

Value of A Combined Model Integrating Clinical Data, CT Features, and Radiomics in Predicting Ki-67 Expression Levels in Stage IA Lung Adenocarcinoma
-
摘要:
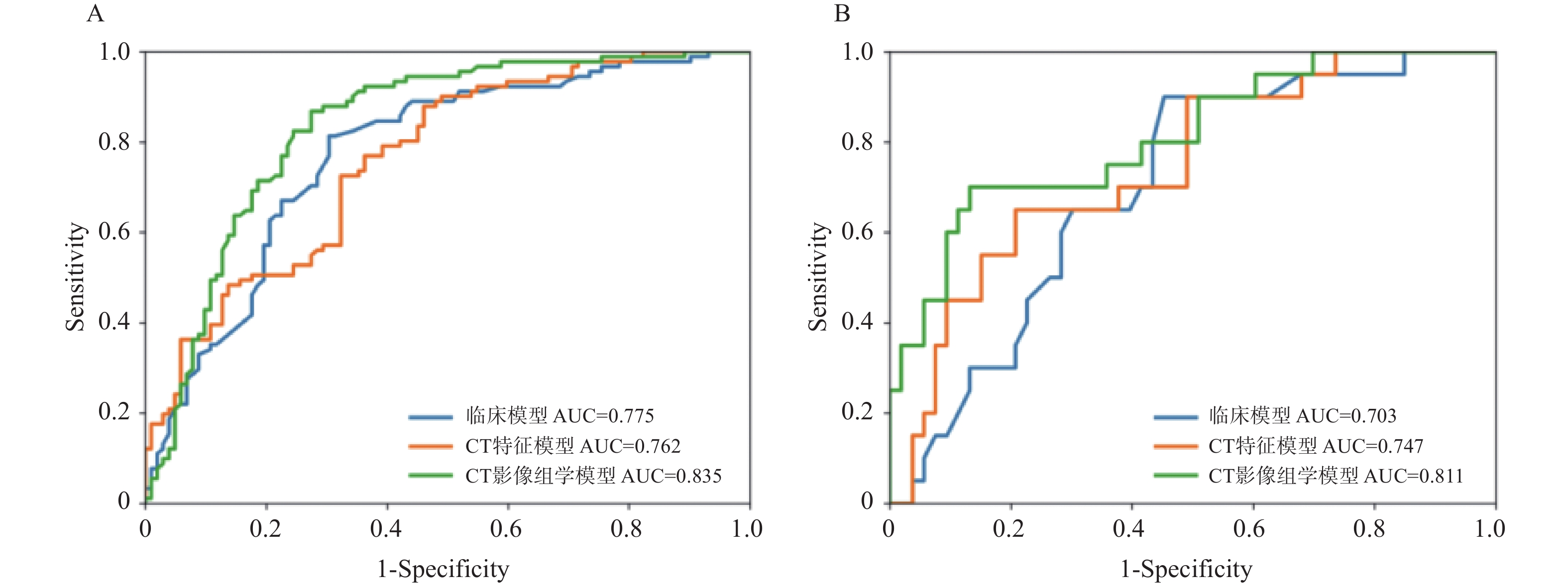
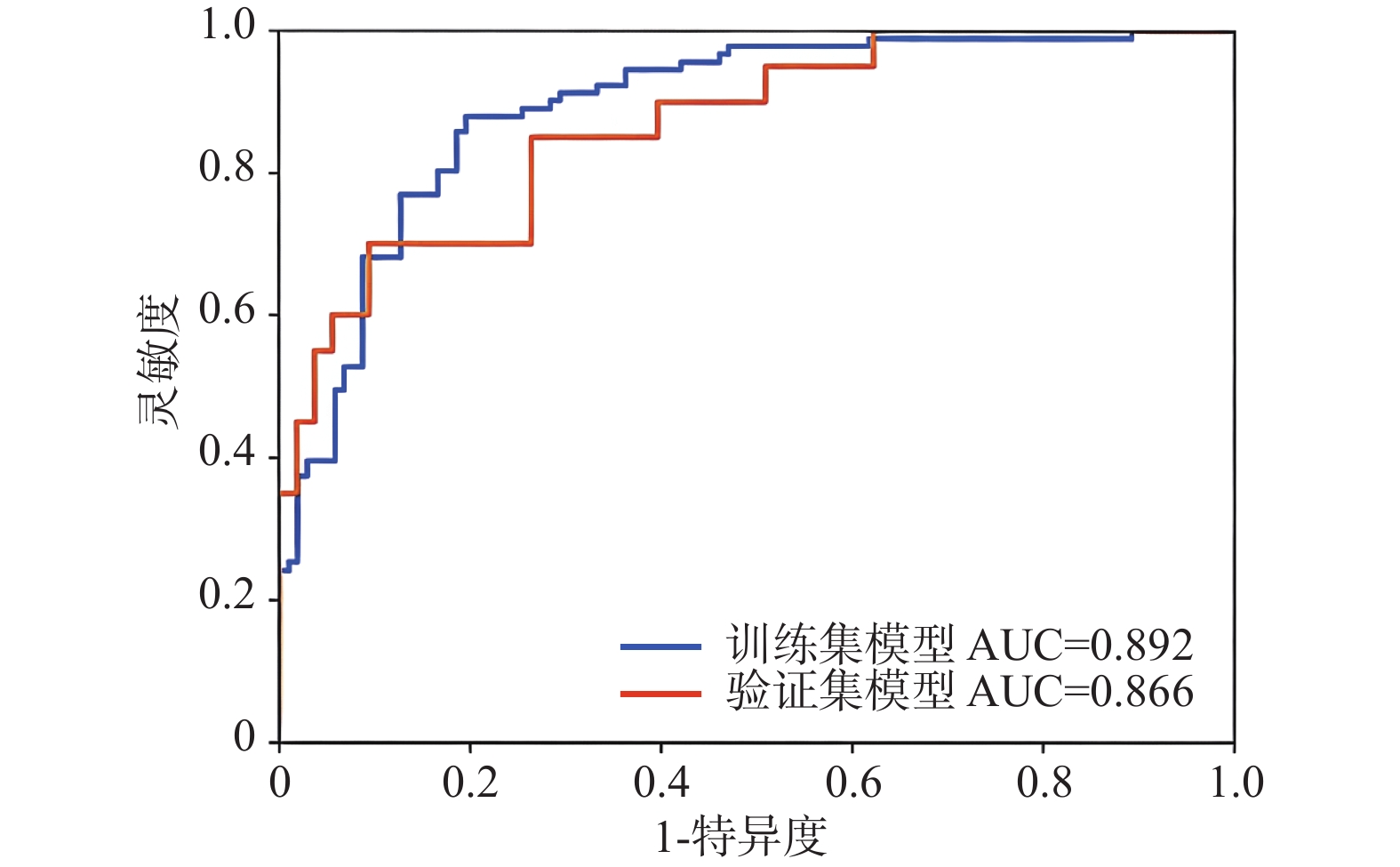
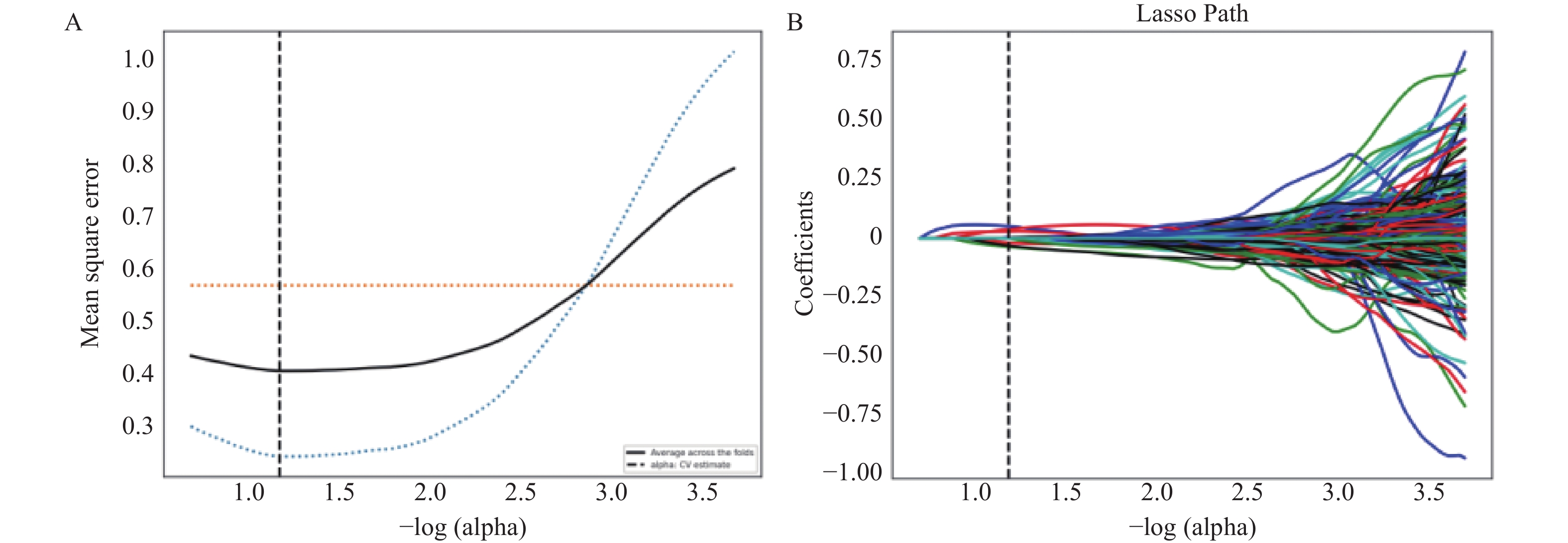
目的 探讨并构建基于临床、CT特征及影像组学特征的联合预测模型,术前预测IA期肺腺癌Ki-67表达的价值,并评估其诊断效能。 方法 回顾性收集2016年01月至2024年01月济宁市第一人民医院经手术病理证实IA期肺腺癌患者193例为训练集,2019年05月至2024年02月烟台业达医院73例患者为验证集。根据Ki-67指数分为高表达(Ki-67 ≥ 15%)和低表达(Ki-67 < 15%)。用ITK-SNAP软件勾画肿瘤感兴趣区(region of interest,ROI);采用软件Python 3.7.3及R Studio 4.1.2提取影像组学特征;采用单因素、多因素逻辑回归分析训练集和验证集的临床、CT特征,用方差阈值法和LASSO回归筛选影像组学特征,通过逻辑回归构建预测模型。将临床、CT特征的危险因素联合影像组学特征构建联合模型并生成列线图。采用受试者工作特征曲线(receiver operating characteristic,ROC)、校准曲线和决策曲线评估模型的预测性能。 结果 患者性别、年龄、病灶性质、分叶征及病灶平均直径为Ki-67高表达的独立危险因素(P < 0.05),临床模型在训练集和验证集的AUC分别为(0.775,95%CI:0.695~0.828)、(0.703,95%CI:0.578~0.828),CT特征模型在训练集和验证集的AUC分别为(0.762,95%CI:0.708~0.841)、(0.747,95%CI:0.623~0.870),影像组学模型训练集和验证集中AUC分别为 (0.835,95%CI:0.776~0.893)、(0.811,95%CI:0.697~0.925),影像组学模型预测效能较高。临床、CT特征的危险因素结合影像组学构建的联合模型,在训练集和验证集中AUC 分别为 (0.892,95%CI:0.846~0.937)、(0.866,95%CI:0.773~0.959),均高于影像组学模型,且Delong检验显示有统计学意义(P < 0.05)。 结论 基于临床、CT特征和影像组学模型可以术前预测IA期肺腺癌Ki-67表达,而联合模型可以进一步提高预测性能。 Abstract:Objective To explore and construct a combined prediction model integrating clinical, CT features and radiomics for preoperative prediction of Ki-67 expression levels in stage IA lung adenocarcinoma, and to assess its diagnostic efficacy; Methods A total of 193 patients with surgically and pathologically confirmed stage IA lung adenocarcinoma from Jining First People's Hospital ( January 2016 to January 2024) were retrospectively selected as the training set, and 73 patients from Yantai Yeda Hospital (May 2019 to February 2024) served as the validation set. Based on the Ki-67 index, patients were divided into high expression (Ki-67 ≥ 15%) and low expression (Ki-67<15%) groups. Tumor region of interest (ROI) were delineated with the ITK-SNAP; Radiomics features were extracted with Python 3.7.3 and R Studio 4.1.2; Univariate and multivariate logistic regression were used to analyze the clinical and CT features in both sets. Variance threshold method and LASSO regression were used to screen the radiomics features, and the predictive models were constructed through logistic regression. The risk factors of clinical and CT features are combined with radiomics features to construct a joint model and generate a nomogram. Model predictive performance was evaluated by the receiver operating characteristic curve (ROC), calibration curve and decision curve analysis. Result The patient's gender, age, lesion characteristics, lobulation sign, and mean lesion diameter were identified as independent risk factors for elevated Ki-67 expression (P < 0.05). The area under the curve (AUC) for the clinical model is 0.775 in the training set and 0.703 in the validation set. The AUC for the CT feature model is 0.762 in the training set and 0.747 in the validation set. The AUC for the radiomics model was 0.835 in the training set and 0.811 in the validation set, indicating a relatively high predictive efficacy. The combined model, which integrated clinical and CT feature risk factors with radiomics, achieved AUCs of 0.892 and 0.866 in the training and validation sets, respectively, both surpassing the performance of the radiomics model alone.The Delong test also demonstrated statistical significance (P < 0.05). Conclusion A model based on clinical, CT features, and radiomics allows for the preoperative prediction of Ki-67 expression levels in stage IA lung adenocarcinoma, and the combined model can enhance predictive accuracy. -
Key words:
- Lung adenocarcinoma /
- Ki-67 /
- X-ray computer tomography /
- Radiomics /
- Prediction
-
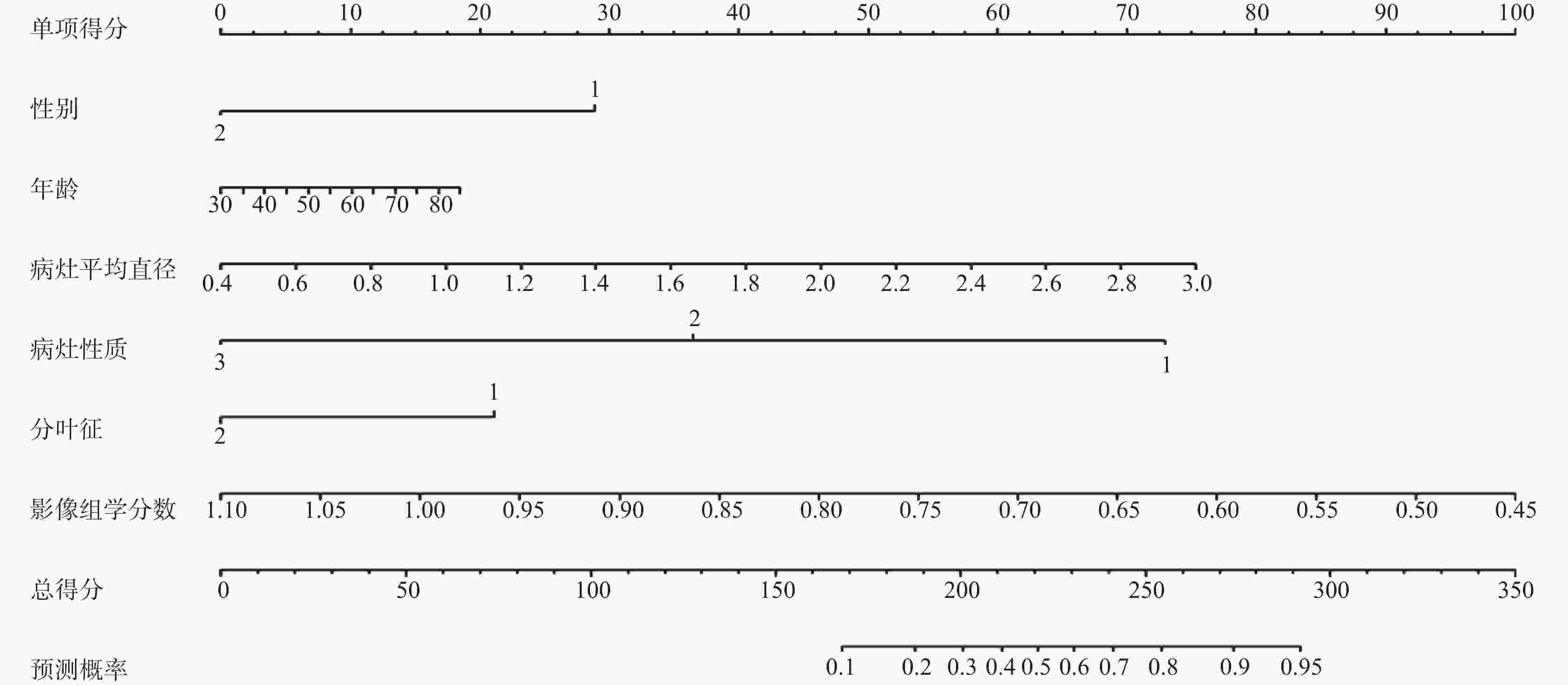
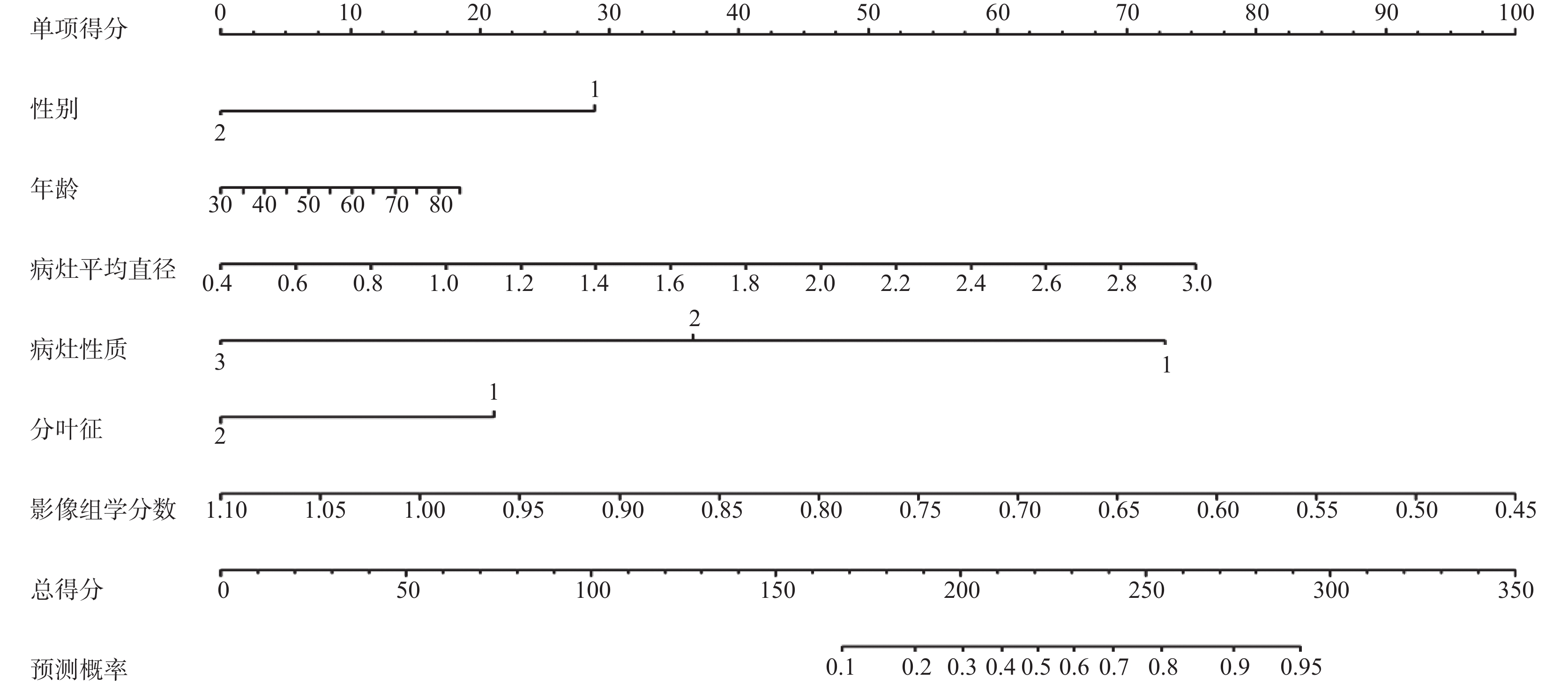
图 3 预测IA期肺腺癌Ki-67高表达联合模型的列线图模型
Figure 3. Nomogram of the combined model for predicting high Ki-67 expression in stage IA pulmonary adenocarcinoma
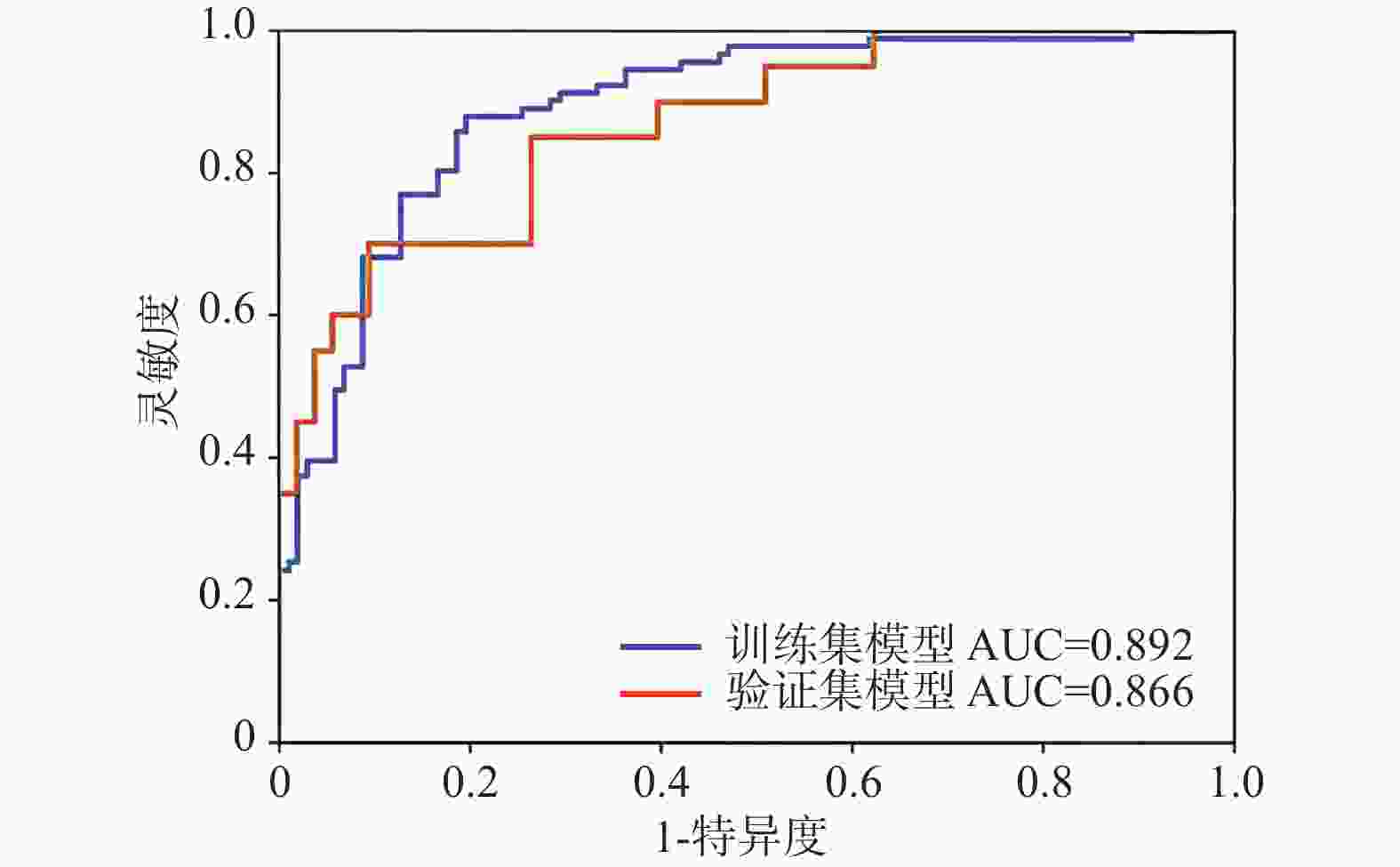
图 4 联合模型ROC曲线训练集和验证集对比
Figure 4. Comparison of the ROC curves of the joint model in training set and the validation set
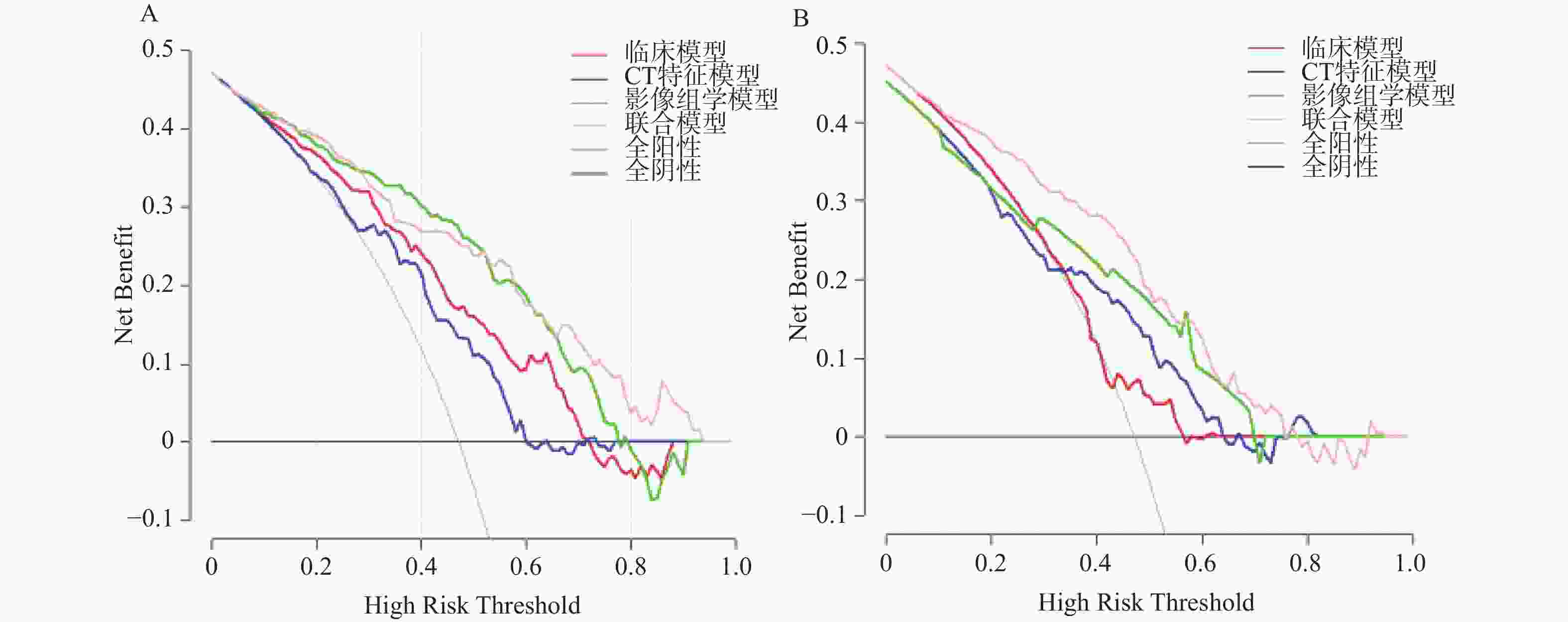
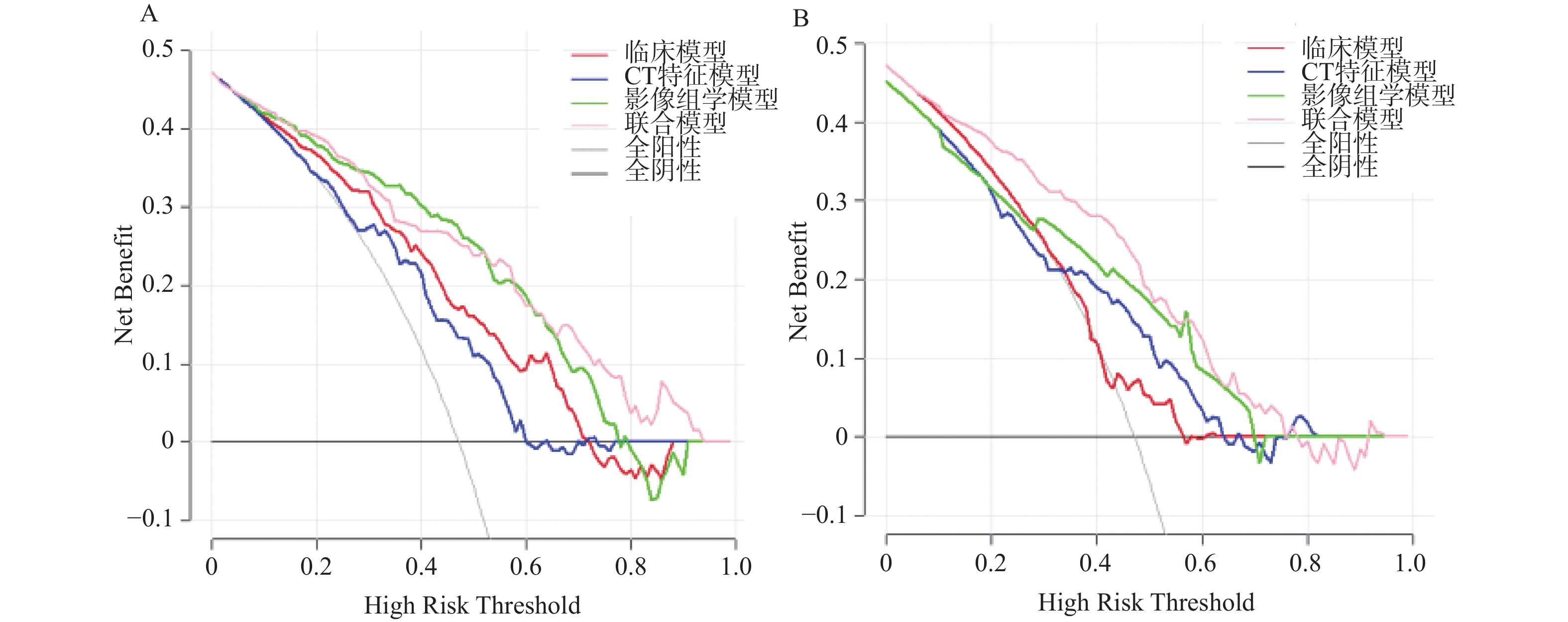
图 6 决策曲线评估联合预测模型的临床净获益情况
A:训练集;B:验证集。
Figure 6. Decision curve evaluating the clinical net benefit of the combined prediction model
表 1 变量赋值表
Table 1. Variable assignment table
变量类别 变量名称 赋值说明 结局变量 Ki67表达水平 0 = 低表达;1 = 高表达 临床特征 性别 0 = 男;1 = 女 年龄 连续型变量 咳嗽咳痰 0 = 无;1 = 有 胸痛 0 = 无;1 = 有 无症状 0 = 无;1 = 有 吸烟史 0 = 无;1 = 有 CT 特征 病灶位置 1 = 左肺上叶;2 = 左肺下叶;3 = 右肺上叶;4 = 右肺中叶;5 = 右肺下叶 病灶性质 1 = 纯实性;2 = 混合磨玻璃;3 = 磨玻璃 病灶形状 1 = 圆形;2 = 类圆形;3 = 不规则 瘤肺界面 1 = 完全清晰;2 = 大部清晰;3 = 部分清晰;4 = 完全模糊 分叶征 0 = 无;1 = 有 毛刺征 0 = 无;1 = 有 蜂窝征 0 = 无;1 = 有 空泡征 0 = 无;1 = 有 胸膜凹陷征 0 = 无;1 = 有 血管集束征 0 = 无;1 = 有 充气支气管征 0 = 无;1 = 有 病灶平均直径 连续型变量 模型变量 影像组学分数 标准化后分值  下载: 导出CSV
下载: 导出CSV
表 2 鉴别IA期肺腺癌Ki-67表达的临床资料比较[n(%)/ M(Q1,Q3)]
Table 2. Comparison of clinical data for identifying Ki-67 expression in stage IA pulmonary adenocarcinoma[n(%)/ M(Q1,Q3)]
临床特征 训练集 验证集 低表达(n=102) 高表达(n=91) Z/χ2 P 低表达(n=53) 高表达(n=20) Z/χ2 P 性别 16.57 <0.001*** 3.036 0.081 男 34(33.3) 57(62.6) 15(28.3) 10(50.0) 女 68(66.7) 34(37.4) 38(71.7) 10(50.0) 年龄(岁) 60.00(54.00,67.25) 64.00(54.00,71.00) −2.035 0.042* 57.0(51.0,65.0) 65.0(55.25,68.0) −2.149 0.032* 症状 1.775 0.412 0.727a 咳嗽咳痰 36(35.3) 33(36.3) 15(28.3) 7(35.0) 胸痛 32(31.3) 27(29.7) 2(3.8) 1(5.0) 无 44(43.2) 31(34.1) 36(67.9) 12(60.0) 吸烟史 0.010 0.922 0.326a 有 43(42.2) 39(42.8) 45(84.9) 15(75.0) 无 59(57.8) 52(57.2) 8(15.1) 5(25.0) a为Fisher's 检验;*P < 0.05;***P < 0.001。
下载: 导出CSV
表 3 鉴别IA期肺腺癌Ki-67表达的CT特征比较[n(%)/M(Q1,Q3)]
Table 3. Comparison of CT characteristics for identifying Ki-67 expression in stage IA pulmonary adenocarcinoma[n(%)/M(Q1,Q3)]
CT特征 训练集 验证集 低表达
(n=102)高表达
(n=91)Z/χ2 P 低表达
(n=53)高表达
(n=20)Z/χ2 P 病灶位置 6.191 0.185 0.285a 左肺上叶 22(21.6) 18(19.8) 16(30.2) 4(20.0) 左肺下叶 24(23.5) 11(12.1) 8(15.1) 2(10.0) 右肺上叶 30(29.4) 38(41.7) 18(34.0) 8(40.0) 右肺中叶 9(8.8) 6(6.6) 0(0) 2(10.0) 右肺下叶 17(16.7) 18(19.8) 11(20.7) 4(20.0) 性质 48.203 <0.001*** <0.001a*** 纯实性 39(38.2) 78(85.7) 3(5.7) 13(65.0) 混合磨玻璃 38(37.3) 12(13.2) 11(20.8) 5(25.0) 磨玻璃 25(24.5) 1(1.1) 39(73.7) 2(10.0) 病灶形状 0.833 0.659 0.160a 圆形 36(35.3) 28(30.8) 25(47.2) 5(25.0) 类圆形 34(33.3) 29(31.9) 19(35.8) 12(60.0) 不规则 32(31.4) 34(37.3) 9(17.0) 3(15.0) 瘤肺界面 21.557 <0.001*** <0.001a*** 完全清晰 24(23.5) 43(47.3) 13(24.5) 15(75.0) 大部清晰 16(15.7) 21(23.1) 34(64.1) 3(15.0) 部分清晰 32(31.3) 19(20.9) 3(5.7) 0(0.0) 完全模糊 30(29.4) 18(19.7) 3(5.7) 2(10.0) 分叶征 1.389 <0.001*** 0.004a** 有 29(28.4) 56(61.5) 22(41.5) 16(80.0) 无 73(71.6) 38(38.5) 31(58.5) 4(20.0) 毛刺征 9.228 0.002** 4.067 0.044* 有 45(44.1) 60(65.9) 18(34.0) 12(60.0) 无 57(55.9) 31(34.1) 35(66.0) 8(40.0) 蜂窝征 0.542 0.462 0.020 0.886 有 13(12.7) 15(16.5) 15(28.3) 6(30.0) 无 89(87.3) 76(83.5) 38(71.7) 14(70.0) 空泡征 1.666 0.197 1.752 0.186 有 44(43.1) 31(34.1) 25(47.2) 6(30.0) 无 58(56.9) 60(65.9) 28(52.8) 14(70.0) 胸膜凹陷征 7.295 0.007** 4.540 0.033* 有 56(54.9) 67(73.6) 25(47.2) 15(75.0) 无 46(45.1) 24(26.3) 28(52.8) 5(25.0) 血管集束征 0.438 0.508 1.483 0.223 有 79(77.5) 74(81.3) 26(49.1) 13(65.0) 无 23(22.5) 17(18.7) 27(50.9) 7(35.0) 充气支气管征 0.448 0.503 0.379 0.538 有 29(28.4) 22(24.2) 20(37.7) 6(30.0) 无 73(71.6) 69(75.8) 33(62.3) 14(70.0) 病灶平均直径(cm) 1.32(1.00,1.80) 1.91(1.57,2.28) −5.732 <0.001** 0.77(0.53,1.20) 1.52(0.74,2.03) −3.167 0.002** 注:a为Fisher's 检验;*P < 0.05;**P < 0.01;***P < 0.001。
下载: 导出CSV
表 4 采用Logistic回归筛选出预测Ki-67表达的独立预测因素
Table 4. Independent predictors of Ki-67 expression identified through Logistic regression analysis
危险因素 β OR 95%CI P 性别 −1.072 0.342 0.165~0.710 0.004** 年龄 0.0071 1.007 1.001~1.013 0.0305 **分叶征 −0.814 0.443 0.213~0.922 0.030** 性质 −1.582 0.205 0.102~0.414 < 0.001*** 病灶平均直径 1.195 3.303 1.659~6.576 0.001*** *P < 0.05;**P < 0.01;***P < 0.001。
下载: 导出CSV
-
[1] Ettinger D S, Wood D E, Aisner D L, et al. Non-small cell lung cancer, version 3.2022, NCCN clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2022, 20(5): 497-530. doi: 10.6004/jnccn.2022.0025 [2] Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA A Cancer J Clin, 2018, 68(6): 394-424. doi: 10.3410/f.734004835.793587632 [3] 周转, 陶旭秀, 周沛军, 等. PD-L1联合Ki67对非小细胞肺癌不同基因突变情况下分期、预后的影响[J]. 中国免疫学杂志, 2023, 39(4): 804-808. [4] 潘剑云, 黄贻恩, 洪淑君, 等. CYFRA21-1、CEA和Ki67在非小细胞肺癌中的表达及预后因素分析[J]. 中国胸心血管外科临床杂志, 2024, 31(5): 682-688. [5] Yan J, Xue X, Gao C, et al. Predicting the Ki-67 proliferation index in pulmonary adenocarcinoma patients presenting with subsolid nodules: Construction of a nomogram based on CT images[J]. Quant Imaging Med Surg, 2022, 12(1): 642-652. doi: 10.21037/qims-20-1385 [6] Liu Z, Feng H, Ma S, et al. Clinicopathological characteristics of peripheral clinical stage IA lung adenocarcinoma with high Ki-67 expression[J]. Transl Cancer Res, 2021, 10(1): 152-161. doi: 10.21037/tcr-20-2608 [7] 刘宇婷, 赵磊, 刘挨师. CT影像组学预测晚期非小细胞肺癌化疗及免疫治疗效果[J]. 中国医学影像学杂志, 2025, 33(7): 758-765. doi: 10.3969/j.issn.1005-5185.2025.07.013 [8] 许娟娟, 吕丹, 石琳鹏, 等. AI辅助从单一影像到多组学数据分析提升肺癌、肺结节精准诊疗水平[J]. 中华医学杂志, 2025, 105(44): 4013-4018. [9] 陆楚睿, 翟威豪, 王智斌. 基于术前CT影像组学生境模型对Ⅰ~ⅢA期可切除非小细胞肺癌预后的预测价值[J]. 中国医学影像学杂志, 2025, 33(9): 912-919. [10] Wilson R, Devaraj A. Radiomics of pulmonary nodules and lung cancer[J]. Transl Lung Cancer Res, 2017, 6(1): 86-91. doi: 10.21037/tlcr.2017.01.04 [11] 靳强, 高俊萍, 王欢, 等. CT放射组学鉴别诊断周围型小细胞肺癌和非小细胞肺癌的价值研究[J]. 中国CT和MRI杂志, 2025, 23(1): 47-49. doi: 10.3969/j.issn.1672-5131.2025.01.017 [12] 秦文恒, 于昊, 王正通, 等. 影像组学在非小细胞肺癌疗效及预后中的研究进展[J]. 实用放射学杂志, 2024, 40(12): 2083-2086. [13] Amin M B, Edge S B, Greene F L, et al. AJCC cancer staging manual[M]. 8th ed. New York: Springer, 2017: 125. [14] WHO Classification of Tumours Editorial Board. WHO classification of thoracic tumours[M]. 5th ed. Lyon: IARC Press, 2021: 48-62. [15] 中国医师协会外科医师分会. 中国肺癌外科诊疗指南 (2023 版)[J]. 中华外科杂志, 2023, 61(5): 321-330. [16] 中华医学会放射学分会心胸学组. 肺结节影像诊断与管理中国专家共识 (2023 版)[J]. 中华放射学杂志, 2023, 57(3): 241-250. [17] 王辰, 詹庆元. 中国肺腺癌诊疗规范 (2021 版)[J]. 中华结核和呼吸杂志, 2021, 44 (5): 437-446. [18] Wu G, Woodruff H C, Sanduleanu S, et al. Preoperative CT-based radiomics combined with intraoperative frozen section is predictive of invasive adenocarcinoma in pulmonary nodules: A multicenter study[J]. Eur Radiol, 2020, 30(5): 2680-2691. doi: 10.1007/s00330-019-06597-8 [19] 刘泽, 孙玉今. CT影像组学关于非小细胞肺癌的诊疗相关研究进展[J]. 实用放射学杂志, 2023, 39(8): 1373-1375+1386. doi: 10.3969/j.issn.1002-1671.2023.08.039 [20] 李博, 苏婕, 陈晨, 等. 探究PET/CT影像组学模型对非小细胞肺癌Ki-67表达状态的预测作用[J]. 实用放射学杂志, 2024, 40(9): 1429-1433. [21] Trivizakis E, Souglakos J, Karantanas A, et al. Deep radiotranscriptomics of non-small cell lung carcinoma for assessing molecular and histology subtypes with a data-driven analysis[J]. Diagnostics, 2021, 11(12): 2383. doi: 10.3390/diagnostics11122383 [22] Li Y, Zhang J, Lin X. Manual delineation of the region of interest combined with clinical image analysis to predict the ki-67 expression level in non-small cell lung cancer[J]. Sage Open Pathol, 2025, 18: 30502098251336608. [23] Ma X, Zhou S, Huang L, et al. Assessment of relationships among clinicopathological characteristics, morphological computer tomography features, and tumor cell proliferation in stage I lung adenocarcinoma[J]. J Thorac Dis, 2021, 13(5): 2844-2857. doi: 10.21037/jtd-21-7 [24] Gu Q, Feng Z, Liang Q, et al. Machine learning-based radiomics strategy for prediction of cell proliferation in non-small cell lung cancer[J]. Eur J Radiol, 2019, 118: 32-37. doi: 10.1016/j.ejrad.2019.06.025 [25] Huang Z, Lyu M, Ai Z, et al. Pre-operative prediction of ki-67 expression in various histological subtypes of lung adenocarcinoma based on CT radiomic features[J]. Front Surg, 2021, 8: 736737. doi: 10.3389/fsurg.2021.736737 [26] Yanagawa M, Tsubamoto M, Satoh Y, et al. Lung adenocarcinoma at CT with 0.25-mm section thickness and a 2048 matrix: High-spatial-resolution imaging for predicting invasiveness[J]. Radiology, 2020, 297(2): 462-471. doi: 10.1148/radiol.2020201911 [27] 刘佳, 崔磊. 原发性肺癌影像组学可重复性研究进展[J]. 中华放射学杂志, 2020, 54(8): 808-811. doi: 10.3760/cma.j.cn112149-20200121-00071 [28] Xu Y, Hosny A, Zeleznik R, et al. Deep learning predicts lung cancer treatment response from serial medical imaging[J]. Clin Cancer Res, 2019, 25(11): 3266-3275. doi: 10.1158/1078-0432.CCR-18-2495 [29] Fu Q, Liu S L, Hao D P, et al. CT radiomics model for predicting the ki-67 index of lung cancer: An exploratory study[J]. Front Oncol, 2021, 11: 743490. doi: 10.3389/fonc.2021.743490 [30] Zhu M, Yang Z, Zhao W, et al. Predicting Ki-67 labeling index level in early-stage lung adenocarcinomas manifesting as ground-glass opacity nodules using intra-nodular and peri-nodular radiomic features[J]. Cancer Med, 2022, 11(21): 3982-3992. doi: 10.1002/cam4.4719 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 132
- HTML全文浏览量: 74
- PDF下载量: 70
- 被引次数: 0
