

The Predictive Value of Serum HSP27,CCL22,sTim-3 for the Prognosis of Periodontitis
-
摘要:
目的 探讨热休克蛋白27(heat shock protein 27,HSP27)、趋化因子配体22(CC chemokine receptor 1,CCR1)及可溶性T细胞免疫球蛋白粘蛋白分子-3(soluble T-cell immunoglobulin and mucin-domain containing-3,sTim-3)在牙周炎患者血清中的水平,分析其与牙周临床指标及预后的关联性,并检验三者及联合检测对预后的预测效能。 方法 选取2021年4月至2025年4月于北京航天总医院收治的422例牙周炎患者,并同期择取415名健康体检者构成对照组。收集两组基线及6个月随访时的血清和龈沟液(gingival crevicular fluid,GCF)样本,检测血清和GCF中HSP27、CCL22、sTim-3 水平,同时记录牙周出血指数(bleeding index,BI)、牙龈指数(gingival index,GI)、附着丧失(attachment loss,AL)、探诊深度(prob-ing depth,PD)。比较两组各指标水平差异,分析血清与GCF中HSP27、CCL22、sTim-3的相关性。比较不同预后牙周炎患者HSP27、CCL22、sTim-3的变化特点,绘制受试者工作特征(receiver operating characteristic,ROC)曲线并计算ROC曲线下面积(area under the curve,AUC)评估各指标变化值对预后不良的预测价值。 结果 牙周炎组基线及6个月随访时血清和 GCF 中 HSP27、CCL22、sTim-3 水平均显著高于健康组(P < 0.05);牙周炎组经6个月治疗后,上述血清及 GCF 指标水平均较基线显著下降(P < 0.05),健康组随访前后各指标的差异无统计学意义(P > 0.05)。Pearson 相关分析显示,牙周炎组患者血清与GCF中 HSP27、CCL22、sTim-3水平在基线及6个月随访时均呈显著正相关(P < 0.05)。预后不良组基线及6个月随访时血清 HSP27、CCL22、sTim-3水平均高于预后良好组,且治疗后指标变化值显著低于预后良好组(P < 0.05)。ROC 曲线分析显示,HSP27、CCL22、sTim-3 变化值对牙周炎患者预后不良均有良好预测价值,三者联合预测的AUC为0.925,显著高于单一指标(P < 0.05)。 结论 血清HSP27、CCL22和sTim-3是牙周炎预后的重要生物学标志物,三者联合检测对牙周炎患者的预后评估具有重要临床价值。 -
关键词:
- 牙周炎 /
- 热休克蛋白27 /
- 趋化因子配体22 /
- 可溶性T细胞免疫球蛋白粘蛋白分子-3 /
- 预后
Abstract:Objective To explore the levels of heat shock protein 27 (HSP27), chemokine ligand 22 (CCL22), and soluble T cell immunoglobulin mucin molecule-1 (sTim-3) in the serum of periodontitis patients, analyze their correlation with periodontal clinical indicators and prognosis, and test the predictive efficacy of each biomarker individually and in combination for prognosis. Methods A total of 422 patients with periodontitis admitted to Beijing Aerospace General Hospital from April 2021 to April 2025 were selected, and 415 healthy individuals who underwent physical examinations during the same period were chosen as the control group. Serum and gingival crevicular fluid (GCF) samples were collected from both groups at baseline and at the 6-month follow-up. Levels of HSP27, CCL22, and sTim-3 were measured in serum and GCF. Periodontal parameters, including bleeding index (BI), gingival index (GI), attachment loss (AL), and probing depth (PD), were recorded concurrently. Differences in these indicators between the two groups were compared, and the correlation between serum and GCF levels of HSP27, CCL22, and sTim-3 was analyzed. The characteristics of HSP27, CCL22, and sTim-3 changes were compared between periodontitis patients with different prognoses. Receiver operating characteristic (ROC) curves were plotted, and the area under the curve (AUC) was calculated to evaluate the predictive value of changes in each indicator for an unfavorable prognosis. Results At baseline and 6-month follow-up, the levels of HSP27, CCL22, and sTim-3 in serum and GCF were significantly higher in the periodontitis group than in the healthy group(P < 0.05); After 6 months of treatment, the levels of serum and GCF indicators in the periodontitis group significantly decreased compared to baseline(P < 0.05), while there were no significant differences in various indicators before and after follow-up in the healthy group(P > 0.05). Pearson correlation analysis showed that the levels of HSP27, CCL22, and sTim-3 in the serum and GCF of patients with periodontitis were significantly positively correlated at both baseline and 6-month follow-up(P < 0.05). The serum levels of HSP27, CCL22, and sTim-3 in the poor prognosis group were higher than those in the good prognosis group at both baseline and the 6-month follow-up, and the magnitude of post-treatment change in these indicators was significantly lower than those in the good prognosis group(P < 0.05). ROC curve analysis showed that the changes in HSP27, CCL22, and sTim-3 each had good predictive value for a poor prognosis in periodontitis patients. The AUC of the combined prediction of the three indicators was 0.925, significantly higher than that of a single indicator(P < 0.05). Conclusion Serum HSP27, CCL22, and sTim-3 are important biological markers for the prognosis of periodontitis. Combined detection of these three markers has significant clinical value for prognostic assessment in periodontitis patients. -
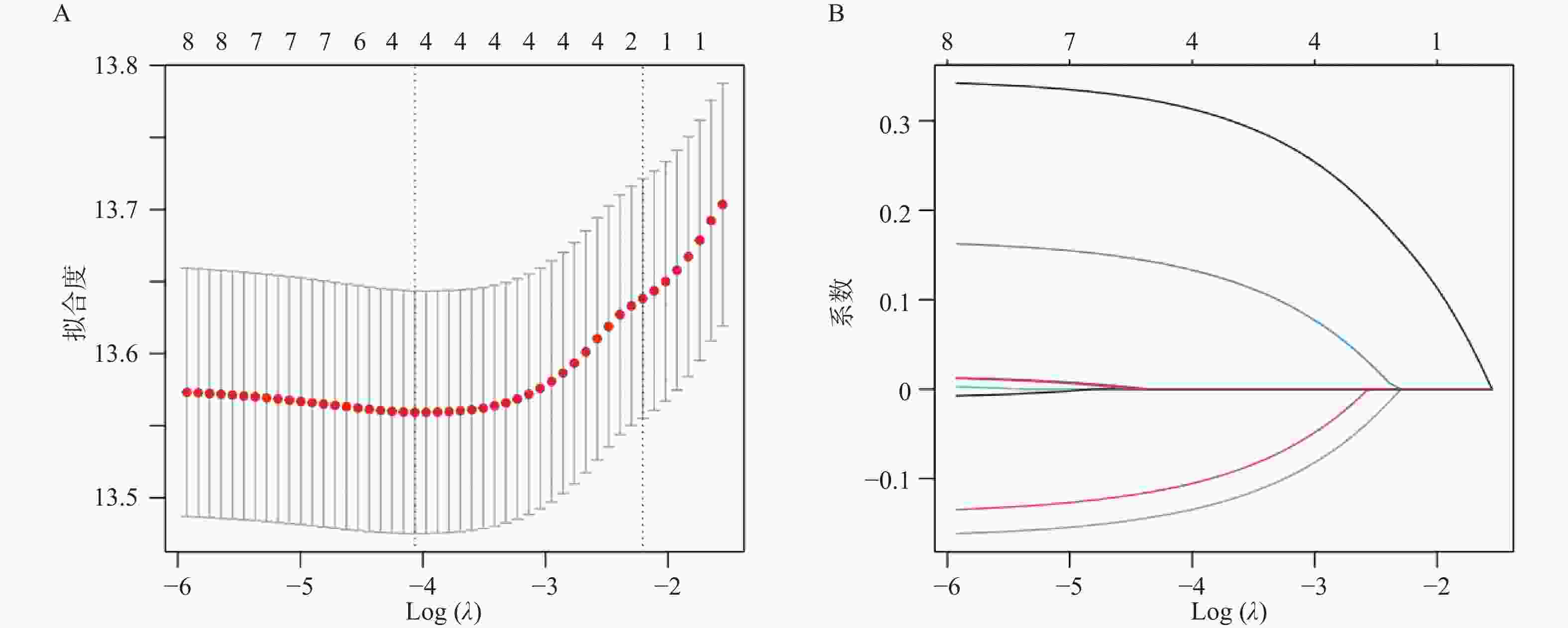
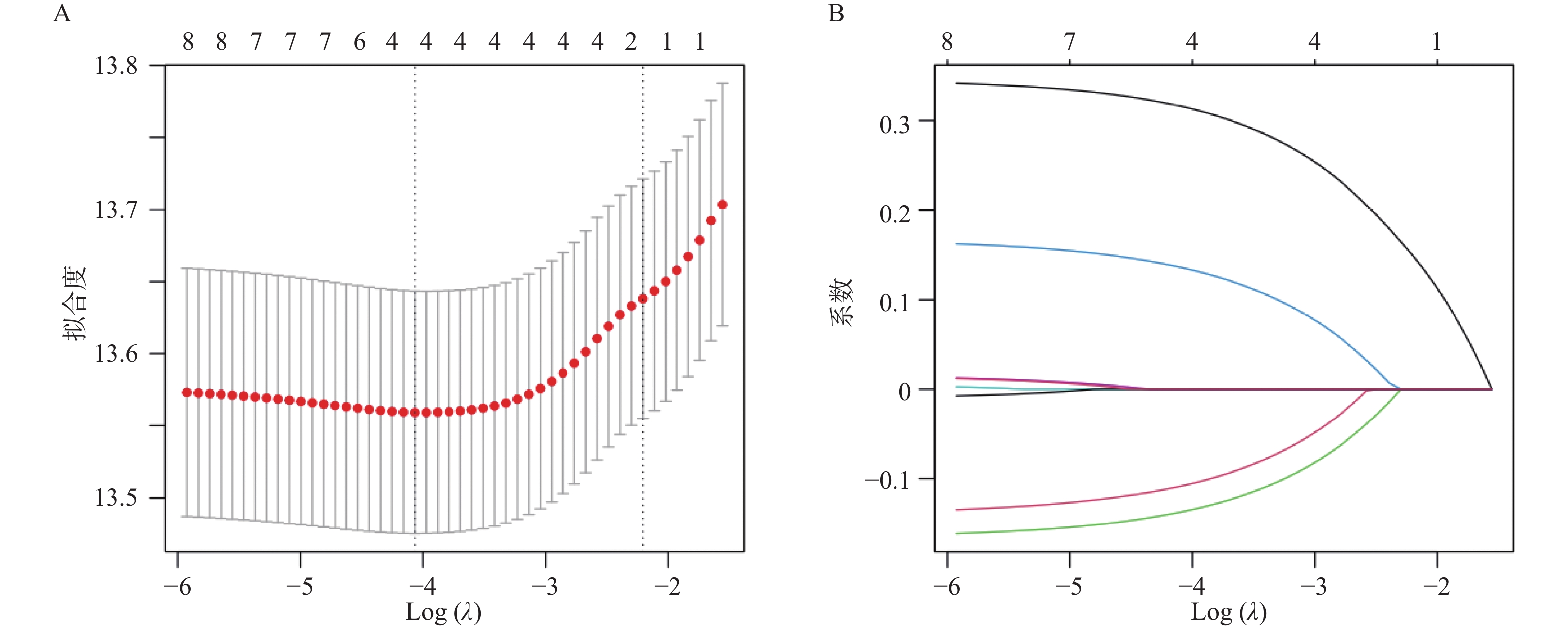
图 1 预后不良的影响因素的LASSO筛选
A:十折交叉验证曲线;B:LASSO回归系数路径图。
Figure 1. LASSO screening of factors affecting poor prognosis
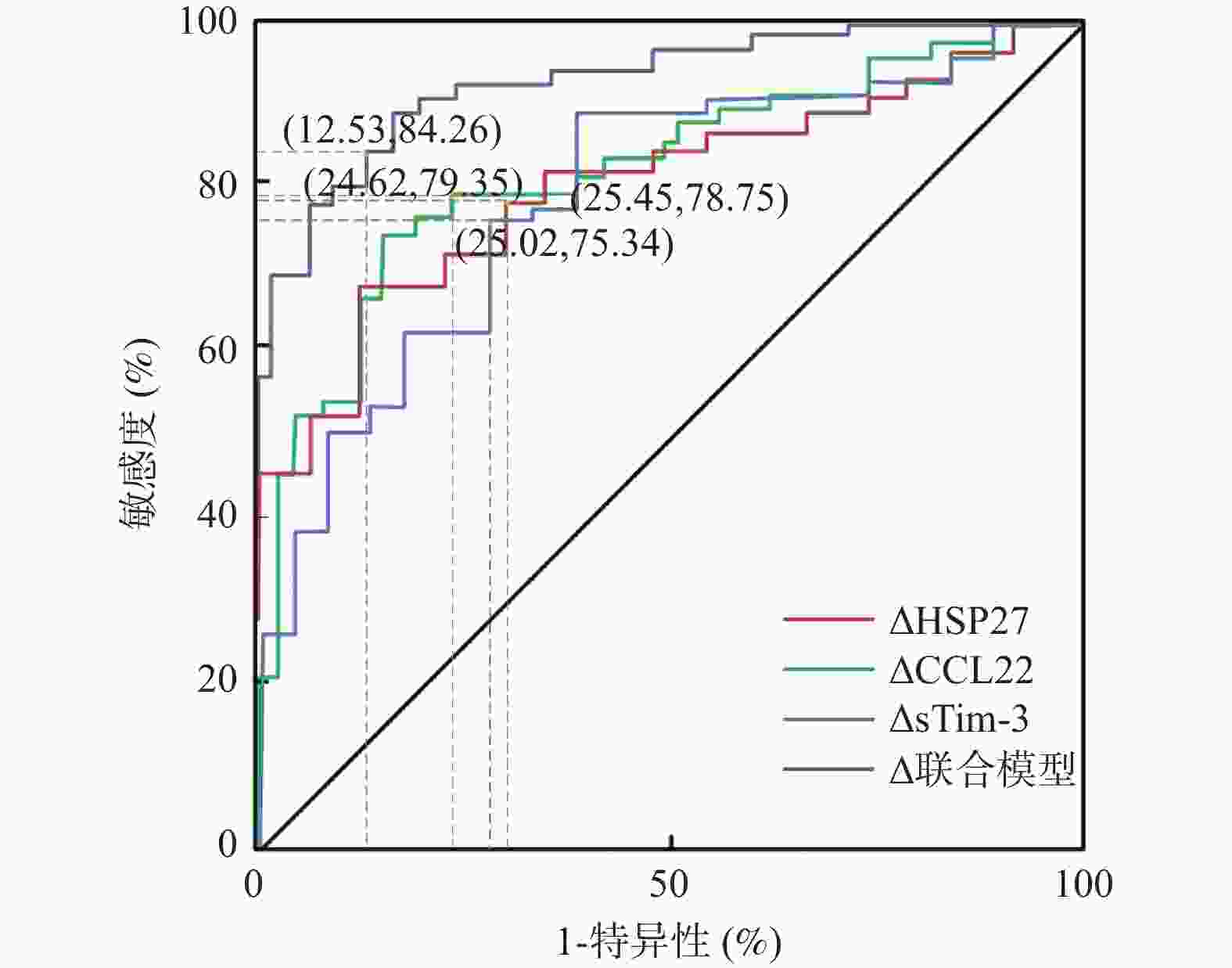
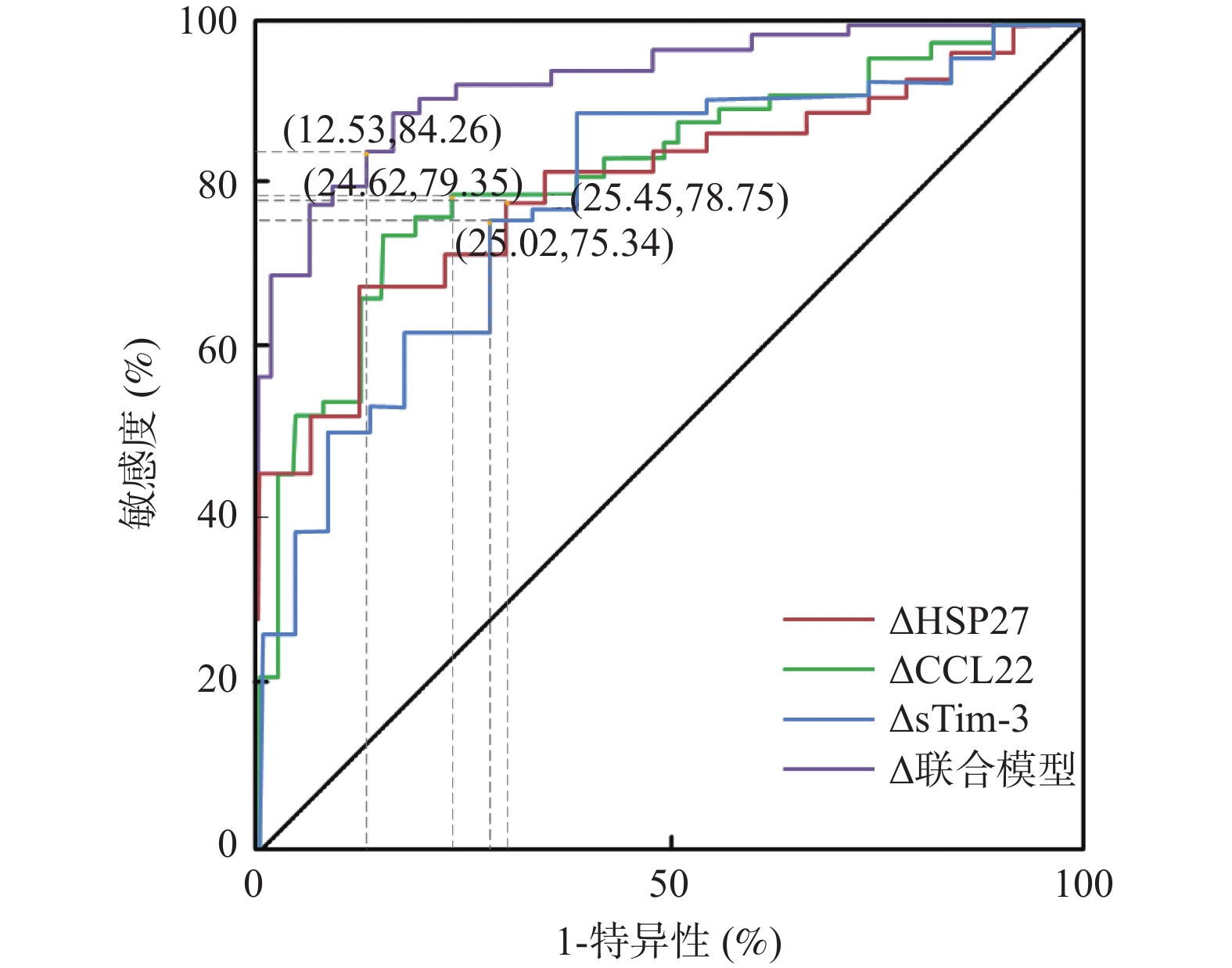
图 2 血清HSP27、CCL22、sTim-3变化值对预后不良的预测效能
Figure 2. Predictive efficacy of changes in serum HSP27,CCL22,and sTim-3 for poor prognosis
表 1 牙周炎患者和健康者基线资料比较[($\bar x \pm s $)/n(%)]
Table 1. Comparison of baseline data between periodontitis patients and healthy individuals[($\bar x \pm s $)/n(%)]
项目 牙周炎组(n=422) 健康组(n=415) t/χ2 P 年龄(岁) 45.63 ± 6.82 44.97 ± 7.15 1.367 0.172 性别 0.104 0.747 男 218(51.66) 219(52.77) 女 204(48.34) 196(47.23) BMI(kg/m2) 23.87 ± 3.26 24.05 ± 3.41 0.781 0.435 吸烟史 0.535 0.465 有 137(32.46) 125(30.12) 无 285(67.54) 290(69.88) 饮酒史 0.068 0.795 有 158(37.44) 159(38.31) 无 264(62.56) 256(61.69) 刷牙次数(次) 0.599 0.439 <2 183(43.36) 191(46.02) ≥2 239(56.64) 224(53.98)  下载: 导出CSV
下载: 导出CSV
表 2 牙周炎患者和健康者血清指标比较($\bar x \pm s $)
Table 2. Comparison of serum indicators between periodontitis patients and healthy individuals($\bar x \pm s $)
项目 牙周炎组(n=422) 健康组(n=415) t P HSP27(ng/mL) 基线 5.92 ± 1.83 4.35 ± 1.67 12.959 <0.001* 6个月随访 4.87 ± 1.65# 4.32 ± 1.66 4.807 <0.001* △值 1.05 ± 0.32 0.03 ± 0.01 64.903 <0.001* CCL22(pg/mL) 基线 785.41 ± 52.36 691.58 ± 45.29 27.709 <0.001* 6个月随访 712.36 ± 48.92# 690.24 ± 44.97 6.151 <0.001* △值 73.05 ± 14.34 1.24 ± 0.32 101.988 <0.001* sTim-3(pg/mL) 基线 325.74 ± 38.65 128.92 ± 22.41 89.932 <0.001* 6个月随访 285.42 ± 35.21# 129.05 ± 22.37 76.545 <0.001* △值 40.32 ± 12.73 0.13 ± 0.04 64.314 <0.001* *P < 0.05;与基线比较,#P < 0.05。
下载: 导出CSV
表 3 牙周炎患者和健康者GCF中HSP27、CCL22、sTim-3比较($\bar x \pm s $)
Table 3. Comparison of HSP27,CCL22,sTim-3 in GCF between periodontitis patients and healthy individuals($\bar x \pm s $)
项目 牙周炎组(n=422) 健康组(n=415) t P HSP27(ng/mL) 基线 8.42 ± 2.15 2.15 ± 0.68 56.686 <0.001* 6个月随访 5.21 ± 1.64# 2.19 ± 0.69 34.621 <0.001* △值 3.21 ± 0.52 0.04 ± 0.01 124.164 <0.001* CCL22(pg/mL) 基线 1256.34 ± 168.27312.45 ± 45.33 110.399 <0.001* 6个月随访 892.47 ± 132.56# 308.92 ± 44.15 85.154 <0.001* △值 363.87 ± 35.71 3.53 ± 1.05 18.246 <0.001* sTim-3(pg/mL) 基线 488.63 ± 75.42 85.24 ± 19.36 105.591 <0.001* 6个月随访 345.28 ± 62.33# 86.01 ± 19.23 81.030 <0.001* △值 143.35 ± 13.09 0.77 ± 0.13 221.880 <0.001* *P < 0.05;与基线比较,#P < 0.05。
下载: 导出CSV
表 4 血清与GCF中HSP27、CCL22、sTim-3的相关性
Table 4. Correlation between Serum and GCF levels of HSP27,CCL22,and sTim-3
指标 时间 r P HSP27 基线 0.712 <0.001* 6个月随访 0.685 <0.001* CCL22 基线 0.689 <0.001* 6个月随访 0.662 <0.001* sTim-3 基线 0.674 <0.001* 6个月随访 0.648 <0.001* *P < 0.05。
下载: 导出CSV
表 5 牙周炎患者和健康者牙周指标比较($\bar x \pm s $)
Table 5. Comparison of periodontal indicators between periodontitis patients and healthy individuals ($\bar x \pm s $)
项目 牙周炎组(n=422) 健康组(n=415) t P BI 基线 3.12 ± 0.86 0.45 ± 0.14 62.438 <0.001* 6个月随访 1.68 ± 0.35# 0.47 ± 0.13 66.086 <0.001* △值 1.44 ± 0.60 0.03 ± 0.01 47.866 <0.001* GI 基线 1.97 ± 0.42 0.51 ± 0.15 46.648 <0.001* 6个月随访 1.32 ± 0.23# 0.53 ± 0.14 59.904 <0.001* △值 0.65 ± 0.21 0.02 ± 0.01 61.046 <0.001* AL(mm) 基线 4.13 ± 0.98 0.23 ± 0.04 81.419 <0.001* 6个月随访 3.85 ± 0.91# 0.21 ± 0.04 81.408 <0.001* △值 0.28 ± 0.07 0.02 ± 0.01 74.917 <0.001* PD(mm) 基线 6.47 ± 1.85 1.68 ± 0.32 51.986 <0.001* 6个月随访 3.45 ± 1.12# 1.66 ± 0.31 31.397 <0.001* △值 3.02 ± 0.73 0.02 ± 0.01 83.710 <0.001* *P < 0.05;与基线比较,#P < 0.05。
下载: 导出CSV
表 6 预后良好组和预后不良组基线资料比较[($\bar x \pm s $)/n(%)]
Table 6. Comparison of baseline data between good prognosis group and poor prognosis group[($\bar x \pm s $)/n(%)]
项目 预后不良组(n=158) 预后良好组(n=264) t/χ2 P 年龄(岁) 45.75 ± 7.63 45.42 ± 7.15 0.447 0.655 性别 0.077 0.781 男 83(52.53) 135(51.14) 女 75(47.47) 129(48.86) BMI(kg/m2) 23.93 ± 3.58 23.72 ± 3.15 0.629 0.529 吸烟史 0.023 0.879 有 52(32.91) 85(32.20) 无 106(67.09) 179(67.80) 饮酒史 1.475 0.225 有 65(41.14) 93(35.23) 无 93(58.86) 171(64.77) 刷牙次数(次) 0.509 0.475 <2 65(41.14) 118(44.70) ≥2 93(58.86) 146(55.30) 基线BI 3.15 ± 0.91 3.08 ± 0.78 0.837 0.403 基线GI 2.01 ± 0.58 1.92 ± 0.45 1.780 0.076 基线AL(mm) 4.65 ± 1.12 3.82 ± 0.85 8.441 <0.001* 基线PD(mm) 7.12 ± 2.01 6.08 ± 1.68 5.987 <0.001* *P < 0.05。
下载: 导出CSV
表 7 预后良好组和预后不良组血清HSP27、CCL22、sTim-3比较($\bar x \pm s $)
Table 7. Comparison of serum HSP27,CCL22,and sTim-3 levels between the good prognosis group and the poor prognosis group($\bar x \pm s $)
项目 预后不良组(n=158) 预后良好组(n=264) t P HSP27(ng/mL) 基线 6.46 ± 1.51 5.58 ± 1.62 6.606 <0.001* 6个月随访 5.73 ± 1.32 3.82 ± 1.25 17.990 <0.001* △值 0.73 ± 0.19 1.76 ± 0.37 32.510 <0.001* CCL22(pg/mL) 基线 792.63 ± 68.74 749.58 ± 46.35 7.673 <0.001* 6个月随访 745.17 ± 65.42 665.31 ± 41.28 15.375 <0.001* △值 47.46 ± 8.92 84.27 ± 13.65 30.244 <0.001* sTim-3(pg/mL) 基线 348.45 ± 95.21 292.36 ± 78.47 6.552 <0.001* 6个月随访 309.82 ± 91.76 198.65 ± 52.51 15.831 <0.001* △值 38.63 ± 7.45 93.71 ± 25.96 26.025 <0.001* *P < 0.05;与基线比较,#P < 0.05。
下载: 导出CSV
表 8 血清HSP27、CCL22、sTim-3变化值对预后不良的预测效能
Table 8. Predictive efficacy of changes in serum HSP27,CCL22,and sTim-3 for poor prognosis
指标 敏感度(%) 特异度(%) 准确度(%) AUC 95%CI Youden指数 最佳截断值 △HSP27 78.75 74.55 77.36 0.811 0.742~0.879 0.551 0.92 ng/mL △CCL22 79.35 75.38 77.14 0.823 0.755~0.890 0.583 67.38 pg/mL △sTim-3 75.34 74.98 73.82 0.799 0.728~0.870 0.515 56.24 pg/mL 三者联合模型 84.26 87.47 86.21 0.925 0.884~0.966 0.780 0.436
下载: 导出CSV
-
[1] Trindade D, Carvalho R, Machado V, et al. Prevalence of periodontitis in dentate people between 2011 and 2020: A systematic review and meta-analysis of epidemiological studies[J]. J Clin Periodontol, 2023, 50(5): 604-626. doi: 10.1111/jcpe.13769 [2] Walther K A, Gröger S, Vogler J A H, et al. Inflammation indices in association with periodontitis and cancer[J]. Periodontol 2000, 2024, 96(1): 281-315. [3] Mendonça C D, Mata A D S P, Azevedo L F R, et al. Probiotics in the non-surgical treatment of periodontitis: A systematic review and network meta-analysis[J]. BMC Oral Health, 2024, 24(1): 1224. doi: 10.1186/s12903-024-05027-6 [4] 李超, 徐紫薇, 张璇, 等. 血清CCL21、CYTL-1水平与慢性牙周炎患者牙龈卟啉单胞菌感染及牙周临床指标的相关性[J]. 标记免疫分析与临床, 2024, 31(2): 264-269. doi: 10.11748/bjmy.issn.1006-1703.2024.02.014 [5] Boyd R A, Majumder S, Stiban J, et al. The heat shock protein Hsp27 controls mitochondrial function by modulating ceramide generation[J]. Cell Rep, 2023, 42(9): 113081. doi: 10.1016/j.celrep.2023.113081 [6] Zou S, Liu B, Feng Y. CCL17, CCL22 and their receptor CCR4 in hematologic malignancies[J]. Discov Oncol, 2024, 15(1): 412. doi: 10.1007/s12672-024-01210-x [7] Chen C, Zhao F, Peng J, et al. Soluble Tim-3 serves as a tumor prognostic marker and therapeutic target for CD8+ T cell exhaustion and anti-PD-1 resistance[J]. Cell Rep Med, 2024, 5(8): 101686. doi: 10.1016/j.xcrm.2024.101686 [8] 中华口腔医学会牙周病学专业委员会. 重度牙周炎诊断标准及特殊人群牙周病治疗原则的中国专家共识[J]. 中华口腔医学杂志, 2017, 52(2): 67-71. [9] 李黎, 徐邦勇, 高珺, 等. 米诺环素对固定义齿修复后继发牙周炎的临床疗效[J]. 昆明医科大学学报, 2017, 38(3): 75-78. [10] Chapple I L C, Mealey B L, Van Dyke T E, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions[J]. J Periodontol, 2018, 89(Suppl 1): S74-S84. doi: 10.1002/JPER.17-0719 [11] Linden G J, Lyons A, Scannapieco F A. Periodontal systemic associations: Review of the evidence[J]. J Periodontol, 2013, 84(4 Suppl): S8-S19. doi: 10.1902/jop.2013.1340010 [12] Tonetti M S, Greenwell H, Kornman K S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition[J]. J Periodontol, 2018, 89(Suppl 1): S159-S172. doi: 10.1002/JPER.18-0006 [13] Cortellini P, Cortellini S, Bonaccini D, et al. Modified minimally invasive surgical technique in human intrabony defects with or without regenerative materials-10-year follow-up of a randomized clinical trial: Tooth retention, periodontitis recurrence, and costs[J]. J Clin Periodontol, 2022, 49(6): 528-536. doi: 10.1111/jcpe.13627 [14] 姜文心, 夏晨蕾, 丁弦, 等. 牙周-正畸联合治疗对侵袭性牙周炎患者牙周功能和龈沟液TSLP、IL-33的影响及其预后的影响因素研究[J]. 现代生物医学进展, 2022, 22(20): 3972-3976+3981. doi: 10.13241/j.cnki.pmb.2022.20.034 [15] 张婧, 汪静. 慢性牙周炎患者龈沟液LF、Shh蛋白、TREM-1水平与牙周临床指标和炎性因子的相关性研究[J]. 检验医学与临床, 2023, 20(13): 1859-1863. doi: 10.3969/j.issn.1672-9455.2023.13.008 [16] Eickholz P, Schröder M, Asendorf A, et al. Effect of nonsurgical periodontal therapy on haematological parameters in grades B and C periodontitis: An exploratory analysis[J]. Clin Oral Investig, 2020, 24(12): 4291-4299. doi: 10.1007/s00784-020-03292-7 [17] Uttamani J R, Kulkarni V, Valverde A, et al. Dynamic changes in macrophage polarization during the resolution phase of periodontal disease[J]. Immun Inflamm Dis, 2024, 12(10): e70044. doi: 10.1002/iid3.70044 [18] Moore T C, Pinkerton T S, Petro T M. IRF3 promotes production of IL-6 and nitric oxide but represses CCL22 in RAW264.7 macrophage cells exposed to lipopolysaccharides in culture[J]. J Inflamm Res, 2025, 18: 1255-1265. doi: 10.2147/JIR.S496930 [19] Grossman T B, Minis E, Loeb-Zeitlin S E, et al. Soluble T cell immunoglobulin mucin domain 3 (sTim-3) in maternal sera: A potential contributor to immune regulation during pregnancy[J]. J Matern Fetal Neonatal Med, 2021, 34(24): 4119-4122. doi: 10.1080/14767058.2019.1706471 [20] 姜文心, 夏晨蕾, 丁弦, 等. 牙周-正畸联合治疗对侵袭性牙周炎患者牙周功能和龈沟液TSLP、IL-33的影响及其预后的影响因素研究[J]. 现代生物医学进展, 2022, 22(20): 3972-3976+3981. doi: 10.13241/j.cnki.pmb.2022.20.034 [21] Schröder A, Wagner K, Cieplik F, et al. Impact of phosphorylation of heat shock protein 27 on the expression profile of periodontal ligament fibroblasts during mechanical strain[J]. J Orofac Orthop, 2023, 84(Suppl 2): 143-153. [22] Chen L, Qin Y, Lin B, et al. Clinical value of the sTim-3 level in chronic kidney disease[J]. Exp Ther Med, 2022, 24(4): 606. doi: 10.3892/etm.2022.11543 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 186
- HTML全文浏览量: 114
- PDF下载量: 34
- 被引次数: 0
