

Construction of A Predictive Model for Multidrug-resistant Organisms Carriage in HIV/AIDS Patients
-
摘要:
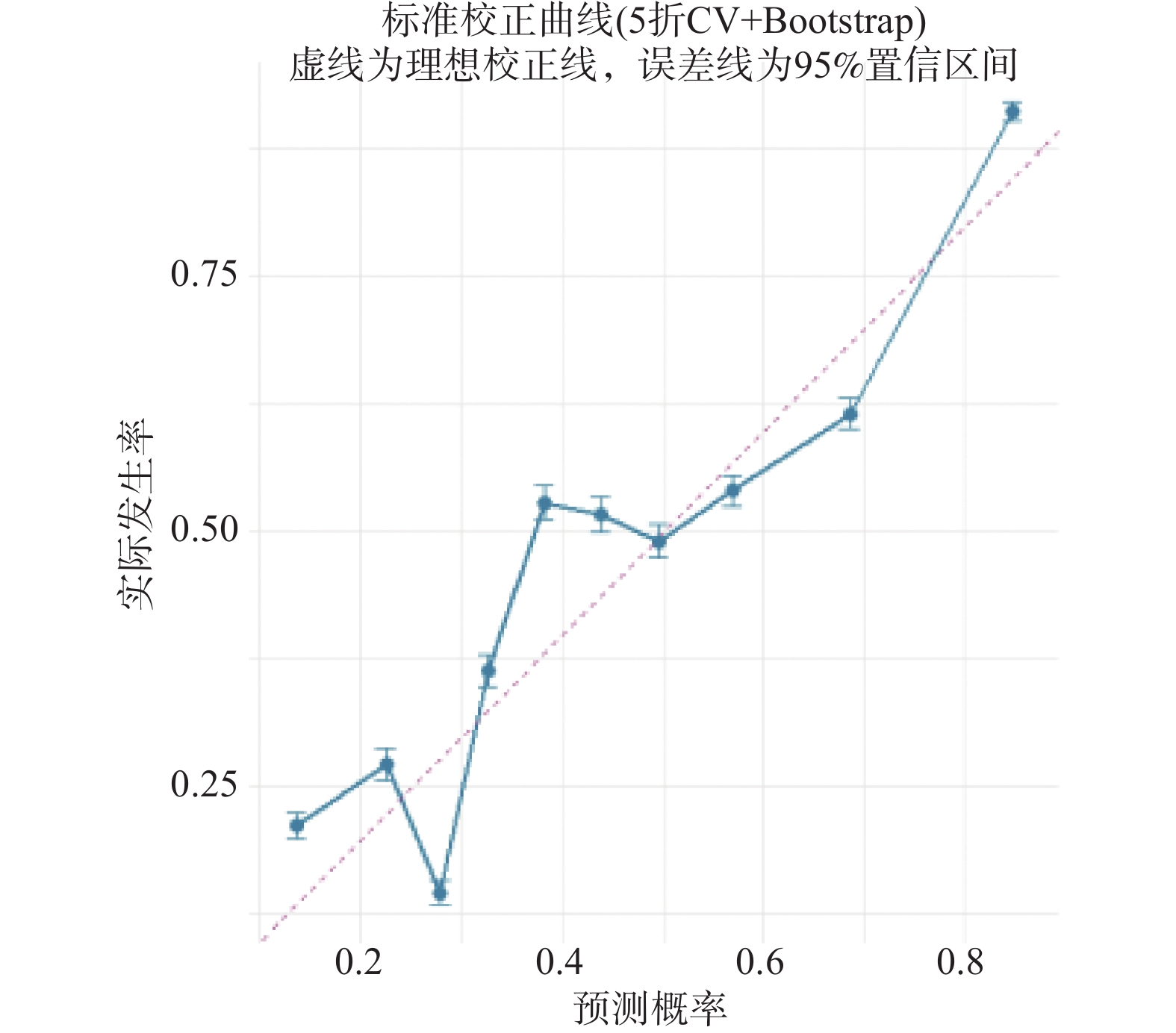
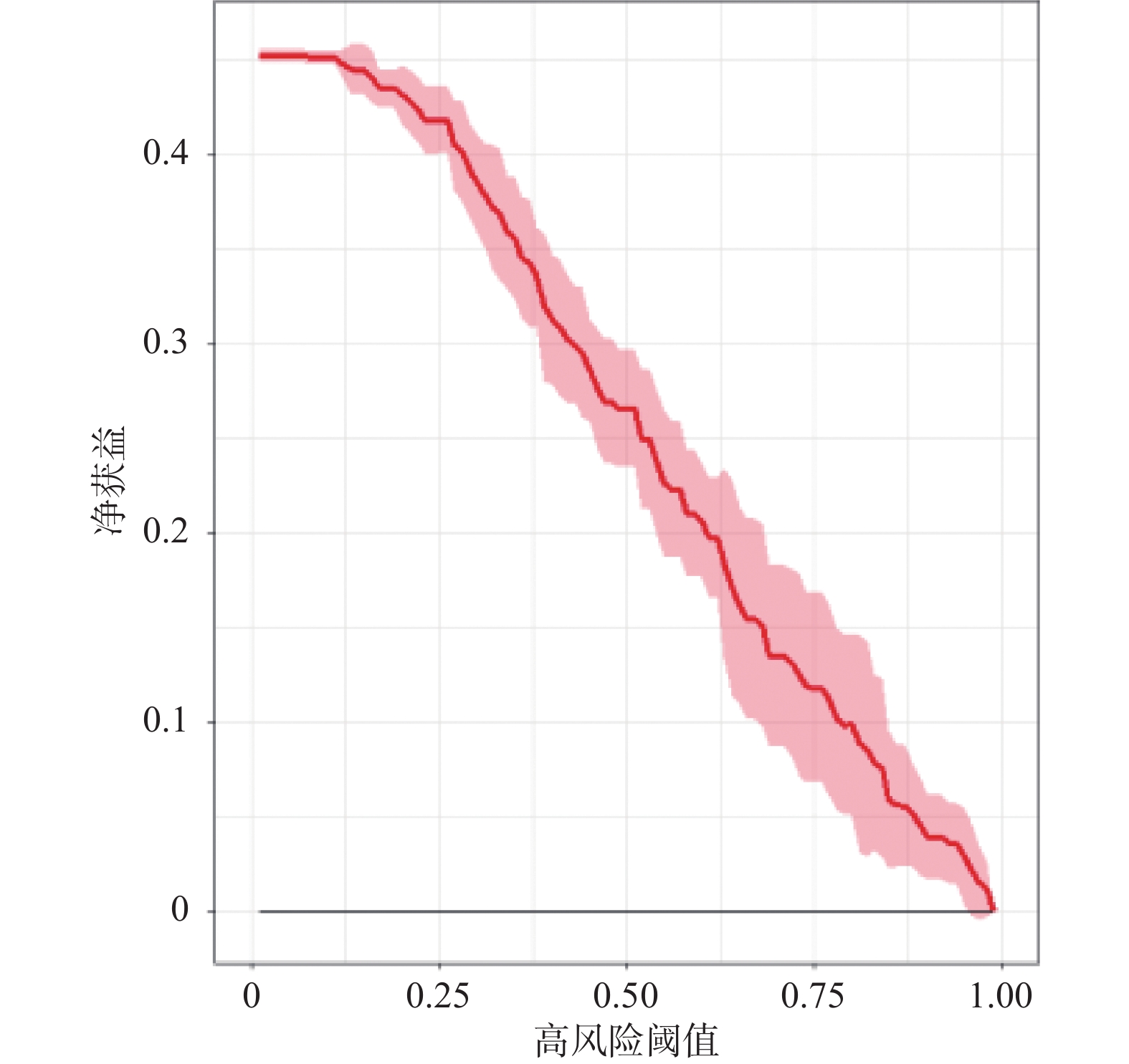
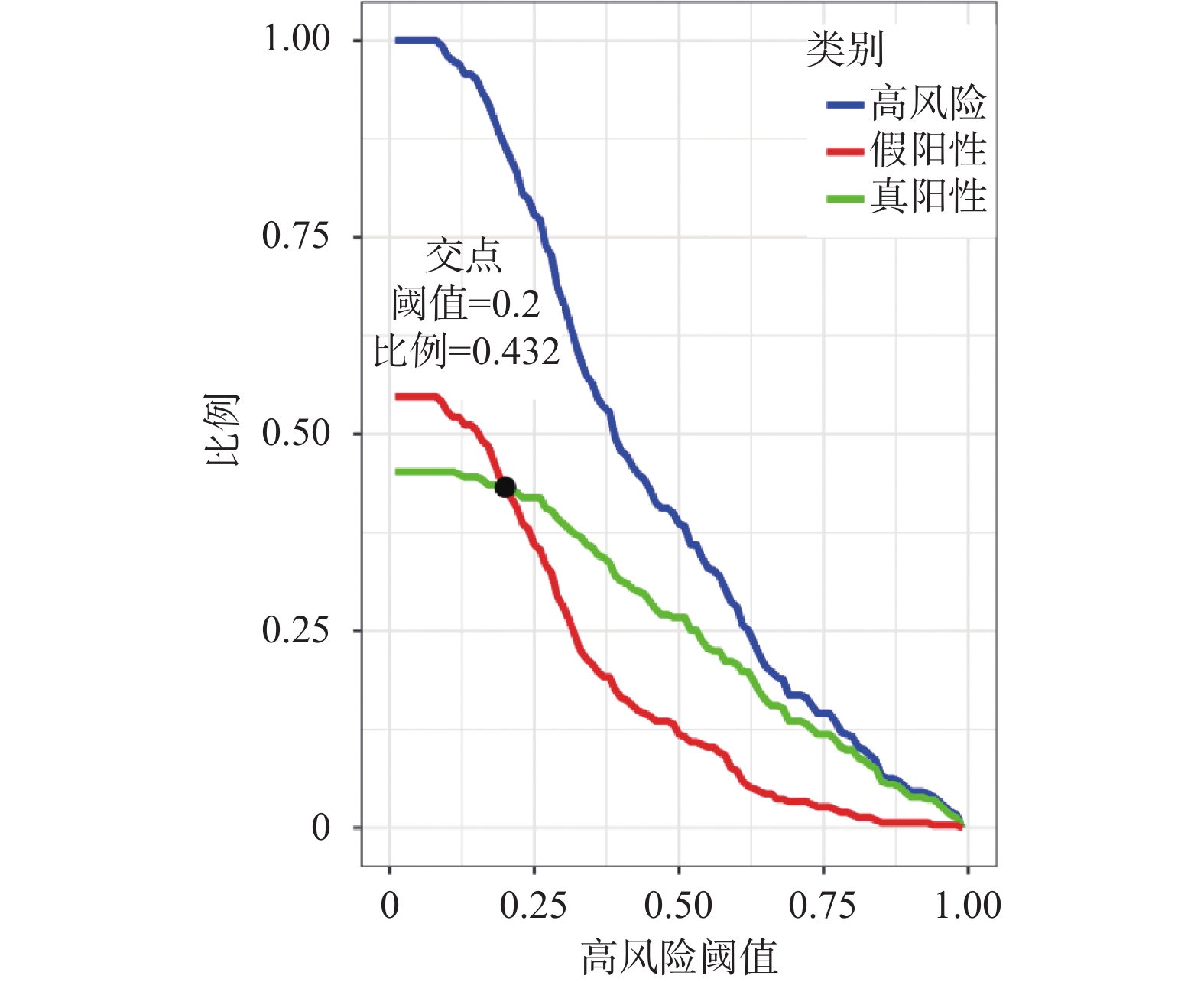
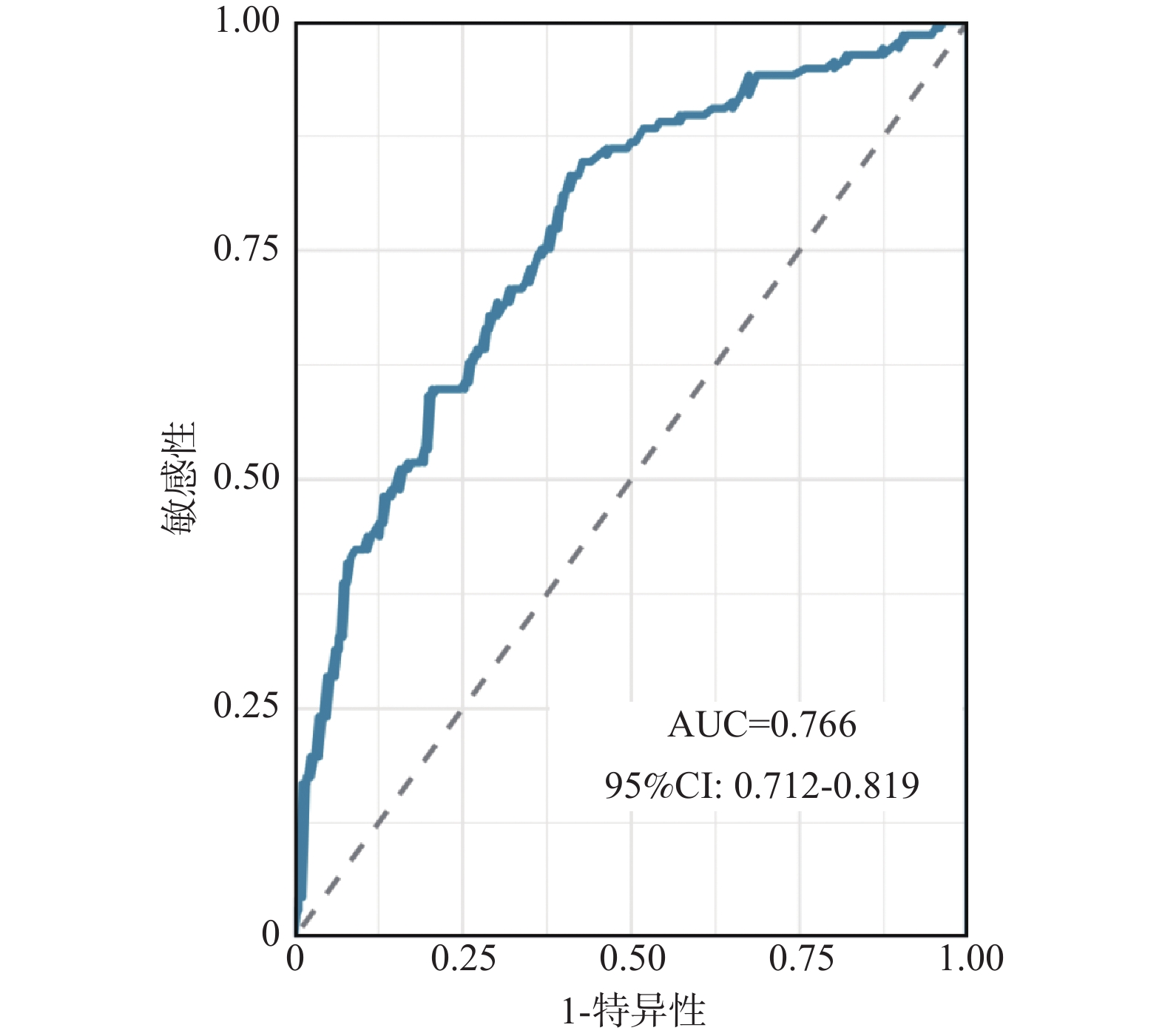
目的 探究传染病重症监护室(intensive care unit,ICU)里艾滋病患者多重耐药菌(multidrug-resistant organisms,MDRO)携带的影响因素,构建风险预测模型并评价模型的预测性能。 方法 回顾性分析2021年1月1日至2025年4月30日入住昆明市第三人民医院ICU的303例艾滋病患者的临床资料。根据患者是否检出MDRO,将患者分为N-MDRO组(n = 166例)和MDRO组(n = 137例)。采用单因素和多因素Logistic 回归分析影响艾滋病患者携带MDRO的因素,以此构建风险预测模型,并采用5折交叉验证策略评估所构建模型的性能。 结果 303例艾滋病患者中MDRO检出137例,检出率45.21%。将单因素分析筛选的10 个因素纳入Logistic回归模型,确定入住ICU 天数、呼吸机辅助通气、抗生素暴露种类及碳青霉烯类抗生素为显著影响变量。5折交叉验证显示模型平均准确率0.787、敏感性0.704、特异性0.879,受试者工作特征曲线下面积0.766;校准曲线提示模型预测与实际拟合良好,Brier评分0.199。决策曲线分析曲线在临床合理阈值内均高于无干预参考线,临床影响曲线显示全阈值下高风险人数高于真、假阳性人数之和,且阈值大于0.2时真阳性人数高于假阳性人数。 结论 ICU艾滋病患者是MDRO感染和传播的高危人群。入住ICU天数、呼吸机辅助通气、抗生素暴露数量和碳青霉烯类抗生素可作为艾滋病患者携带MDRO风险模型的预测指标。 Abstract:Objective To identify factors associated with multidrug-resistant organisms(MDRO) carriage in ICU AIDS patients, develop a risk prediction model, and assess its predictive performance. Methods A retrospective analysis was conducted on clinical data of 303 HIV/AIDS patients admitted to the ICU of Kunming Third People's Hospital from January 1, 2021 to April 30, 2025. Patients were stratified into two groups based on MDRO detection: N-MDRO group (n = 166) and MDRO group (n = 137). Univariate and multivariate logistic regression analyses were used to identify factors affecting MDRO carriage in HIV/AIDS patients, construct a risk prediction model, and evaluate model performance using 5-fold cross-validation strategy. Results Among 303 HIV/AIDS patients, 137 cases tested positive for MDRO, with a detection rate of 45.21%. Ten factors identified through univariate analysis were incorporated into the logistic regression model, identifying ICU length of stay, mechanical ventilation support, antibiotic exposure type, and carbapenem antibiotics as significant predictive variables. Five - fold cross - validation demonstrated the model achieved mean accuracy of 0.787, sensitivity of 0.704, specificity of 0.879, and area under the receiver operating characteristic curve of 0.766. The calibration curve indicated a good fit between the predicted and actual values, with a Brier score of 0.199. Decision curve analysis showed curves exceeded the no - intervention reference line within the clinically reasonable thresholds. The clinical impact curve showed that the number of high - risk patients across all thresholds exceeded the sum of true - positive and false - positive cases, and when the threshold was greater than 0.2, the number of true - positive cases was higher than that of false - positive cases. Conclusion AIDS patients in ICU are at high risk for MDRO infection and transmission. The length of ICU stay, ventilator-assisted ventilation, the number of antibiotic exposure classes, and carbapenem use can serve as predictive indicators for the MDRO carriage risk model in AIDS patients. -
Key words:
- Multidrug-resistant organisms /
- Carriage /
- Influencing factors /
- Model /
- HIV/AIDS patients
-
表 1 细菌检出情况 [n(%)]
Table 1. Bacterial detection results [n(%)]
细菌检出情况 占比 未检出细菌 124 (40.92) 检出细菌 137 (76.54) 耐药菌 137 (76.54) 非耐药菌 42 (23.46)  下载: 导出CSV
下载: 导出CSV
表 2 重要耐药菌检出情况 [n(%)]
Table 2. Detection of major drug-resistant bacteria [n(%)]
重要耐药菌种类(n = 74) 占比 耐甲氧西林金黄色葡萄球菌 6 (8.11) 耐万古霉素肠球菌(屎肠球菌、
粪肠球菌、VRE)1 (1.35) 耐碳青霉烯类肺炎克雷伯亚种 15 (20.27) 耐碳青霉烯类大肠埃希菌 32 (43.24) 耐碳青霉烯类铜绿假单胞菌 4 (5.41) 耐碳青霉烯类鲍曼不动杆菌 16 (21.62)
下载: 导出CSV
表 3 检出MDRO标本分布情况 [n(%)]
Table 3. Distribution of MDRO specimens detected [n(%)]
标本类型 占比 痰液 116 (67.44) 血培养 22 (12.79) 尿液 20 (11.63) 脓液 7(4.07) 腹水 3 (1.74) 支气管刷取物 3 (1.74) 胸水 1(0.58)
下载: 导出CSV
表 4 艾滋病患者携带MDRO的单因素分析 [n(%)/($ \bar x \pm s $)/M(P25, P75)]
Table 4. Univariate analysis of MDRO carriage in HIV/AIDS patients [n(%)/($\bar x \pm s$)/M(P25, P75)]
变量 分类 N-MDRO组
(n = 166例)MDRO组
(n = 137例)χ2/t/Z P 性别 男 102 (61.45) 98 (71.53) 3.404 0.065 女 64 (38.55) 39 (28.47) 年龄(岁) 49.54 ± 13.72 51.28 ± 13.39 −1.113 0.267 HIV病毒载量(拷贝/mL) 1.00E+02(1.00E+02,4.465E+05) 1.05E+02(1.00E+02,4.96E+05) −0.148 0.882 CD4+ T细胞计数(个/μL) 121.50(30.40,268.75) 99.80(26.32,226.50) −0.91 0.363 CD3+ T细胞计数(个/μL) 476.20(239.75,716.50) 438.00(249.50,666.77) −0.401 0.688 CD8 +T细胞计数(个/μL) 277.50(130.71,435.50) 290.00(155.00,455.98) −0.667 0.505 CD4/CD8比值 0.53(0.17,1.32) 0.32(0.13,1.21) −1.606 0.108 入住ICU天数(d) 7.08 ± 6.83 13.61 ± 10.69 −6.696 0.000* 手术 是 27 (16.27) 28 (20.44) 0.880 0.348 否 139 (83.73) 109 (79.56) 中心静脉/深静脉置管 是 113 (68.07) 113 (82.48) 8.222 0.004 否 53 (31.93) 24 (17.52) 动脉置管 是 94 (56.63) 92 (67.15) 3.509 0.061 否 72 (43.37) 45 (32.85) 鼻肠管置管 是 119 (71.69) 111 (81.02) 3.577 0.059 否 47 (28.31) 26 (18.98) 血液净化 是 54 (32.53) 46 (33.58) 0.037 0.847 否 112 (67.47) 91 (66.42) 胸腔闭式引流 是 15 (9.04) 14 (10.22) 0.121 0.728 否 151 (90.96) 123 (89.78) 腹腔穿刺引流 是 6 (3.61) 8 (5.84) 0.843 0.359 否 160 (96.39) 129 (94.16) 组织/脏器穿刺 是 16 (9.64) 14 (10.22) 0.028 0.866 否 150 (90.36) 123 (89.78) 腰椎穿刺 是 25 (15.06) 34 (24.82) 4.557 0.033 否 141 (84.94) 103 (75.18) 呼吸机辅助通气 是 92 (55.42) 99 (72.26) 9.136 0.003 否 74 (44.58) 38 (27.74) 腔镜检查 是 30 (18.07) 48 (35.04) 11.3 0.000* 否 136 (81.93) 89 (64.96) 合并真菌感染 是 89 (53.61) 92 (67.15) 5.49 0.019 否 77 (46.39) 45 (32.85) 抗生素暴露数量(种) 0~2 120 (72.29) 69 (50.36) 15.373 0.000* ≥3 46 (27.71) 68 (49.64) 碳青霉烯类抗生素 是 111 (66.87) 112 (81.75) 8.557 0.003 否 55 (33.13) 25 (18.25) *P < 0.001。
下载: 导出CSV
表 5 入住ICU天数对艾滋病患者携带MDRO的影响分析 [n(%)]
Table 5. Impact of ICU length of stay on MDRO carriage in HIV/AIDS patients [n(%)]
变量 N-MDRO组
(n = 166例)MDRO组
(n = 137例)x2 P 入住ICU天数≥7 59 (35.54) 98 (71.53) 38.94 0.000* 入住ICU天数≥14 21 (12.65) 57 (41.61) 32.919 0.000* 入住ICU天数≥30 4 (2.41) 14 (10.22) 8.192 0.004 *P < 0.001。
下载: 导出CSV
表 6 艾滋病患者携带MDRO的多因素分析
Table 6. Multivariate analysis of MDRO carriage in HIV/AIDS patients
变量 B SE Wald P OR 95% CI 下限 上限 入住ICU天数 0.098 0.019 27.859 0.000* 1.103 1.064 1.144 呼吸机辅助通气 0.702 0.279 6.321 0.012 2.018 1.167 3.488 抗生素暴露数量 1.306 0.281 21.570 0.000* 3.690 2.127 6.401 碳青霉烯类抗生素 0.681 0.312 4.765 0.029 1.975 1.072 3.638 常量 −2.580 0.389 43.951 0.000* 0.076 *P < 0.001。
下载: 导出CSV
-
[1] Efsa E F S A, Ema E M A. Antimicrobial consumption and resistance in bacteria from humans and food-producing animals: Fourth joint inter-agency report on integrated analysis of antimicrobial agent consumption and occurrence of antimicrobial resistance in bacteria from humans and food-producing animals in the EU/EEA JIACRA IV–2019–2021[J]. EFSA J, 2024, 22(2): e8589. [2] Naghavi M, Vollset S E, Ikuta K S, et al. Global burden of bacterial antimicrobial resistance 1990–2021: A systematic analysis with forecasts to 2050[J]. Lancet, 2024, 404(10459): 1199-1226. doi: 10.1016/S0140-6736(24)01867-1 [3] Zhen X, Lundborg C S, Sun X, et al. Economic burden of antibiotic resistance in ESKAPE organisms: A systematic review[J]. Antimicrob Resist Infect Control, 2019, 8(1): 137. doi: 10.1186/s13756-019-0590-7 [4] Blot S, Ruppé E, Harbarth S, et al. Healthcare-associated infections in adult intensive care unit patients: Changes in epidemiology, diagnosis, prevention and contributions of new technologies[J]. Intensive Crit Care Nurs, 2022, 70: 103227. doi: 10.1016/j.iccn.2022.103227 [5] 何凤玲, 邵星, 宋晓莉, 等. 艾滋病患者医院感染多药耐药菌及易感部位分析[J]. 中华医院感染学杂志, 2018, 28(2): 210-212+217. [6] Sy C L, Chen P Y, Cheng C W, et al. Recommendations and guidelines for the treatment of infections due to multidrug resistant organisms[J]. J Microbiol Immunol Infect, 2022, 55(3): 359-386. doi: 10.1016/j.jmii.2022.02.001 [7] The burden of bacterial antimicrobial resistance in the WHO European region in 2019: A cross-country systematic analysis[J]. The Lancet Public Health, 2022, 7(11): e897-e913. [8] 中华医学会感染病学分会艾滋病学组, 中国疾病预防控制中心, 沈银忠, 等. 中国艾滋病诊疗指南(2024版)[J]. 中国预防医学杂志, 2024, 25(12): 1469-1497. doi: 10.16506/j.1009-6639.2025.02.001 [9] 黄勋, 邓子德, 倪语星, 等. 多重耐药菌医院感染预防与控制中国专家共识[J]. 中国感染控制杂志, 2015, 14(1): 1-9. [10] 杨启文, 吴安华, 胡必杰, 等. 临床重要耐药菌感染传播防控策略专家共识[J]. 中国感染控制杂志, 2021, 20(1): 1-14. [11] Tilahun M, Gedefie A, Sahle Z. Asymptomatic carriage rate, multidrug resistance level, and associated risk factors of Enterococcus in clinical samples among HIV-positive patients attending at debre birhan comprehensive specialized hospital, North Showa, Ethiopia[J]. BioMed Res Int, 2023, 2023: 7310856. doi: 10.1155/2023/7310856 [12] 努尔恰西·艾布都热索力. AIDS合并多重耐药菌感染患者原因分析及预防措施[J]. 世界最新医学信息文摘, 2017, 17(51): 93, 97. [13] 冯玲, 桂希恩, 桂静, 等. HIV/AIDS住院病人多重耐药菌感染的临床特点分析及干预[J]. 医学动物防制, 2020, 36(10): 926-929+933. [14] 邹倩, 耿苗苗, 祝延红. 基于循证理论构建重症监护病房患者多重耐药菌感染风险预测模型及外部验证研究[J]. 中国全科医学, 2022, 25(12): 1441-1448. [15] Heath M R, Fan W, Leu C S, et al. Gut colonization with multidrug resistant organisms in the intensive care unit: A systematic review and meta-analysis[J]. Crit Care, 2024, 28(1): 211. doi: 10.1186/s13054-024-04999-9 [16] Diao H, Lu G, Zhang Y, et al. Risk factors for multidrug-resistant and extensively drug-resistant Acinetobacter baumannii infection of patients admitted in intensive care unit: A systematic review and meta-analysis[J]. J Hosp Infect, 2024, 149: 77-87. doi: 10.1016/j.jhin.2024.04.013 [17] Harris P N A, Tambyah P A, Lye D C, et al. Effect of piperacillin-tazobactam vs meropenem on 30-day mortality for patients with E coliorKlebsiella pneumoniae bloodstream infection and ceftriaxone resistance: A randomized clinical trial[J]. Jama, 2018, 320(10): 984. doi: 10.1001/jama.2018.12163 [18] 井然, 卓超, 徐英春, 等. 临床产超广谱β-内酰胺酶肠杆菌目细菌感染应对策略专家共识(2025)[J]. 中国感染控制杂志, 2025, 24(9): 1191-1207. [19] 胡必杰. 中国碳青霉烯耐药革兰阴性杆菌(CRO)感染预防与控制技术指引[J]. 中华医院感染学杂志, 2019, 29(13): 2075-2080. [20] 王佳, 冯磊, 郑玉磊, 等. 鲍曼不动杆菌多重耐药性与外排泵及生物膜形成相关性研究[J]. 昆明医科大学学报, 2024, 45(12): 115-121. [21] 邓昕, 夏玉朝. 2009—2011年AIDS住院患者多重耐药菌感染调查及耐药性分析[J]. 中国感染控制杂志, 2013, 12(4): 256-258+293. [22] 刘婧婕. 艾滋病相关机会性感染病原菌分布及耐药性分析[J]. 首都食品与医药, 2023, 30(18): 42-45. doi: 10.3969/j.issn.1005-8257.2023.18.015 [23] 丁梦媛, 李文进, 耿苗苗, 等. 综合重症监护病房患者多重耐药菌医院感染风险评估模型构建[J]. 中国卫生资源, 2020, 23(4): 384-387+399. doi: 10.13688/j.cnki.chr.2020.20326 [24] Yan Zhou, Fan Yu, Ying Yu, et al. Clinical significance of MDRO screening and infection risk factor analysis in the ICU[J]. Am J Transl Res, 2021, 13(4): 3717-3723. [25] 杨晋如, 谈宜斌, 邬闻文, 等. 重症医学科不同置管患者多重耐药菌感染的生存分析[J]. 中国感染与化疗杂志, 2021, 21(3): 297-302. [26] 邹倩, 丁梦媛, 耿苗苗, 等. ICU多重耐药菌感染判别分析预判模型建立研究[J]. 医学研究杂志, 2021, 50(1): 32-36. [27] 黎琪, 杨柔, 周小诗, 等. 重症监护病房患者多重耐药菌感染的危险因素分析和列线图模型评价[J]. 中国医药, 2024, 19(3): 426-430. [28] Tamma P D, Aitken S L, Bonomo R A, et al. Infectious diseases society of America guidance on the treatment of AmpC β-Lactamase–producing enterobacterales, Carbapenem-resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia infections[J]. Clin Infect Dis, 2022, 74(12): 2089-2114. doi: 10.1093/cid/ciab1013 [29] 何江娟, 瞿婷婷. 重症监护病房多重耐药菌感染风险预测模型研究进展[J]. 中华临床感染病杂志, 2023, 16(5): 384-390. [30] Zhang D, Micek S T, Kollef M H. Time to appropriate antibiotic therapy is an independent determinant of postinfection ICU and hospital lengths of stay in patients with sepsis[J]. Crit Care Med, 2015, 43(10): 2133-2140. doi: 10.1097/CCM.0000000000001140 [31] 王浩, 代凯利, 周记, 等. 中国ICU成人病人多重耐药菌感染影响因素的Meta分析[J]. 循证护理, 2024, 10(22): 3996-4003. [32] Liu X, Zhang L, Li X, et al. Single-cell multi-omics profiling uncovers the immune heterogeneity in HIV-infected immunological non-responders[J]. eBioMedicine, 2025, 115: 105667. doi: 10.1016/j.ebiom.2025.105667 [33] Bono V, Marchetti G C. Immunological recovery with BIC/FTC/TAF: CD4 T-cell count and CD4/CD8 ratio as markers of response[J]. New Microbiologica, 2025, 48(1): 1-4. [34] Dumford D 3rd, Skalweit M J. Antibiotic-resistant infections and treatment challenges in the immunocompromised host: An update[J]. Infect Dis Clin North Am, 2020, 34(4): 821-847. doi: 10.1016/j.idc.2020.08.005 [35] Rachman B E, Supranoto Y T N, Iskandar S I, et al. Defining and predicting HIV immunological non-response: A multi-definition analysis from an Indonesian cohort[J]. Viruses, 2025, 17(12): 1581. doi: 10.3390/v17121581 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3
- HTML全文浏览量: 1
- PDF下载量: 0
- 被引次数: 0
