节肿痛、蛋白尿等,HSP发病后4周内约有90%患者发生HSPN,且发病率呈逐年上升趋势[1]。临床常采用泼尼松、他克莫司等药物联合治疗,但仍有部分患儿治疗效果不佳,寻找HSPN患儿疗效相关指标对临床制定治疗方案具有重要意义。
可溶性血管内皮生长因子受体-1 (soluble vascular endothelial growth factor receptor-1,sFlt-1)是由近端肾小管细胞等部位分泌,可结合血管内皮生长因子,引起血管生成障碍,并可诱发肾毛细血管丛炎性反应,造成小血管壁损伤,促使蛋白尿生成[2]。多配体蛋白聚糖-4(polyligand proteoglycan-4,SDC4)属于Ⅰ型跨膜蛋白,主要存在于内皮细胞、足细胞,可调节信号转导通路,促进细胞外基质黏附,参与肾脏疾病发生发展过程[3]。可溶性人基质裂解素2(soluble human stromal lysin 2,sST2)属于白细胞介素-1受体(interleukin-1 receptor,IL-1R)家族成员,可调节白细胞介素-33(interleukin-33,IL-33)/人基质裂解素2(human stromal lysin 2,ST2)轴诱导炎性细胞因子/趋化因子释放,参与急性肾损伤、糖尿病肾病等多种疾病发生发展过程[4]。但sFlt-1、SDC4、sST2与HSPN相关研究报道鲜少,因此,本研究通过观察HSPN患儿血清sFlt-1、SDC4、sST2水平与肾脏病理分级相关性,并探究其对治疗效果的预测价值,旨在为临床治疗提供参考。
1. 资料与方法
1.1 研究对象
回顾性选取2021年4月至2023年4月信阳一五四医院收治的98例HSPN患儿作为研究对象,病理分级:Ⅰ级15例(轻微病变)、Ⅱ级38例(系膜增生)、 Ⅲ级31例(系膜增生且形成肾小球新月≤50%)、 Ⅳ级14例(系膜增生且50%<肾小球新月≤70%,伴有节段损害)。本研究经信阳一五四医院伦理委员会批准(20240409)。
1.2 纳入和排除标准
1.2.1 纳入标准[5]
(1)符合HSPN诊断标准[6]:HSP发病6个月内出现血尿或蛋白尿;(2)首次发病;(3)入院前1个月内未使用免疫抑制剂、抗组胺药等药物治疗;(4)既往无糖尿病等代谢性疾病史;(5)既往无家族肾脏遗传性疾病史;(6)病历资料完整。
1.2.2 排除标准[7]
(1)伴有心脑等重要脏器功能障碍者;(2)合并系统性红斑狼疮、自身免疫缺陷疾病;(3)伴有肾脏外伤;(4)入院前1个月内患有呼吸道感染、胃肠道感染性疾病;(5)合并肾病综合征等原发性或继发性肾病;(6)凝血功能严重障碍者。
1.3 研究方法
1.3.1 治疗方案与疗效判定
研究组患儿予以常规治疗,包括口服泼尼松(黑龙江鼎恒升药业有限公司,国药准字H20046457),每日剂量为0.5 mg/kg、他克莫司(杭州中美华东制药有限公司,国药准字H20084514),每日剂量为0.1 mg/kg, 静脉滴注环磷酰胺(哈尔滨三联药业股份有限公司,国药准字H20084196),剂量为:750 mg/m2,0.9%氯化钠注射液100 mL稀释后静脉滴注,总剂量为1 g,1次/月,连续治疗2个月。依据治疗2个月后临床疗效分为有效组78例、无效组20例,疗效判定[8]:完全缓解:尿蛋白、血尿症状消失,尿/血常规检查结果正常,红细胞<3个;部分缓解:血尿症状明显改善,24 h尿蛋白量降低幅度≥50%,尿红细胞计数降低幅度≥50%;无效:未达到上述标准,完全缓解、部分缓解视为有效,否则视为无效。
1.3.2 检测血清sFlt-1、SDC4、sST2水平
研究对象于治疗前、治疗1个月后采集空腹外周静脉血5 mL,速度为
3500 r/min离心10 min(离心半径10 cm)分离血清,ELISA法检测血清SDC4、sFlt-1、sST2水平(南京森贝咖生物公司)。1.3.3 收集临床资料
通过查阅电子病历档案、门诊实验室检查项目等收集临床资料,包括性别、年龄、体质量指数、病理分级、D-二聚体、凝血酶原时间、纤维蛋白原、活化部分凝血时间、CD3+、CD4+、CD8+、24 h尿蛋白含量、尿红细胞计数、呼吸道病原体感染、EB病毒感染、免疫球蛋白A(Immunoglobulin A,IgA)、免疫球蛋白G(Immunoglobulin G,IgG)、紫癜症状评分[9],采用TSA9000C全自动凝血分析仪(上海寰熙医疗器械有限公司)检测D-二聚体、凝血酶原时间、纤维蛋白原、活化部分凝血时间,免疫荧光标记法检测CD3+、CD4+、CD8+水平,ELISA法检测血清IgA、IgG水平,双缩脲法检测24 h尿蛋白含量,使用BX43显微镜(上海门季生物科技有限公司)检测尿红细胞计数。
1.4 观察指标
(1)对比分析不同病理分级患儿(入院时)血清sFlt-1、SDC4、sST2水平变化;(2)分析有效、无效患儿治疗前、治疗1个月后血清sFlt-1、SDC4、sST2水平;(3)多因素分析疗效的影响因素;(4)评价治疗1个月后血清sFlt-1、SDC4、sST2水平对治疗2个月后疗效的预测效能。
1.5 统计学处理
数据整理后正态分布检验,每组数据均满足正态分布,组间比较采用独立样本t检验,组内比较采用配对t检验,多组间比较采用单因素方差分析,组间两两比较采用SNK-q检验;影响因素分析用多因素Logistic回归;采用MedCalc18.2绘制受试者工作特征曲线(receiver operating characteristic,ROC)并计算曲线下面积(area under curve,AUC),采用Z检验对比模型AUC差异;用SPSS26.0统计软件处理,检验标准P < 0.05。
2. 结果
2.1 不同病理分级HSPN患儿血清sFlt-1、SDC4、sST2水平比较
HSPN患儿随着病理分级增加,血清sFlt-1、SDC4、sST2水平呈上升趋势,两两比较,差异均有统计学意义(P < 0.05),见表1。
表 1 不同病理分级患儿血清sFlt-1、SDC4、sST2水平比较($\bar x \pm s $)Table 1. Comparison of serum sFlt-1,SDC4,and sST2 levels in children with different pathologic grades ($\bar x \pm s $)组别 n sFlt-1(pg/mL) SDC4(ng/mL) sST2(pg/mL) Ⅰ级 15 411.63 ± 107.21 11.30 ± 3.02 1085.36 ± 221.78Ⅱ级 38 786.34 ± 162.15* 17.52 ± 2.16* 1574.29 ± 224.76*Ⅲ级 31 1263.35 ± 250.87*#25.63 ± 3.57*# 2065.34 ± 262.67*#Ⅳ级 14 2069.95 ± 319.98*#&42.42 ± 3.14*#& 3692.73 ± 330.91*#&F 177.889 335.403 308.121 P <0.001 <0.001 <0.001 与Ⅰ级比较,*P < 0.05;与Ⅱ级比较,#P < 0.05;与Ⅲ级比较,&P < 0.05。 2.2 有效与无效患儿临床资料比较
无效组24 h尿蛋白含量、尿红细胞计数、紫癜症状评分及IgA水平高于有效组,差异有统计学意义(P < 0.05),见表2。
表 2 有效与无效患儿临床资料比较[($\bar x \pm s $)/n(%)]Table 2. Comparison of clinical data of effective and ineffective children [($\bar x \pm s $)/n(%)]临床资料 无效(n=20) 有效(n=78) t/χ2 P 性别 0.013 0.910 男 11(55.00) 44(56.41) 女 9(45.00) 34(43.59) 年龄(岁) 8.63±1.17 9.02±1.06 1.437 0.154 体质量指数(kg/m2) 17.55±2.03 18.28±1.75 1.610 0.111 病理分级 0.730 0.866 Ⅰ级 4(20.00) 11(14.10) Ⅱ级 8(40.00) 30(38.46) Ⅲ级 5(25.00) 26(33.33) Ⅳ级 3(15.00) 11(14.10) D-二聚体(μg/L) 60.33±5.24 61.02±5.74 0.488 0.627 凝血酶原时间(s) 8.62±1.63 8.71±1.77 0.206 0.837 纤维蛋白原(g/L) 12.82±1.27 12.71±1.33 0.333 0.740 活化部分凝血时间(s) 15.06±2.11 14.92±2.17 0.259 0.796 CD3+(%) 52.16±5.24 53.11±4.19 0.858 0.393 CD4+(%) 25.99±3.21 25.94±3.14 0.063 0.950 CD8+(%) 27.45±3.16 27.61±3.02 0.209 0.835 24 h尿蛋白含量(mg) 942.61±114.20 878.52±122.84 2.110 0.037 尿红细胞计数(个/μL) 226.31±30.21 201.74±27.24 3.520 0.001* 呼吸道病原体感染 0.699 0.403 有 13(65.00) 58(74.36) 无 7(35.00) 20(25.64) EB病毒感染 0.009 0.926 有 9(45.00) 36(46.15) 无 11(55.00) 42(53.85) IgA(g/L) 2.55±0.52 1.68±0.36 8.747 <0.001* IgG(g/L) 9.06±2.02 8.87±2.15 0.357 0.722 紫癜症状评分(分) 7.58±1.52 5.61±1.17 6.303 <0.001* *P < 0.05。 2.3 有效与无效HSPN患儿血清sFlt-1、SDC4、sST2水平比较
治疗1个月后,无效组血清sFlt-1、SDC4、sST2水平高于有效组,差异均有统计学意义(P < 0.05),见表3。
表 3 有效与无效患儿血清sFlt-1、SDC4、sST2水平比较($\bar x \pm s $)Table 3. Comparison of serum sFlt-1,SDC4 and sST2 levels between effective and ineffective children($\bar x \pm s $)组别 n sFlt-1(pg/mL) SDC4(ng/mL) sST2(pg/mL) 治疗前 治疗1个月后 治疗前 治疗1个月后 治疗前 治疗1个月后 无效 20 1055.96 ± 251.98635.25 ± 111.75* 23.01 ± 4.67 16.03 ± 3.34* 1988.54 ± 362.871563.29 ± 321.11*有效 78 1065.12 ± 255.04502.31 ± 127.43* 22.61 ± 6.53 11.08 ± 3.29* 1949.44 ± 349.811165.49 ± 368.46*t 0.144 4.261 0.257 5.985 0.443 4.414 P 0.886 <0.001 0.798 <0.001 0.659 <0.001 与同组治疗前比较,*P < 0.05。 2.4 多因素分析
以治疗效果为因变量(有效=0、无效=1),以24 h尿蛋白含量、尿红细胞计数、紫癜症状评分、IgA水平及治疗1个月后血清sFlt-1、SDC4、sST2水平为自变量,校正紫癜症状评分、IgA水平等其他因素后,多因素Logistic回归分析显示治疗1个月后血清sFlt-1、SDC4、sST2水平仍为疗效的影响因素(P < 0.05),见表4。
表 4 多因素分析Table 4. Multi-factor analysis影响因素 β S.E. Waldχ2 P OR 95%CI sFlt-1 1.404 0.626 5.027 <0.001* 4.070 2.014~8.224 SDC4 1.694 0.574 8.714 <0.001* 5.443 3.215~9.216 sST2 2.097 0.613 11.707 <0.001* 8.145 2.574~10.013 24 h尿蛋白含量、尿红细胞计数、紫癜症状评分、IgA及治疗1个月后血清sFlt-1、SDC4、sST2水平均设为实测值。*P < 0.05。 2.5 ROC分析血清sFlt-1、SDC4、sST2水平对疗效的预测价值
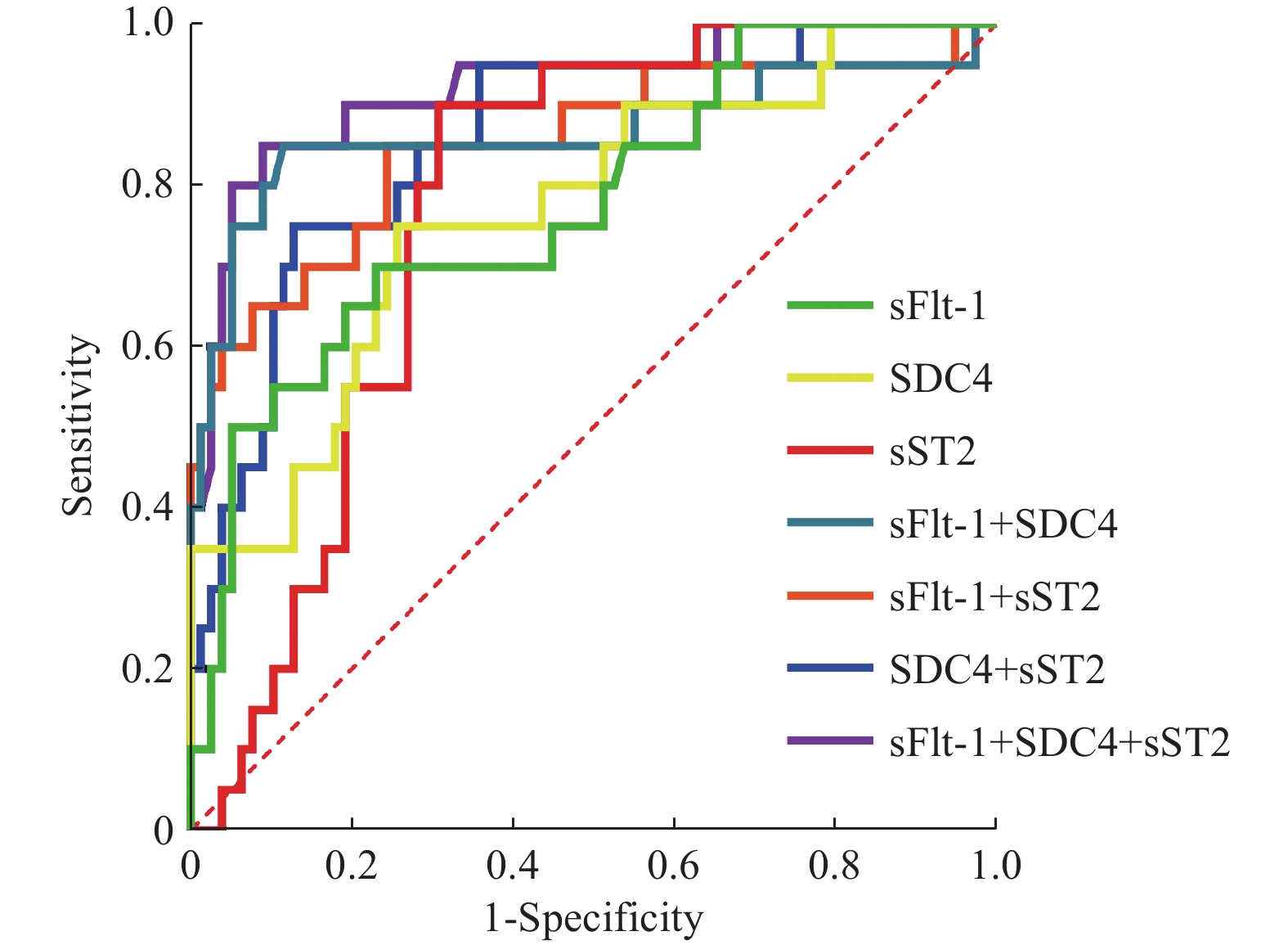
以无效组20例为阳性样本,以有效组78例为阴性样本,ROC分析显示,治疗1个月后血清sFlt-1、SDC4、sST2水平联合预测疗效的AUC大于任意2项联合预测、单项指标预测(P < 0.05),见表5、图1。
表 5 ROC分析血清sFlt-1、SDC4、sST2水平对疗效的预测价值Table 5. Predictive value of serum sFlt-1,SDC4,and sST2 levels for efficacy by ROC analysis指标 AUC 95%CI cut-off 敏感度(%) 特异度(%) P sFlt-1(pg/mL) 0.776 0.681~0.854 >588.9 70.00 76.92 <0.001* SDC4(ng/mL) 0.769 0.673~0.848 >21.2 75.00 74.36 <0.001* sST2(pg/mL) 0.774 0.679~0.853 > 1366.84 90.00 69.23 <0.001* sFlt-1+SDC4 0.867 0.783~0.927 − 85.00 88.46 <0.001* sFlt-1+sST2 0.852 0.766~0.916 − 85.00 75.64 <0.001* SDC4+sST2 0.858 0.773~0.921 − 75.00 87.18 <0.001* sFlt-1+SDC4+sST2 0.923 0.851~0.967 − 85.00 91.03 <0.001* *P < 0.05。 3. 讨论
3.1 HSPN病理机制
HSPN病理基础为病原体感染、过敏等导致IgA或IgG类循环免疫复合物沉积于细小动脉/毛细血管,其发病机制可能与免疫-炎性反应、肾小球内皮细胞损伤、微血栓形成、肾小球内纤维蛋白沉积等有关[10]。
3.2 sFlt-1与HSPN相关性机制
sFlt-1可结合血管内皮生长因子引起内皮细胞损伤,改变血管壁通透性/完整性,促使血小板黏附及聚集,诱发肾组织损伤,导致蛋白尿排出[11]。本研究结果显示,随着病理分级增加,血清sFlt-1水平呈上升趋势,与既往结果相似[12],提示sFlt-1水平升高可能参与HSPN发生过程。原因可能为sFlt-1水平升高可引起内皮细胞损伤,促使血小板聚集、黏附及血栓形成,改变肾脏微血管结构及功能,引起肾组织缺血或低灌注,造成肾脏损伤,进而参与HSPN发生过程;同时sFlt-1水平升高可诱导肾小球系膜细胞、肾小管上皮细胞分泌炎性因子,引起凝血纤溶系统紊乱。
3.3 SDC4与HSPN相关性机制
SDC4可调节瞬时受体电位阳离子通道蛋白6表达,促使钙离子内流,引起足细胞结构/功能障碍,并可激活肾小管上皮细胞转化生长因子-β1,促进炎性因子表达,促使肾间质纤维化、肾小球硬化,进而参与肾脏疾病发生发展过程[13]。本研究发现SDC4水平升高与病理分级密切相关,与既往研究结果相似[14],提示SDC4可能参与HSPN发生发展过程。原因可能为SDC4水平升高可刺激肾组织炎性增生/纤维化,破坏小血管结构/功能,造成肾组织缺血缺氧,引起肾小血管损伤,并可介导细胞与细胞外基质蛋白接触,干扰足突细胞-基质相互作用,进而加重肾组织损伤程度。
3.4 sST2与HSPN相关性机制
sST2可抑制细胞核因子κ B、丝裂原活化蛋白激酶激活,引起免疫-炎性反应,其水平随着肾脏疾病严重程度加重而上升,且为肾脏疾病预后不良的危险因素[15−16]。本研究中HSPN患儿血清sST2水平升高与病理分级密切相关。任宏伟等[17]研究表明HSP患儿血清sST2水平升高,且与HSP病情进展密切相关,这支持本研究结论。其原因可能为sST2水平升高可引起免疫系统紊乱,促使炎性细胞因子生成量增加,诱导细胞外基质沉积,增加免疫复合物沉积,造成肾脏损伤。
3.5 sFlt-1、SDC4、sST2与HSPN疗效相关性及其对疗效的预测价值
本研究结果显示,治疗1个月后,无效组血清sFlt-1、SDC4、sST2水平高于有效组,且经多因素分析显示紫癜症状评分、IgA水平及治疗1个月后血清sFlt-1、SDC4、sST2水平为疗效的独立危险因素,提示sFlt-1、SDC4、sST2水平升高与HSPN患儿治疗效果密切相关。可能原因为HSPN患儿治疗后sFlt-1、SDC4、sST2水平升高可促使肾小血管周围炎性因子聚集增多,引起血管炎性损害,并可促进肾小球细胞外基质合成,引起肾纤维化、肾小球硬化,促使肾小球滤过功能异常,进而增加无效发生风险。既往研究表明血清sFlt-1、SDC4、sST2水平变化对多种疾病预后具有一定预测价值[18-20]。但血清sFlt-1、SDC4、sST2水平变化对HSPN患儿治疗效果的预测价值尚未明确。本研究经ROC分析发现治疗1个月后血清sFlt-1、SDC4、sST2水平联合预测疗效的AUC大于任意2项联合预测、单项指标预测,提示早期检测血清sFlt-1、SDC4、sST2水平可能用于预测HSPN患儿治疗效果。
综上所述,HSPN患儿血清sFlt-1、SDC4、sST2水平升高与肾脏组织病理分级密切相关,且为无效的独立危险因素,联合检测其水平可能作为临床预测疗效的潜在指标,有助于指导早期治疗方案的调整,以提高临床疗效。
-
表 1 不同病理分级患儿血清sFlt-1、SDC4、sST2水平比较($\bar x \pm s $)
Table 1. Comparison of serum sFlt-1,SDC4,and sST2 levels in children with different pathologic grades ($\bar x \pm s $)
组别 n sFlt-1(pg/mL) SDC4(ng/mL) sST2(pg/mL) Ⅰ级 15 411.63 ± 107.21 11.30 ± 3.02 1085.36 ± 221.78Ⅱ级 38 786.34 ± 162.15* 17.52 ± 2.16* 1574.29 ± 224.76*Ⅲ级 31 1263.35 ± 250.87*#25.63 ± 3.57*# 2065.34 ± 262.67*#Ⅳ级 14 2069.95 ± 319.98*#&42.42 ± 3.14*#& 3692.73 ± 330.91*#&F 177.889 335.403 308.121 P <0.001 <0.001 <0.001 与Ⅰ级比较,*P < 0.05;与Ⅱ级比较,#P < 0.05;与Ⅲ级比较,&P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 有效与无效患儿临床资料比较[($\bar x \pm s $)/n(%)]
Table 2. Comparison of clinical data of effective and ineffective children [($\bar x \pm s $)/n(%)]
临床资料 无效(n=20) 有效(n=78) t/χ2 P 性别 0.013 0.910 男 11(55.00) 44(56.41) 女 9(45.00) 34(43.59) 年龄(岁) 8.63±1.17 9.02±1.06 1.437 0.154 体质量指数(kg/m2) 17.55±2.03 18.28±1.75 1.610 0.111 病理分级 0.730 0.866 Ⅰ级 4(20.00) 11(14.10) Ⅱ级 8(40.00) 30(38.46) Ⅲ级 5(25.00) 26(33.33) Ⅳ级 3(15.00) 11(14.10) D-二聚体(μg/L) 60.33±5.24 61.02±5.74 0.488 0.627 凝血酶原时间(s) 8.62±1.63 8.71±1.77 0.206 0.837 纤维蛋白原(g/L) 12.82±1.27 12.71±1.33 0.333 0.740 活化部分凝血时间(s) 15.06±2.11 14.92±2.17 0.259 0.796 CD3+(%) 52.16±5.24 53.11±4.19 0.858 0.393 CD4+(%) 25.99±3.21 25.94±3.14 0.063 0.950 CD8+(%) 27.45±3.16 27.61±3.02 0.209 0.835 24 h尿蛋白含量(mg) 942.61±114.20 878.52±122.84 2.110 0.037 尿红细胞计数(个/μL) 226.31±30.21 201.74±27.24 3.520 0.001* 呼吸道病原体感染 0.699 0.403 有 13(65.00) 58(74.36) 无 7(35.00) 20(25.64) EB病毒感染 0.009 0.926 有 9(45.00) 36(46.15) 无 11(55.00) 42(53.85) IgA(g/L) 2.55±0.52 1.68±0.36 8.747 <0.001* IgG(g/L) 9.06±2.02 8.87±2.15 0.357 0.722 紫癜症状评分(分) 7.58±1.52 5.61±1.17 6.303 <0.001* *P < 0.05。
下载: 导出CSV
表 3 有效与无效患儿血清sFlt-1、SDC4、sST2水平比较($\bar x \pm s $)
Table 3. Comparison of serum sFlt-1,SDC4 and sST2 levels between effective and ineffective children($\bar x \pm s $)
组别 n sFlt-1(pg/mL) SDC4(ng/mL) sST2(pg/mL) 治疗前 治疗1个月后 治疗前 治疗1个月后 治疗前 治疗1个月后 无效 20 1055.96 ± 251.98635.25 ± 111.75* 23.01 ± 4.67 16.03 ± 3.34* 1988.54 ± 362.871563.29 ± 321.11*有效 78 1065.12 ± 255.04502.31 ± 127.43* 22.61 ± 6.53 11.08 ± 3.29* 1949.44 ± 349.811165.49 ± 368.46*t 0.144 4.261 0.257 5.985 0.443 4.414 P 0.886 <0.001 0.798 <0.001 0.659 <0.001 与同组治疗前比较,*P < 0.05。
下载: 导出CSV
表 4 多因素分析
Table 4. Multi-factor analysis
影响因素 β S.E. Waldχ2 P OR 95%CI sFlt-1 1.404 0.626 5.027 <0.001* 4.070 2.014~8.224 SDC4 1.694 0.574 8.714 <0.001* 5.443 3.215~9.216 sST2 2.097 0.613 11.707 <0.001* 8.145 2.574~10.013 24 h尿蛋白含量、尿红细胞计数、紫癜症状评分、IgA及治疗1个月后血清sFlt-1、SDC4、sST2水平均设为实测值。*P < 0.05。
下载: 导出CSV
表 5 ROC分析血清sFlt-1、SDC4、sST2水平对疗效的预测价值
Table 5. Predictive value of serum sFlt-1,SDC4,and sST2 levels for efficacy by ROC analysis
指标 AUC 95%CI cut-off 敏感度(%) 特异度(%) P sFlt-1(pg/mL) 0.776 0.681~0.854 >588.9 70.00 76.92 <0.001* SDC4(ng/mL) 0.769 0.673~0.848 >21.2 75.00 74.36 <0.001* sST2(pg/mL) 0.774 0.679~0.853 > 1366.84 90.00 69.23 <0.001* sFlt-1+SDC4 0.867 0.783~0.927 − 85.00 88.46 <0.001* sFlt-1+sST2 0.852 0.766~0.916 − 85.00 75.64 <0.001* SDC4+sST2 0.858 0.773~0.921 − 75.00 87.18 <0.001* sFlt-1+SDC4+sST2 0.923 0.851~0.967 − 85.00 91.03 <0.001* *P < 0.05。
下载: 导出CSV
-
[1] 秦艳妮,党清华,景芳丽,等. 过敏性紫癜肾炎患儿血清IL-16、IL-18、IGF-1及IGFBP-3水平变化及临床意义[J]. 海南医学,2020,31(1):31-34. doi: 10.3969/j.issn.1003-6350.2020.01.009 [2] 代彦林,韩姗姗,丁樱,等. 清热止血方联合雷公藤多苷治疗儿童紫癜性肾炎疗效及其对血清sFlt-1、vWF的影响[J]. 中国中医基础医学杂志,2022,28(8):1296-1299. doi: 10.3969/j.issn.1006-3250.2022.8.zgzyjcyx202208025 [3] Tang R, Lin W, Shen C J, et al. Single-cell transcriptomics uncover hub genes and cell-cell crosstalk in patients with hypertensive nephropathy[J]. Int Immunopharmacol,2023,125(1):111104-111114. [4] Moreau A,Nicaise C,Awada A,et al. Soluble ST2 is increased in systemic lupus erythematous and is a potential marker of lupus nephritis[J]. Clin Exp Rheumatol,2022,40(5):897-903. [5] 何传梅, 刘锦秀, 韩红, 等. 雷公藤多苷治疗紫癜性肾炎患儿的疗效和安全性分析[J]. 世界中医药,2020,15(20):3094-3096. [6] 中华医学会儿科学分会肾脏学组. 紫癜性肾炎诊治循证指南(2016)[J]. 中华儿科杂志,2017,55(9):647-651. doi: 10.3760/cma.j.issn.0578-1310.2017.09.003 [7] 陈宾, 邢舒旺, 陈东旭, 等. 肾炎康复片对紫癜性肾炎患儿的临床疗效分析以及对IL-17和IL-10因子的影响[J]. 中国中西医结合肾病杂志,2020,21(7):603-604. [8] 张致远,高振中. 肾炎康复片对过敏性紫癜肾炎患儿血清及尿MCP-1、TGF-β1水平的影响[J]. 国际医药卫生导报,2019,25(4):606-610. doi: 10.3760/cma.j.issn.1007-1245.2019.04.033 [9] Fessatou S,Nicolaidou P,Gourgiotis D,et al. Endothelin 1 levels in relation to clinical presentation and outcome of Henoch Schonlein purpura[J]. BMC Pediatr,2008,8(1):33-43. doi: 10.1186/1471-2431-8-33 [10] Kurokawa M,Maehara K,Kaku Y,et al. Necessity and choice of therapy for Henoch-Schönlein purpura nephritis[J]. Pediatr Int,2022,64(1):e15282-e15292. doi: 10.1111/ped.15282 [11] 代彦林,张霞,高敏,等. 紫癜性肾炎患儿血清sFlt-1、vWF水平变化及其意义[J]. 山东医药,2021,61(12):51-53. doi: 10.3969/j.issn.1002-266X.2021.12.012 [12] 张迎旭,樊淑娟. 紫瘢性肾炎患儿血清FiB、D-D、sFlt-1、vWF水平变化及其临床意义[J]. 医学临床研究,2022,39(7):1033-1036. doi: 10.3969/j.issn.1671-7171.2022.07.020 [13] 张丽丽,林慧晶,蒋丽军,等. 血清骨膜蛋白、多配体蛋白聚糖4与紫癜性肾炎患儿肾脏病理分级的关系[J]. 实用临床医药杂志,2023,27(6):112-116. doi: 10.7619/jcmp.20222389 [14] 刘剑锋,霍佳雯,朱栋梁,等. 血清POSTN、SDC4水平和24 h尿蛋白定量与紫癜性肾炎患儿肾脏病理分级的相关性[J]. 天津医药,2020,48(2):128-131. doi: 10.11958/20191936 [15] 张雨,高爽,张媛. 血清sPLA2-IB、GDF-15、sST2在特发性膜性肾病患者中表达及临床意义[J]. 标记免疫分析与临床,2022,29(1):96-100. [16] 杨晶,邱晓楠,柳彩侠. 血清抗PLA2R抗体和sST2在特发性膜性肾病中的水平及临床意义[J]. 检验医学与临床,2022,19(6):758-761. [17] 任宏伟,行敏. 过敏性紫癜患儿血清IL-21、TGF-β、SST2、IgA1水平变化的临床意义[J]. 中国中西医结合皮肤性病学杂志,2022,21(5):408-411. [18] 吕霞,周小燕,焦黛妍. 血清sCAM-1、IGF-1和sFlt-1对自发性蛛网膜下腔出血后脑血管痉挛的病情与预后评估的价值[J]. 河北医药,2022,44(8):1194-1197. doi: 10.3969/j.issn.1002-7386.2022.08.017 [19] 冯凯,范贤明,欧阳晓莉,等. 不同病情老年社区获得性肺炎患者血清ALB、NT-proBNP、PTX3、SDC4的变化及对预后的影响分析[J]. 现代生物医学进展,2023,23(1):152-157. [20] 何新平,金岚,杨非柯,等. 老年慢性心力衰竭患者血清sST2、CTGF、suPAR与心功能的关系及其联合检测对心血管事件的预测价值[J]. 现代生物医学进展,2023,23(12):2347-2352. -

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 812
- HTML全文浏览量: 908
- PDF下载量: 4
- 被引次数: 0
