

Establishment and Evaluation of a Risk Prediction Model for Chronic Liver Failure Complicated by Primary Hepatocellular Carcinoma Before Intervention
-
摘要:
目的 分析原发性肝癌(PHC)干预前并发慢性肝衰竭的影响因素,建立列线图风险预测模型并进行评价。 方法 收集PHC的一般资料和入院24 h内临床检测资料等进行回顾性分析,使用单因素分析和Lasso回归进行变量筛选后进行多因素Logistic回归分析,确定PHC干预前并发慢性肝衰竭的独立影响因素,据此建立PHC干预前并发慢性肝衰竭的列线图风险预测模型。使用Hosmer-Lemeshow检验、绘制受试者工作特征曲线(ROC)、校准曲线、临床决策曲线、临床影响曲线对模型进行评价。 结果 共收集PHC患者353例,肝衰竭组(n = 153)和非肝衰竭组(n = 200),患病率43.3%。Lasso回归筛选出的变量有消化道出血、凝血酶原时间(PT)、白蛋白(ALB)、总胆红素(TBIL)、γ谷氨酰转移酶(GGT),进行多因素Logistic回归分析结果显示:消化道出血(OR = 13.549,95%CI 2.899~63.322,P = 0.001)、PT(OR = 1.599,95%CI 1.282~1.995,P < 0.001)、TBIL(OR = 1.016,95%CI 1.006~1.025,P = 0.002)、GGT(OR = 1.002,95%CI 1.000~1.003,P = 0.028)是PHC干预前并发慢性肝衰竭的独立影响因素,据此建立列线图风险预测模型。Hosmer-Lemeshow检验显示该模型具有较好的拟合度(χ2 = 6.152,P > 0.05);ROC下面积为0.902(0.869~0.934),灵敏度80.4%,特异度87.5%。校准曲线显示该模型预测PHC干预前并发慢性肝衰竭具有较好的一致性。临床决策曲线和临床影响曲线显示在一定阈值范围内该模型具有较好的临床实用性。 结论 有消化道出血、PT≥16.05 s、TBIL≥37.80 mmol/L、GGT≥99.00 U/L是PHC干预前发生慢性肝衰竭的独立危险因素,建立的列线图风险预测模型在预测PHC干预前发生慢性肝衰竭的风险时具有一定的临床应用价值。 Abstract:Objective To analyze the influencing factors of chronic liver failure in patients with primary hepatic carcinoma (PHC) before intervention, and to establish and evaluate a nomogram risk prediction model. Methods A retrospective analysis was conducted by collecting general data and clinical test data within 24 hours of admission for PHC patients. Univariate analysis and Lasso regression were used for variable selection, followed by multivariate logistic regression analysis to identify independent influencing factors for CLF before PHC intervention, leading to the establishment of a nomogram risk prediction model. The model was evaluated using the Hosmer-Lemeshow test, receiver operating characteristic (ROC) curve, calibration curve, clinical decision curve, and clinical impact curve. Result A total of 353 cases of PHC patients were collected, including 153 cases in the liver failure group and 200 cases in the non-liver failure group, with a prevalence rate of 43.3%. Variables selected by Lasso regression included gastrointestinal bleeding, prothrombin time (PT), albumin (ALB), total bilirubin (TBIL), and gamma glutamyl transferase (GGT). Multivariate logistic regression analysis showed that gastrointestinal bleeding (OR = 13.549, 95%CI: 2.899~63.322, P = 0.001), PT (OR = 1.599, 95%CI: 1.282~1.995, P < 0.001), TBIL (OR = 1.016, 95%CI: 1.006~1.025, P = 0.002), and GGT (OR = 1.002, 95%CI: 1.000~1.003, P = 0.028) were independent risk factors for chronic liver failure prior to PHC intervention, leading to the establishment of a nomogram risk prediction model. The Hosmer Lemeshow test showed that the model had a good fit (χ2 = 6.152, P > 0.05); the area under ROC was 0.902 (0.869-0.934), with a sensitivity of 80.4% and a specificity of 87.5%. The calibration curve indicated that the model predicts chronic liver failure prior to PHC intervention with good consistency. Clinical decision curve analysis and clinical impact curve analysis showed that the model has good clinical utility within a certain threshold range. Conclusion Gastrointestinal bleeding, PT≥16.05s, TBIL≥37.80 mmol/L, and GGT≥99.00 U/L are independent risk factors for the occurrence of chronic liver failure before PHC intervention. The established nomogram risk prediction model has certain clinical application value in predicting the risk of chronic liver failure before PHC intervention. -
Key words:
- Primary liver cancer /
- Chronic liver failure /
- Influencing factors /
- Prediction model
-
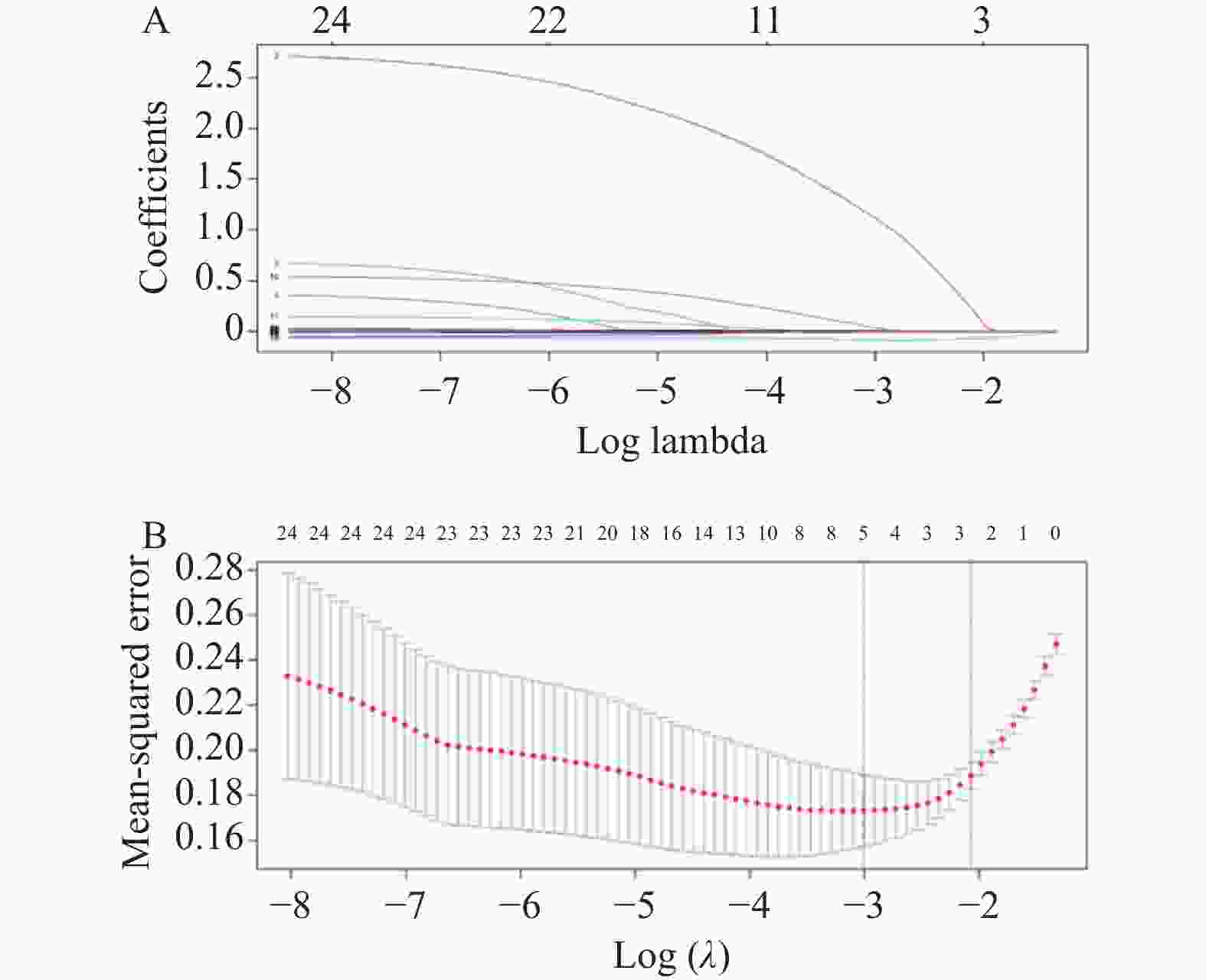
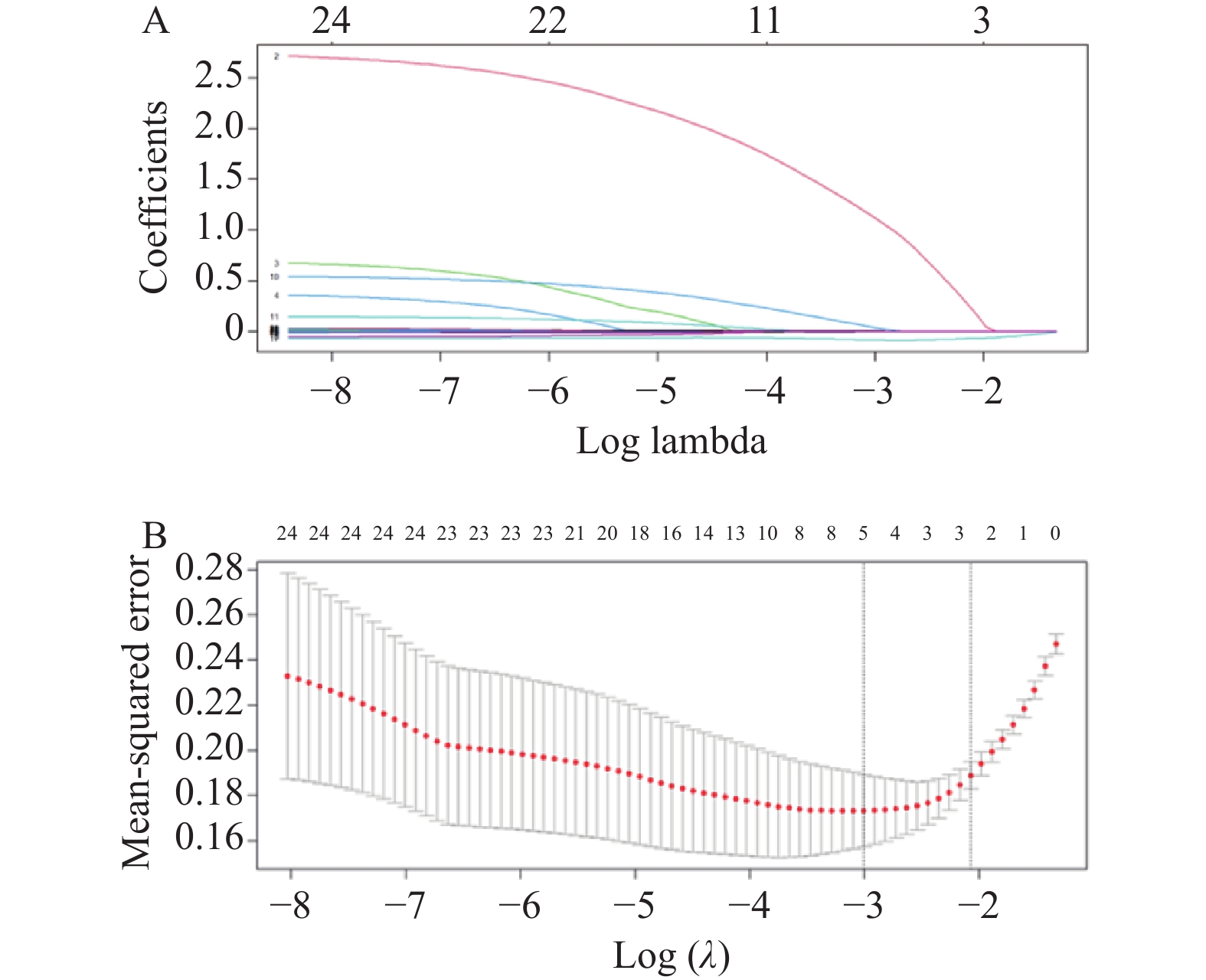
图 1 原发性肝癌干预前并发慢性肝衰竭的Lasso回归模型
A:系数筛选图;B:变量系数图。
Figure 1. Lasso regression model for primary liver cancer complicated with chronic liver failure before intervention
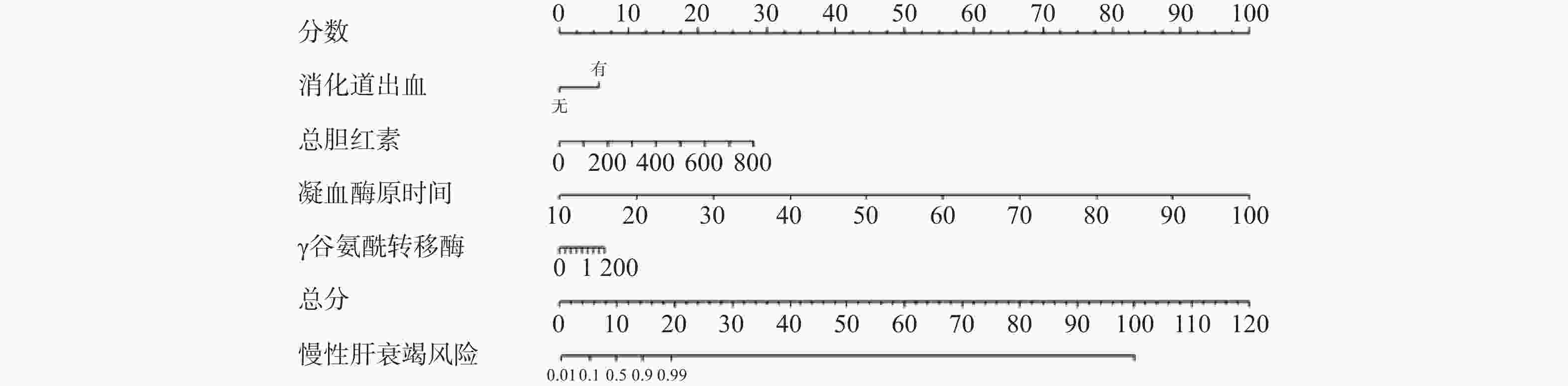
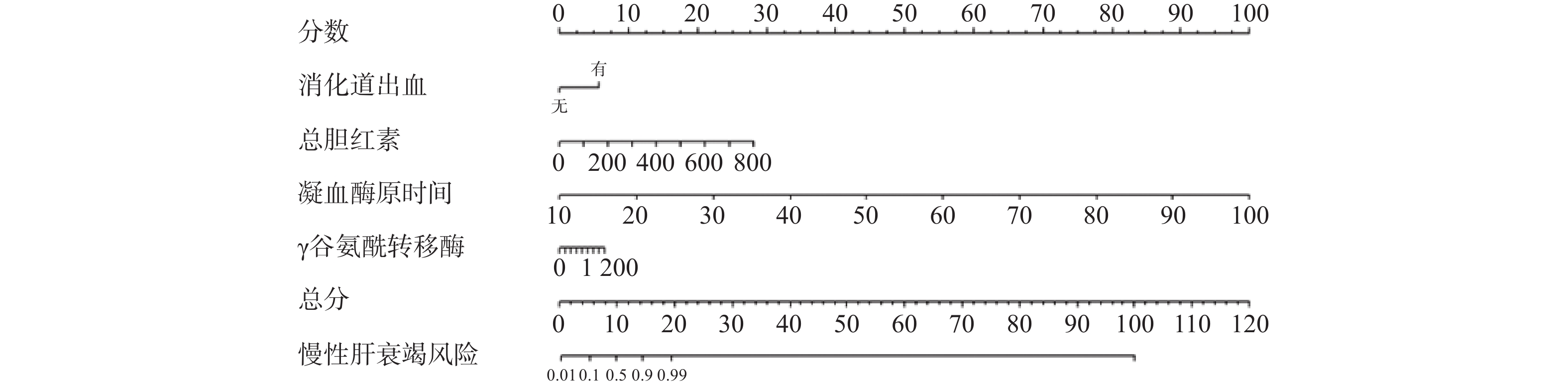
图 2 原发性肝癌干预前并发慢性肝衰竭的列线图模型
Figure 2. A nomogram model of chronic liver failure before primary liver cancer intervention
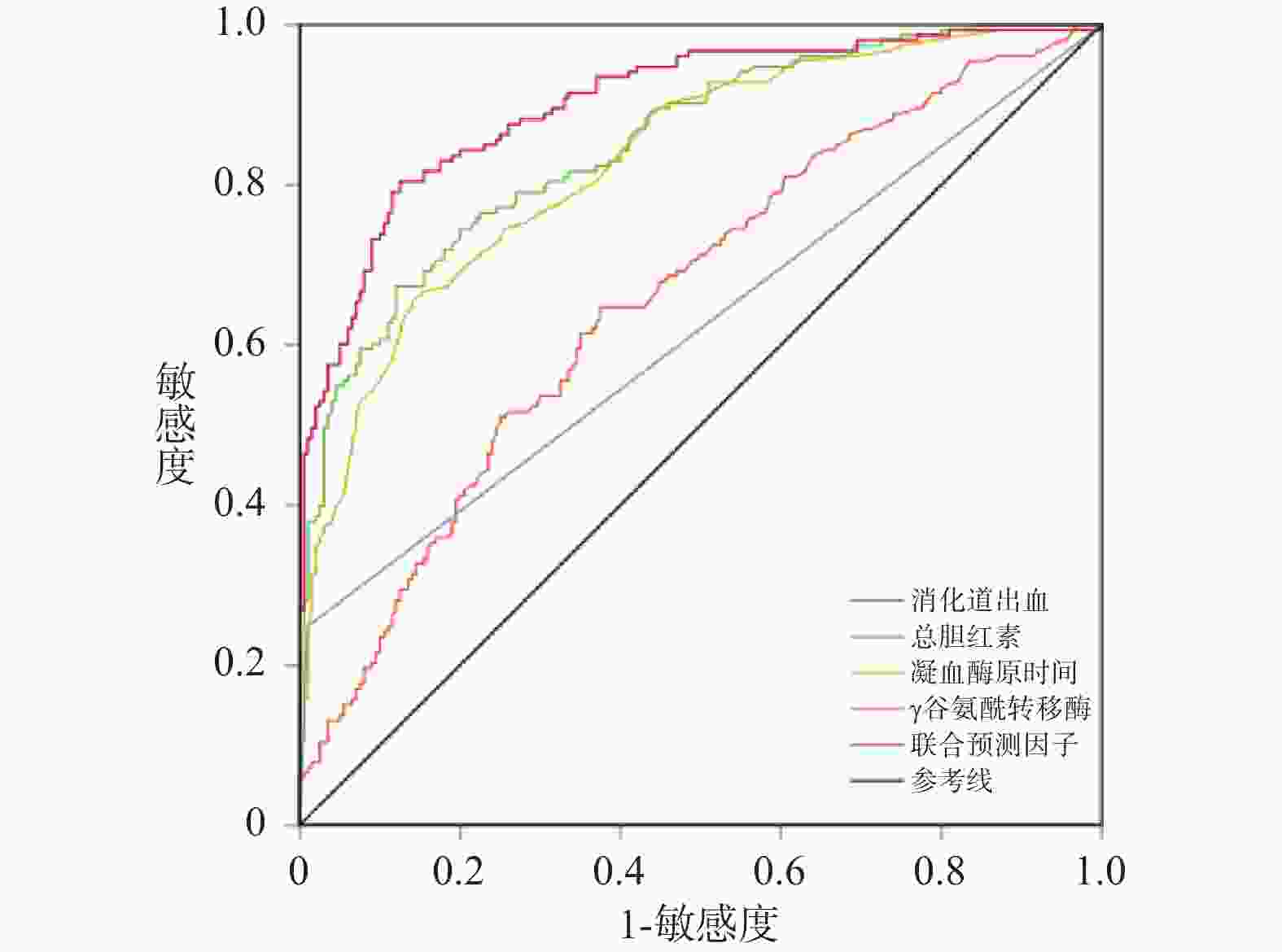
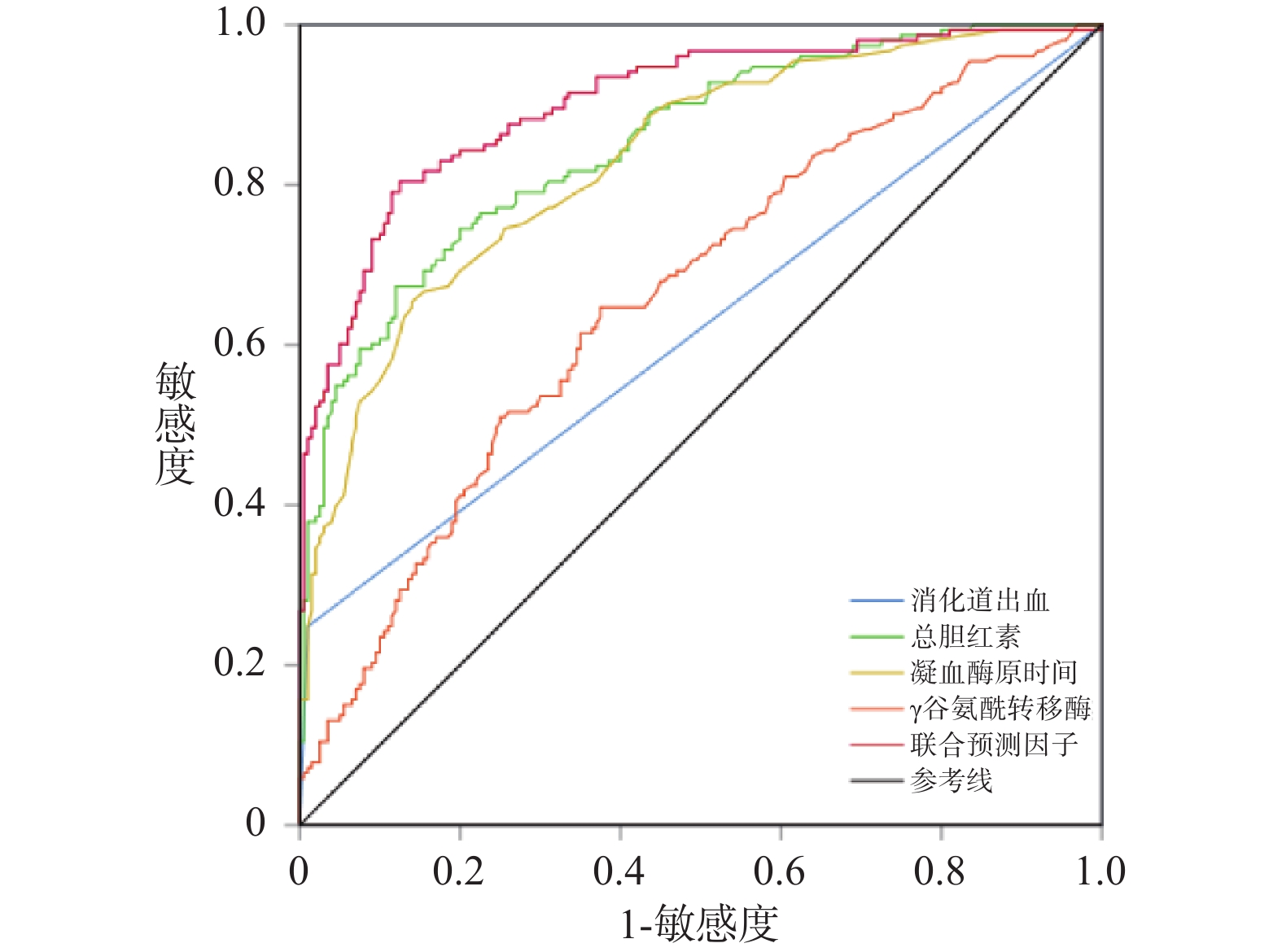
图 3 单项指标与联合指标预测原发性肝癌干预前并发慢性肝衰竭的ROC曲线
Figure 3. ROC curve of single and combined indicators predicting chronic liver failure before intervention of primary liver cancer
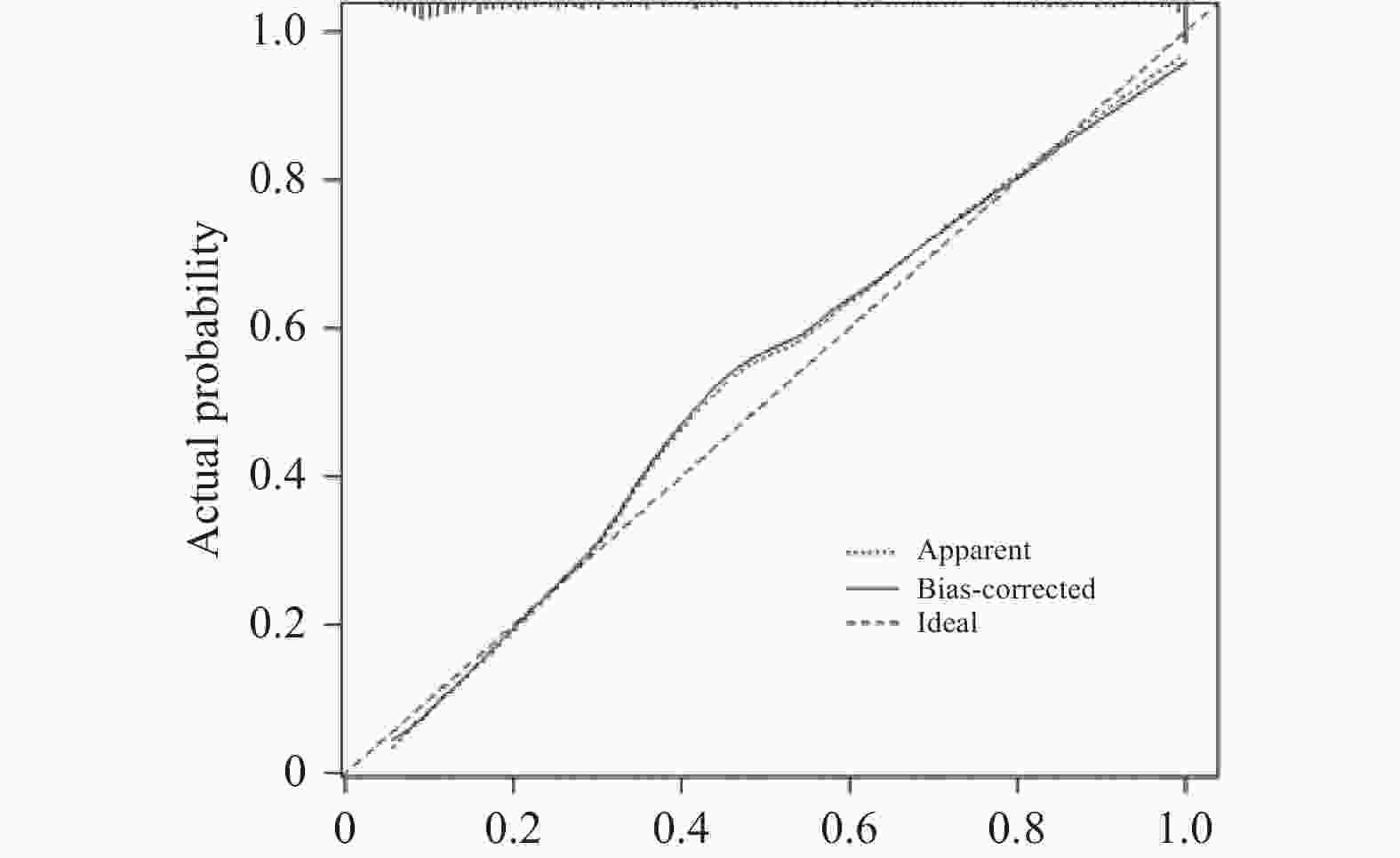
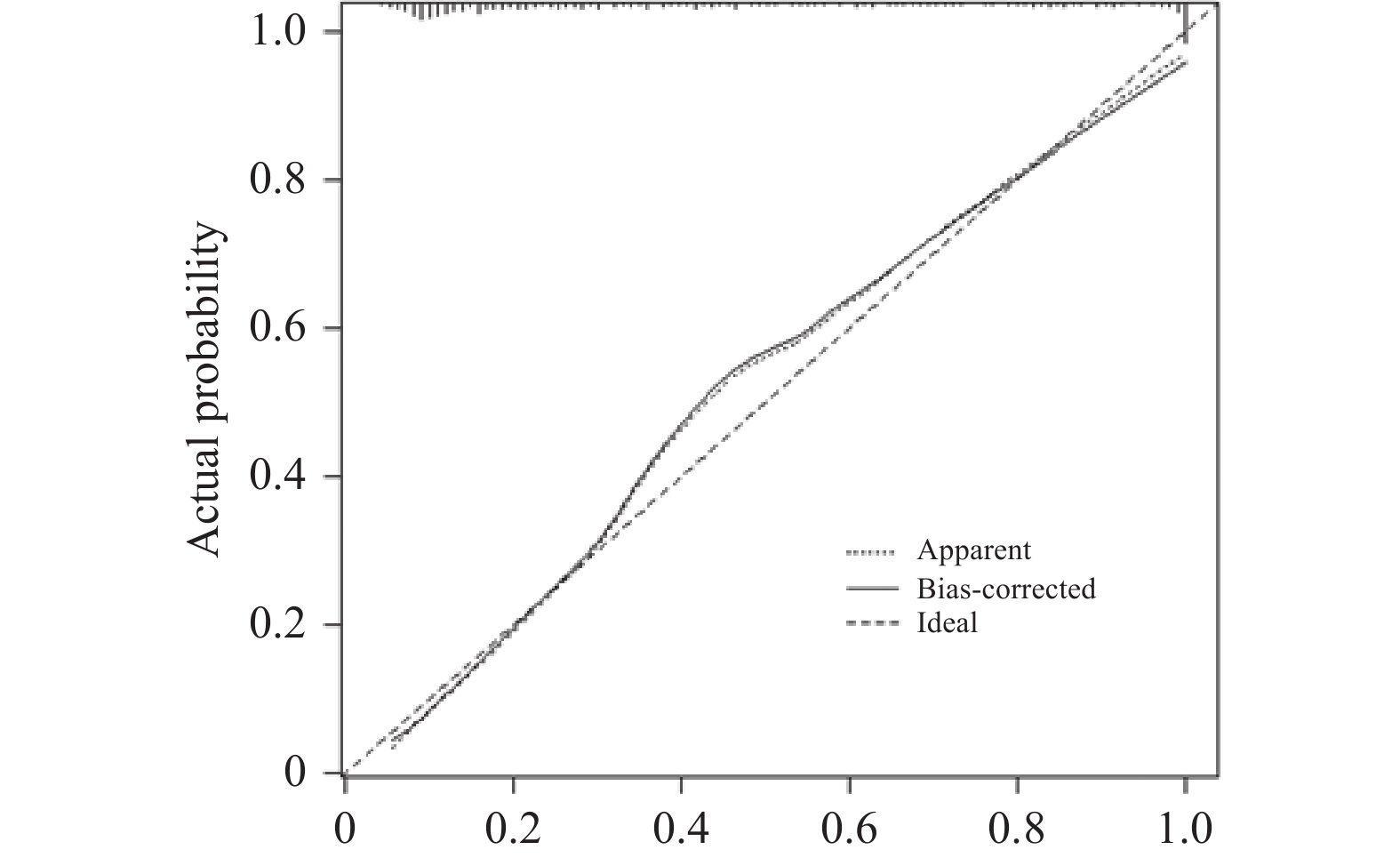
图 4 列线图模型预测原发性肝癌干预前并发慢性肝衰竭的校准曲线
Figure 4. Calibration curve of a nomogram model predicting chronic liver failure before intervention for primary liver cancer
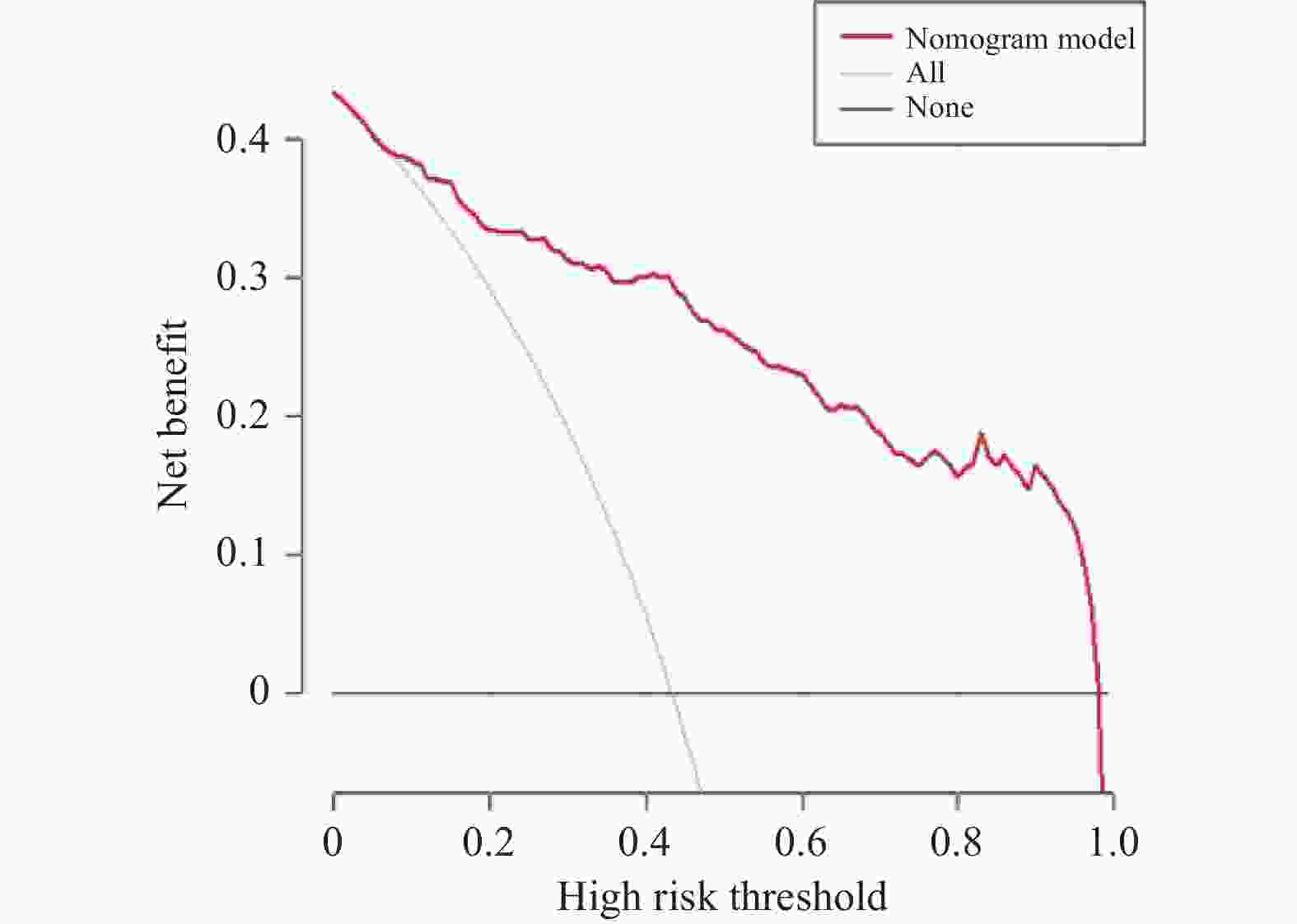
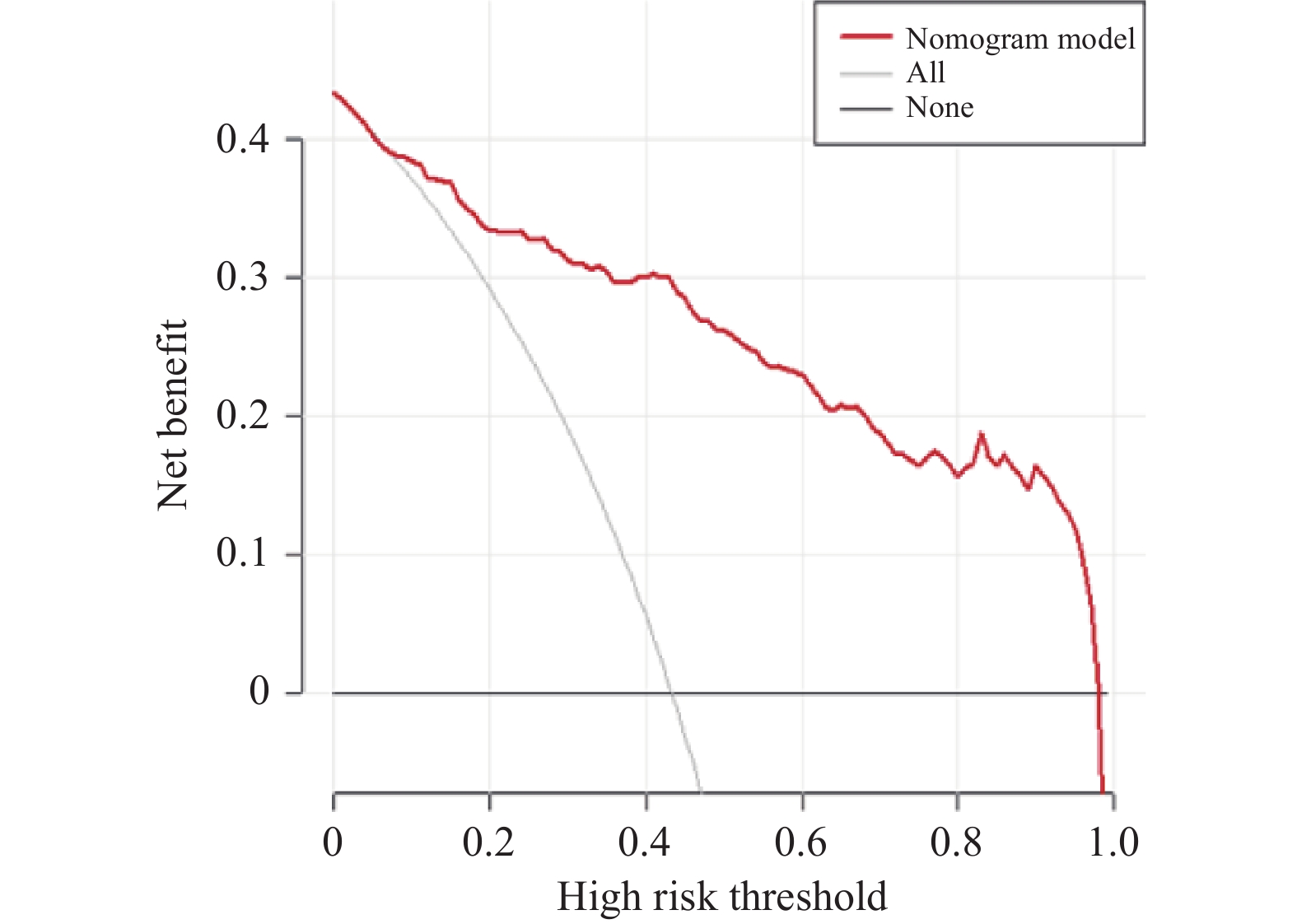
图 5 列线图模型预测原发性肝癌干预前并发慢性肝衰竭的临床决策曲线
Figure 5. The clinical decision curve of a nomogram model predicting chronic liver failure before intervention for primary liver cancer
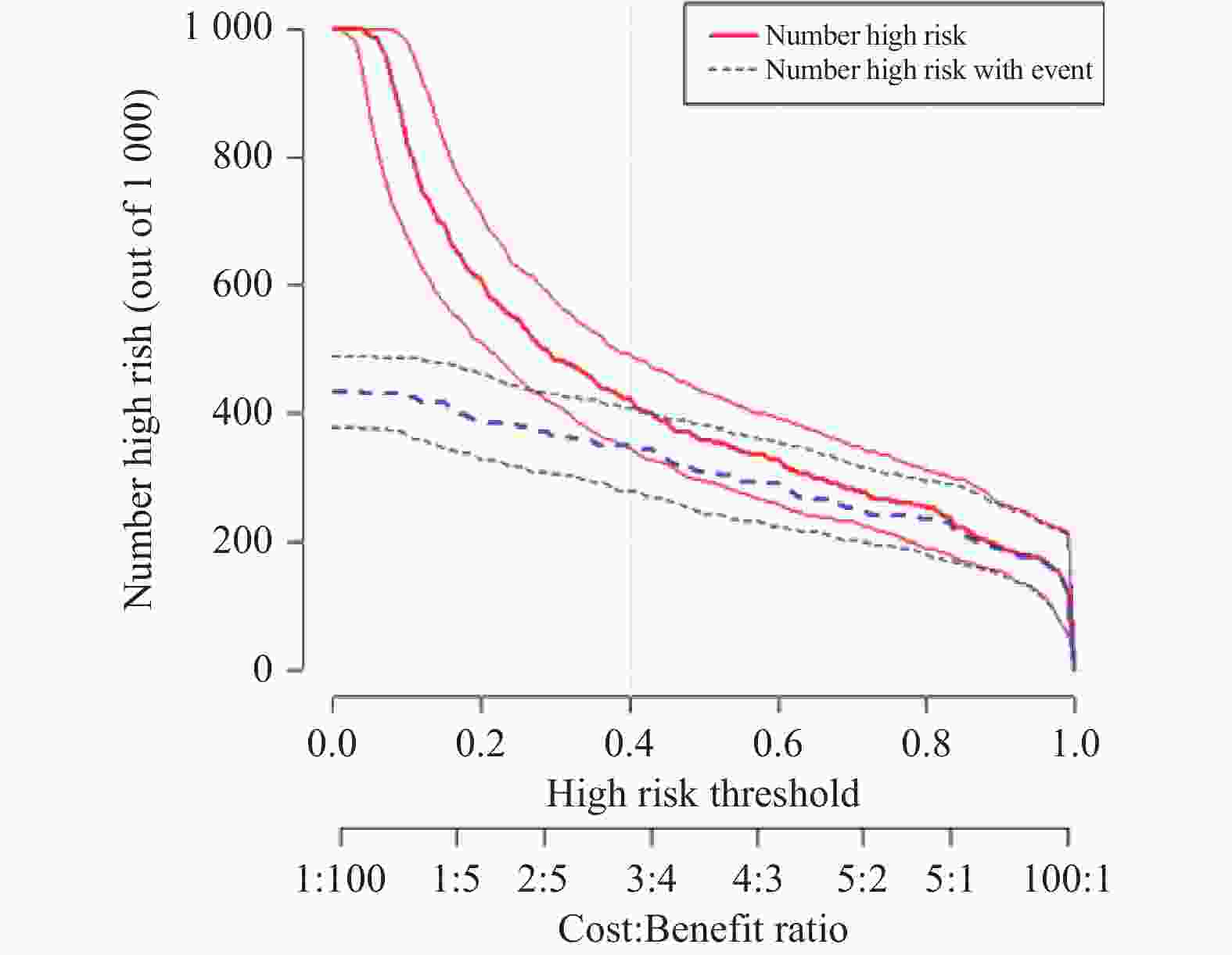
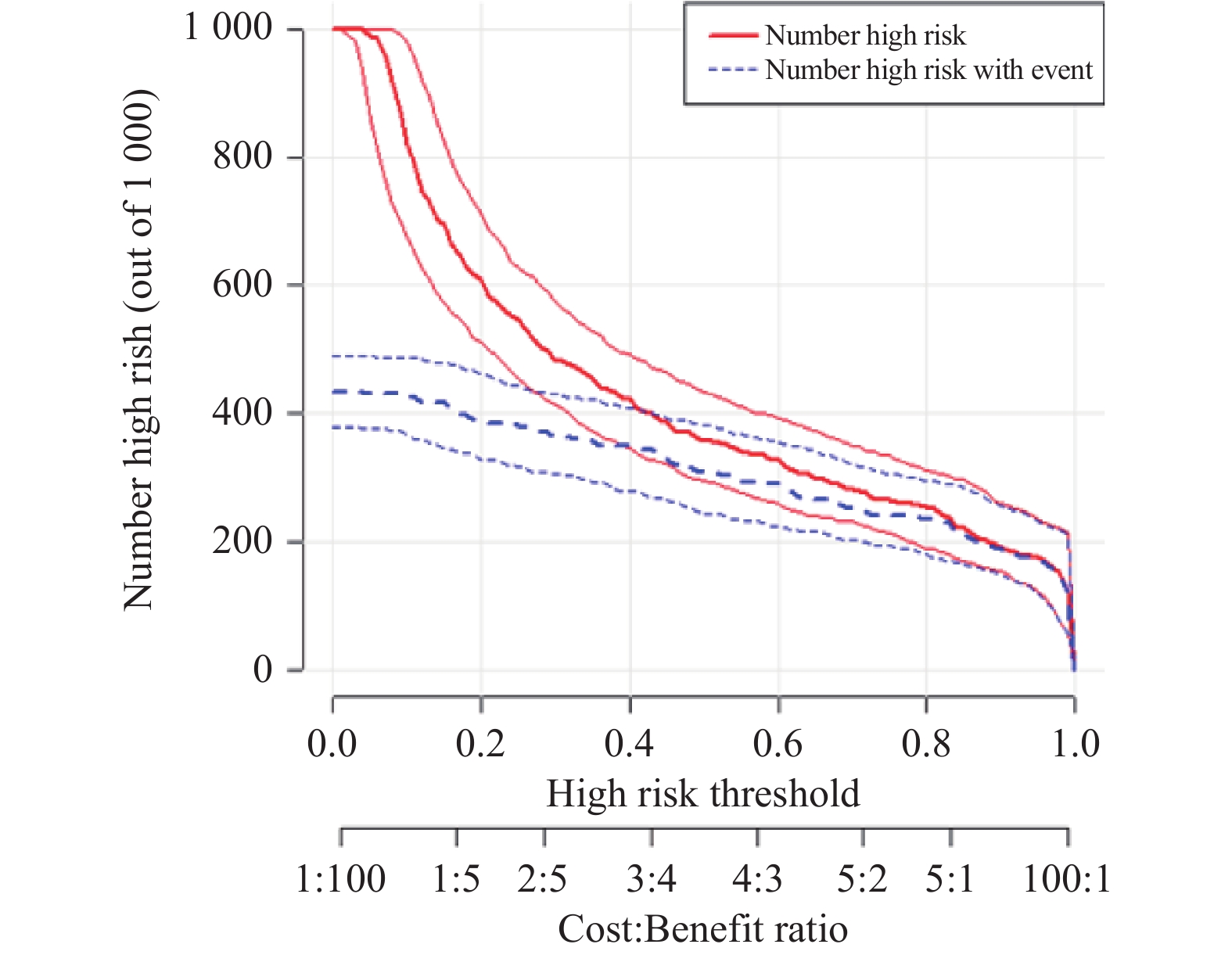
图 6 列线图模型预测原发性肝癌干预前并发慢性肝衰竭的临床影响曲线
Figure 6. The clinical impact curve of a nomogram model predicting chronic liver failure before intervention for primary liver cancer
表 1 353例原发性肝癌患者的一般资料分析[n(%)/M(P25,P75)/ $\bar x \pm s$]
Table 1. General data analysis of 353 patients with primary liver cancer [n(%)/M(P25,P75)/ $\bar x \pm s$]
指标 肝衰竭组
n=153非肝衰竭组
n=200χ2/t/z P 性别 男性 130(85.0) 173(86.5) 0.167 0.682 女性 23(15.0) 27(13.5) 年龄(岁) 51.0(46.0,58.5) 55.0(49.0,62.0) 2.422 0.015* BMI(kg/m2) 22.66±2.77 22.25±2.77 1.375 0.170 饮酒 是 78(51.0) 89(44.5) 1.460 0.227 否 75(49.0) 111(55.5) CHB 是 100(65.4) 150(75.0) 3.899 0.048* 否 53(34.6) 50(25.0) CHC 是 41(26.8) 34(17.0) 4.973 0.026* 否 112(73.2) 166(83.0) 高血压 是 18(11.8) 37(18.5) 2.990 0.084 否 135(88.2) 163(81.5) 糖尿病 是 19(12.4) 30(15.0) 0.483 0.487 否 134(87.6) 170(85.0) 消化道出血 有 38(24.8) 2(1.0) <0.001* 无 115(75.2) 198(99.0) 肝癌转移 有 5(3.3) 2(1.0) 0.247 无 148(96.7) 198(99.0) *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 353例原发性肝癌患者的临床检测资料分析[M(P25,P75)]
Table 2. Analysis of clinical data of 353 patients with primary liver cancer[M(P25,P75)]
指标 肝衰竭组(n = 153) 非肝衰竭组(n = 200) z P WBC(×109/L) 5.79(4.07,8.38) 4.66(3.60,5.90) 4.422 0.015* Neu(×109/L) 4.06(2.33,6.23) 2.87(2.10,3.96) 4.265 <0.001* PT(s) 16.90(15.35,19.40) 14.3(13.73,15.58) 10.640 <0.001* FIB(g/L) 2.20(1.60,3.31) 2.94(2.37,3.59) 5.091 <0.001* TP(g/L) 63.10(56.90,68.10) 68.9(63.03,73.70) 6.415 0.065 ALB(g/L) 28.1(24.5,33.57) 38.70(34.23,42.95) 10.858 <0.001* TBIL (mmol/L) 64.30(30.80,149.75) 20.30(14.28,28.95) 11.322 <0.001* AST(U/L) 109.0(56.5,198.0) 42.0(32.0,65.5) 9.727 <0.001* ALT(U/L) 53.0(30.0,80.5) 33.0(23.0,49.0) 5.245 <0.001* GGT(U/L) 157.00(69.00,298.50) 78.50(41.25,156.50) 5.178 <0.001* ALP(U/L) 202.0(144.0,341.5) 136.5(104.0,197.0) 10.050 <0.001* AFP/(μg/L) 107.60(10.21, 7520.00 )17.90( 4.1475 ,468.43)5.478 <0.001* PCT(μg/L) 0.38(0.14,1.09) 0.13(0.06,0.30) 7.057 <0.001* hs-CRP/(mg/L) 24.80(7.57,45.85) 8.55(1.32,36.23) 4.577 <0.001* TC(mmol/L) 3.23(2.33,4.46) 3.8(3.27,4.49)) 4.086 <0.001* LDL(mmol/L) 1.90(1.34,2.88) 2.37(1.95,2.93) 3.531 <0.001* Cr(μmol/L) 64.00(54.80,81.50) 65.00(54.25,73.00) 0.809 0.419 UA(μmol/L) 299.0(223.5,381.5) 313.5(253.5,391.0) 1.376 0.169 GLU(mmol/L) 5.15(4.63,5.99) 5.40(5.03,6.12) 3.063 0.002* IL-6(ng/L) 52.33(16.70,105.49) 15.91(10.28,52.41) 5.149 <0.001* CD4+(106个/ L) 382.60(315.54,528.61) 441.67(363.91,596.75) 3.123 0.002* CD8+(106个/ L) 224.94(162.25,305.66) 293.48(197.08,439.52) 4.337 <0.001* * P < 0.05。
下载: 导出CSV
表 3 原发性肝癌干预前并发慢性肝衰竭危险因素Logistic分析
Table 3. Logistic analysis of risk factors for chronic liver failure complicated with primary liver cancer before intervention
指标 β SE Wald OR 95%CI P 消化道出血 2.606 0.787 10.975 13.549 2.899~63.322 0.001* PT(s) 0.469 0.113 17.308 1.599 1.282~1.995 <0.001* ALB(g/L) −0.029 0.027 1.173 0.971 0.921~1.024 0.279 TBIL(mmol/L) 0.016 0.005 10.028 1.016 1.006~1.025 0.002* GGT(U/L) 0.002 0.001 4.853 1.002 1.000~1.003 0.028* *P < 0.05。
下载: 导出CSV
表 4 原发性肝癌患者干预前并发慢性肝衰竭影响因素的ROC分析
Table 4. ROC analysis of influencing factors of chronic liver failure in patients with primary liver cancer before intervention
指标 AUC 95%CI 灵敏度 特异度 截断值 消化道出血 0.619 0.559~0.680 0.248 0.990 − PT(s) 0.830 0.788~0.873 0.654 0.860 16.05 TBIL(mmol/L) 0.852 0.812~0.891 0.673 0.880 37.80 GGT(U/L) 0.661 0.604~0.718 0.647 0.625 99.00 联合预测因子 0.902 0.869~0.934 0.804 0.875 −
下载: 导出CSV
-
[1] Rumgay H,Arnold M,Ferlay J,et al. Global burden of primary liver cancer in 2020 and predictions to 2040[J]. J Hepatol,2022,77(6):1598-1606. doi: 10.1016/j.jhep.2022.08.021 [2] Sun L,Yang Y,Li Y,et al. The past,present,and future of liver cancer research in china[J]. Cancer Lett,2023,574:216334. doi: 10.1016/j.canlet.2023.216334 [3] Ding Y,Feng M,Ma D,et al. The 20 years transition of clinical characteristics and metabolic risk factors in primary liver cancer patients from china[J]. Front Oncol,2023,13:1109980. doi: 10.3389/fonc.2023.1109980 [4] Lawrence P F,Hager E S,Harlander-Locke M P,et al. Treatment of superficial and perforator reflux and deep venous stenosis improves healing of chronic venous leg ulcers[J]. J Vasc Surg Venous Lymphat Disord,2020,8(4):601-609. doi: 10.1016/j.jvsv.2019.09.016 [5] 徐曼曼,李珊珊,杨颜榕,等. 2012至2021年北京佑安医院肝衰竭住院患者流行病学特征[J]. 中华肝脏病杂志,2024,32(1):49-57. doi: 10.3760/cma.j.cn501113-20220824-00433 [6] Sarin S K,Choudhury A,Sharma M K,et al. Acute-on-chronic liver failure: Consensus recommendations of the asian pacific association for the study of the liver (apasl): An update[J]. Hepatol Int,2019,13(4):353-390. doi: 10.1007/s12072-019-09946-3 [7] Mahmud N,Hubbard R A,Kaplan D E,et al. Risk prediction scores for acute-on-chronic liver failure development and mortality[J]. Liver Int,2020,40(5):1159-1167. doi: 10.1111/liv.14328 [8] 尹鹏飞,黄桂忠,林巧红,等. 构建基于普美显增强MRI的肝切除术后肝衰综合预测模型[J]. 现代肿瘤医学,2023,31(16):3046-3050. doi: 10.3969/j.issn.1672-4992.2023.16.019 [9] 车汉洋,钟雅俊,陈志辉,等. 原发性肝癌患者术后并发肝衰竭的危险因素分析及nomogram预测模型构建[J]. 医学研究杂志,2023,52(5):163-166+143. [10] Merath K,Tiwari A,Court C,et al. Postoperative liver failure: definitions,risk factors,prediction models and prevention strategies[J]. J Gastrointest Surg,2023,27(11):2640-2649. doi: 10.1007/s11605-023-05834-2 [11] 中华人民共和国国家卫生健康委员会. 原发性肝癌诊疗指南(2022年版)[J]. 肿瘤综合治疗电子杂志,2022,8(2):16-53. [12] 中华医学会感染病学分会肝衰竭与人工肝学组,中华医学会肝病学分会重型肝病与人工肝学组. 肝衰竭诊治指南(2018年版)[J]. 临床肝胆病杂志,2019,35(1):38-44. doi: 10.3969/j.issn.1001-5256.2019.01.007 [13] 蒙荫杰,邱华,孟晨炜,等. 中西医结合治疗慢性肝衰竭规律及疗效的单中心回顾性研究[J]. 中西医结合肝病杂志,2023,33(6):484-487+495. doi: 10.3969/j.issn.1005-0264.2023.006.002 [14] 张丽丽,胡建华,汪九重,等. 酒精相关性慢性肝衰竭患者临床特点分析[J]. 肝脏,2022,27(09):963-965. [15] 董金玲,李璐,陈煜. 缓慢持续型慢加急性肝衰竭与慢性肝衰竭的甄别[J]. 实用肝脏病杂志,2021,24(5):611-612. doi: 10.3969/j.issn.1672-5069.2021.05.001 [16] 闫兰竹,乔顺义,张艳丽,等. 免疫球蛋白在肝癌tace治疗过程中的变化及预测疗效的价值[J]. 昆明医科大学学报,2024,45(04):128-134. [17] 周晶,杨艳芳,张艳洁,等. 原发性肝癌tace治疗后并发上消化道出血的原因及处理[J]. 医学综述,2018,24(4):698-702. doi: 10.3969/j.issn.1006-2084.2018.04.014 [18] 王亚飞,冯鹏远. 乙型肝炎肝硬化患者并发慢加急性肝衰竭的因素分析[J]. 四川生理科学杂志,2022,44(10):1798-1800+1846. [19] Gao Q,Qu X,Chen X,et al. Outcomes and risk factors of patients with acute fatty liver of pregnancy: a multicentre retrospective study[J]. Singapore Med J,2018,59(8):425-430. doi: 10.11622/smedj.2018001 [20] 王琦玮,杨鹏,韩明英,等. 山东省多中心picu收治的急性肝衰竭患儿病因、临床特点及预后影响因素[J]. 山东医药,2023,63(18):1-5. doi: 10.3969/j.issn.1002-266X.2023.18.001 [21] 魏明燕. 甲胎蛋白与血清凝血酶原时间联合诊断原发性肝癌的临床观察[J]. 临床医学工程,2018,25(2):185-186. doi: 10.3969/j.issn.1674-4659.2018.02.0185 [22] Jin D,Kang K,Yan B Z,et al. Combined age with mean decrease rates of total bilirubin and MELD score as a novel and simple clinical predictor on 90-day transplant-free mortality in adult patients with acute liver failure undergoing plasma exchange: A single-center retrospective study[J]. Can J Gastroenterol Hepatol,2023,2023:6115499. [23] Hafsa F,Chaudary Z I,Tariq O,et al. Acute-on-chronic liver failure: Causes,clinical parameters,and predictors of mortality[J]. Cureus,2024,16(1):e52690. [24] 宁琪琪,孟庆华,朱跃科. 肝癌术后肝脏再生与衰竭机制的研究进展[J]. 中华肝胆外科杂志,2018,24(3):214-216. doi: 10.3760/cma.j.issn.1007-8118.2018.03.019 [25] 赵惠临. 总胆红素与白蛋白比值对原发性肝癌自发性破裂出血患者预后的预测价值[J]. 山西医药杂志,2021,50(12):1976-1978. doi: 10.3969/j.issn.0253-9926.2021.12.028 [26] 马芝倩,杨立新,魏强,等. 超声引导下微波消融术对中晚期原发性肝癌患者血清tbil、dbil、alt水平的影响及安全性分析[J]. 现代医学与健康研究(电子版),2020,4(18):16-18. [27] 陈显荣,肖兵容,成浩. B超与血清d-二聚体、白蛋白和总胆红素水平评价肝硬化和向原发性肝癌转化时的临床价值[J]. 中国卫生检验杂志,2020,30(20):2489-2491. [28] Lv Y,Wang Z,Li K,et al. Risk stratification based on chronic liver failure consortium acute decompensation score in patients with child-pugh b cirrhosis and acute variceal bleeding[J]. Hepatology,2021,73(4):1478-1493. doi: 10.1002/hep.31478 [29] Yoshino K,Yoh T,Taura K,et al. A systematic review of prediction models for post-hepatectomy liver failure in patients undergoing liver surgery[J]. HPB (Oxford),2021,23(9):1311-1320. doi: 10.1016/j.hpb.2021.05.002 [30] 曾然,付松柏,周琳. 免疫球蛋白联合肝功能指标检测在肝衰竭诊断和预后判断中的价值[J]. 检验医学与临床,2018,15(16):2459-2461+2464. doi: 10.3969/j.issn.1672-9455.2018.16.029 [31] 范彦希. 免疫球蛋白与肝功能指标联合检测对肝衰竭的诊断价值[J]. 现代医学与健康研究(电子版),2020,4(3):119-121. [32] Qiu S,Jin L,Yang D,et al. Clinical application value of hepatitis b virus basal core promoter 1762/1764 and GGTII and GGT in patients with HBV-DNA-positive primary liver cancer[J]. Medicine (Baltimore),2023,102(43):e35699. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1274
- HTML全文浏览量: 663
- PDF下载量: 19
- 被引次数: 0
