

Predictive Value of FORCE Open Source CT Dual-energy Imaging in Preoperative Lymph Node Metastasis of Resectable Colon Cancer
-
摘要:
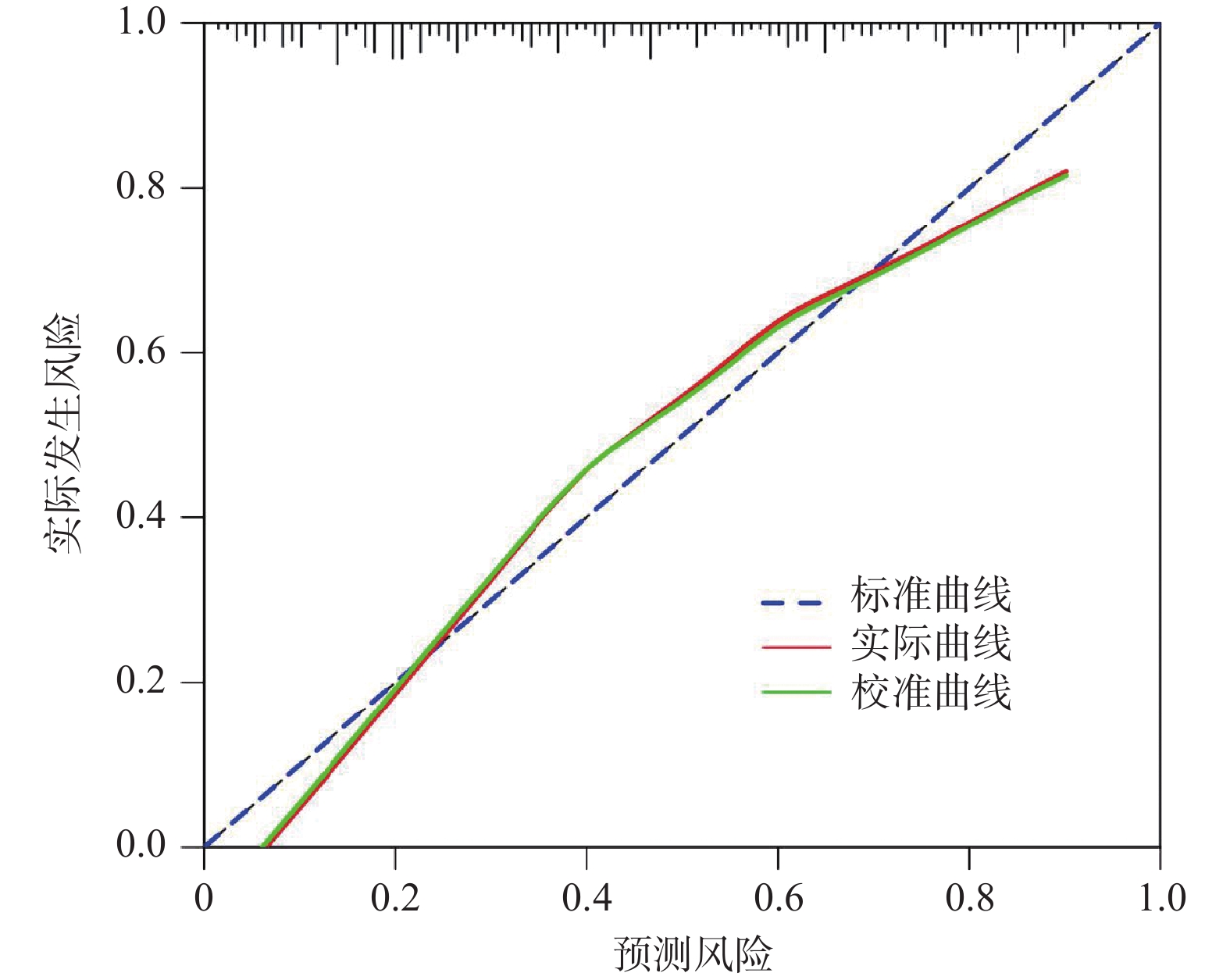
目的 探讨FORCE开源CT双能量成像在可切除结肠癌术前淋巴结转移中的预测价值。 方法 回顾性纳入绵阳市中心医院2021年1月至2025年2月213例可切除结肠癌患者作为研究对象,术前均行CT双能量成像,以术后病理检查为金标准,分为淋巴结转移组(n = 121)与无淋巴结转移组(n = 92)。比较两组临床资料、CT双能量成像参数差异,采用Lasso-Logistic回归分析术前淋巴结转移的影响因素,受试者工作特征(receiver operating characteristic,ROC)曲线分析CT双能量成像参数及联合参数对术前淋巴结转移的预测价值,并对预测效能进行外部验证。 结果 淋巴结转移组肿瘤直径大于无淋巴结转移组,肿瘤形态浸润型比例、低分化比例、脉管癌栓比例、肿瘤出芽分级BD3级比例高于无淋巴结转移组(P < 0.05);淋巴结转移组动脉期碘浓度(arterial iodine concentration,AIC)、动脉期标准化碘浓度(arterial normalized iodine concentration,ANIC)、动脉期能谱曲线斜率(arterial spectral curve slope,λHU-A)、动脉期电子云密度(arterial electron cloud density,Rho-A)、动脉期原子序数(arterial effective atomic number,Zeff-A)及静脉期碘浓度(venous iodine concentration,VIC)、静脉期标准化碘浓度(venous normalized iodine concentration,VNIC)、静脉期能谱曲线斜率(venous spectral curve slope,λHU-V)、静脉期电子云密度(venous electron cloud density,Rho-V)、静脉期原子序数(venous effective atomic number,Zeff-V)高于无淋巴结转移组(P < 0.05);Logistic回归分析,肿瘤直径、分化程度、脉管癌栓、AIC、λHU-A、Rho-A、Zeff-A、VIC、Rho-V与淋巴结转移独立相关(P < 0.05);ROC曲线分析,AIC、λHU-A、Rho-A、Zeff-A、VIC、Rho-V预测术前淋巴结转移的曲线下面积(area under curve,AUC)分别为0.726、0.758、0.763、0.719、0.727、0.784,联合预测AUC为0.893,校准曲线显示,模型预测概率与实际观测概率具有良好的一致性,Hosmer-Lemeshow χ2 = 5.683,P = 0.487,且外部验证显示,联合参数预测术前淋巴结转移的AUC为0.894,敏感度为84.62%,特异度为84.21%,模型预测概率与实际观测概率具有良好的一致性,Hosmer-Lemeshow χ2 = 5.418,P = 0.502。 结论 FORCE开源CT双能量成像AIC、λHU-A、Rho-A、Zeff-A、VIC、Rho-V与结肠癌术前淋巴结转移密切相关,对淋巴结转移具有一定预测价值。 Abstract:Objective To investigate the predictive value of FORCE open source CT dual energy imaging in preoperative lymph node metastasis of resectable colon cancer. Methods A retrospective study was performed to enroll 213 patients with resectable colon cancer who were admitted to Mianyang Central Hospital from January 2021 to February 2025. All patients underwent preoperative dual-energy computed tomography (CT) imaging. With postoperative pathological examination as the gold standard, the patients were divided into the lymph node metastasis group and the non-lymph node metastasis group. Clinical data and the differences in dual-energy CT imaging parameters between the two groups were compared. Lasso-Logistic regression analysis was applied to identify the influencing factors of preoperative lymph node metastasis. The receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive value of dual-energy CT imaging parameters and their combined parameters for preoperative lymph node metastasis, and external validation was carried out to verify the predictive efficacy. Results The lymph node metastasis group demonstrated a larger tumor diameter and higher rates of infiltrative morphology, poor differentiation, vascular tumor thrombus, and BD3-grade tumor budding than the non-lymph node metastasis group (P < 0.05). The arterial iodine concentration (AIC), arterial normalized iodine concentration(ANIC), arterial spectral curve slope (λHU-A), arterial electron cloud density (Rho-A), rterial effective atomic number (Zeff-A), venous iodine concentration (VIC), venous normalized iodine concentration (VNIC), venous spectral curve slope (λHU-V), venous electron cloud density (Rho-V), venous effective atomic number (Zeff-V) in lymph node metastasis group were higher than those in non-lymph node metastasis group (P < 0.05). Logistic regression analysis indicated that tumor diameter, differentiation grade, vascular tumor thrombus, AIC, λHU--A, Rho-A, Zeff-A, VIC, and Rho-V were independently associated with lymph node metastasis (P < 0.05). ROC curve analysis showed the area under the curve (AUC) values of AIC, λHU-A, Rho-A, Zeff-A, VIC, and Rho-V for predicting preoperative lymph node metastasis were 0.726, 0.758, 0.763, 0.719, 0.727, and 0.784, respectively, with the combined predictive model achieving an AUC of 0.893. Calibration curves showed good consistency between predicted and observed probabilities (Hosmer-Lemeshow χ2 = 5.683, P = 0.487). External validation confirmed the combined model had an AUC of 0.894, sensitivity of 84.62%, specificity of 84.21%, and excellent agreement between predicted and actual probabilities (Hosmer-Lemeshow χ2 = 5.418, P = 0.502). Conclusion AIC, λHU-A, Rho-A, Zeff-A, VIC and Rho-V obtained from FORCE open-source dual-energy CT are closely correlated with preoperative lymph node metastasis in colon cancer, and exhibit favorable predictive value for lymph node metastasis. -
Key words:
- Computer tomography /
- Colorectal cancer /
- Lymph node metastasis /
- Prediction
-
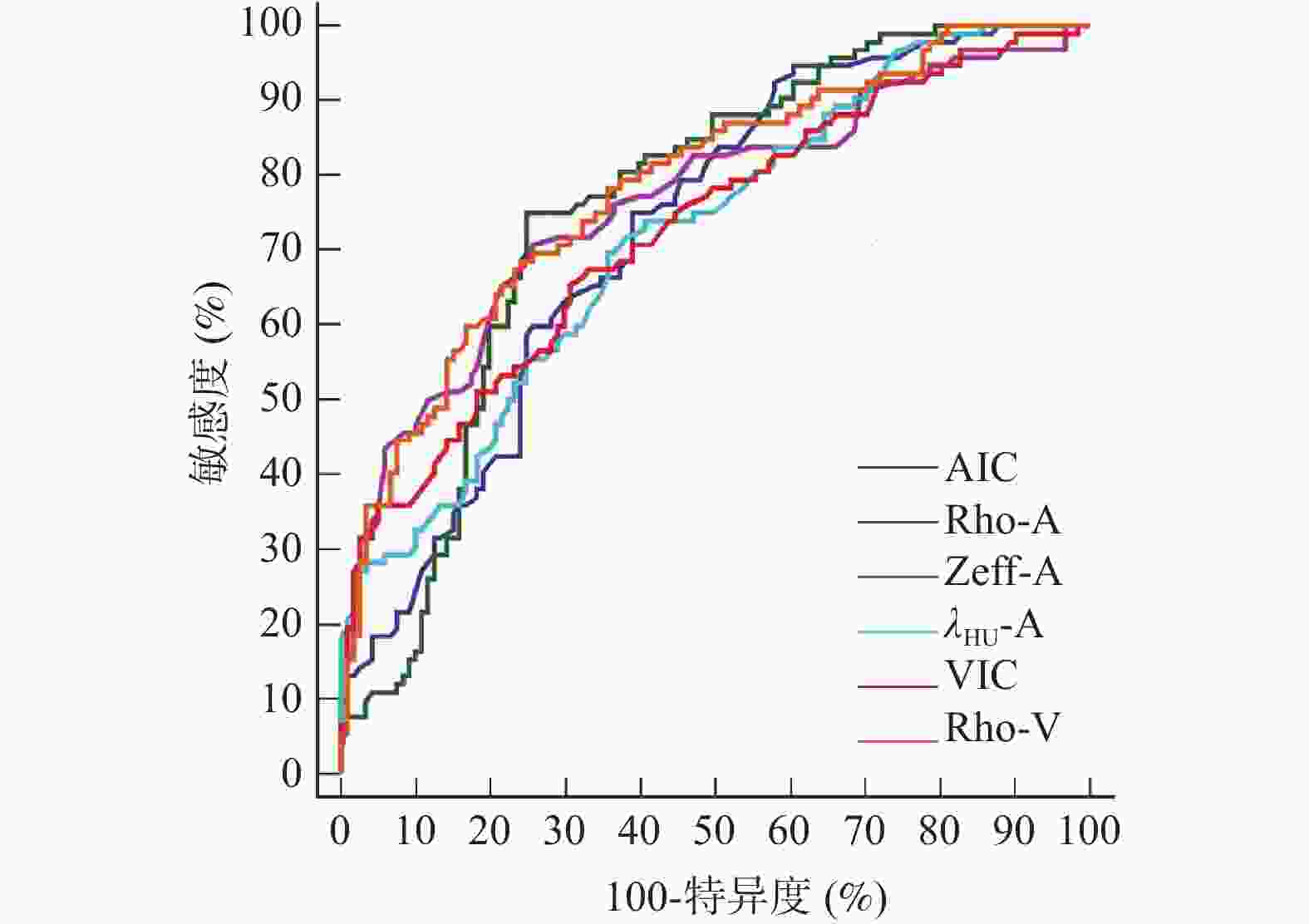
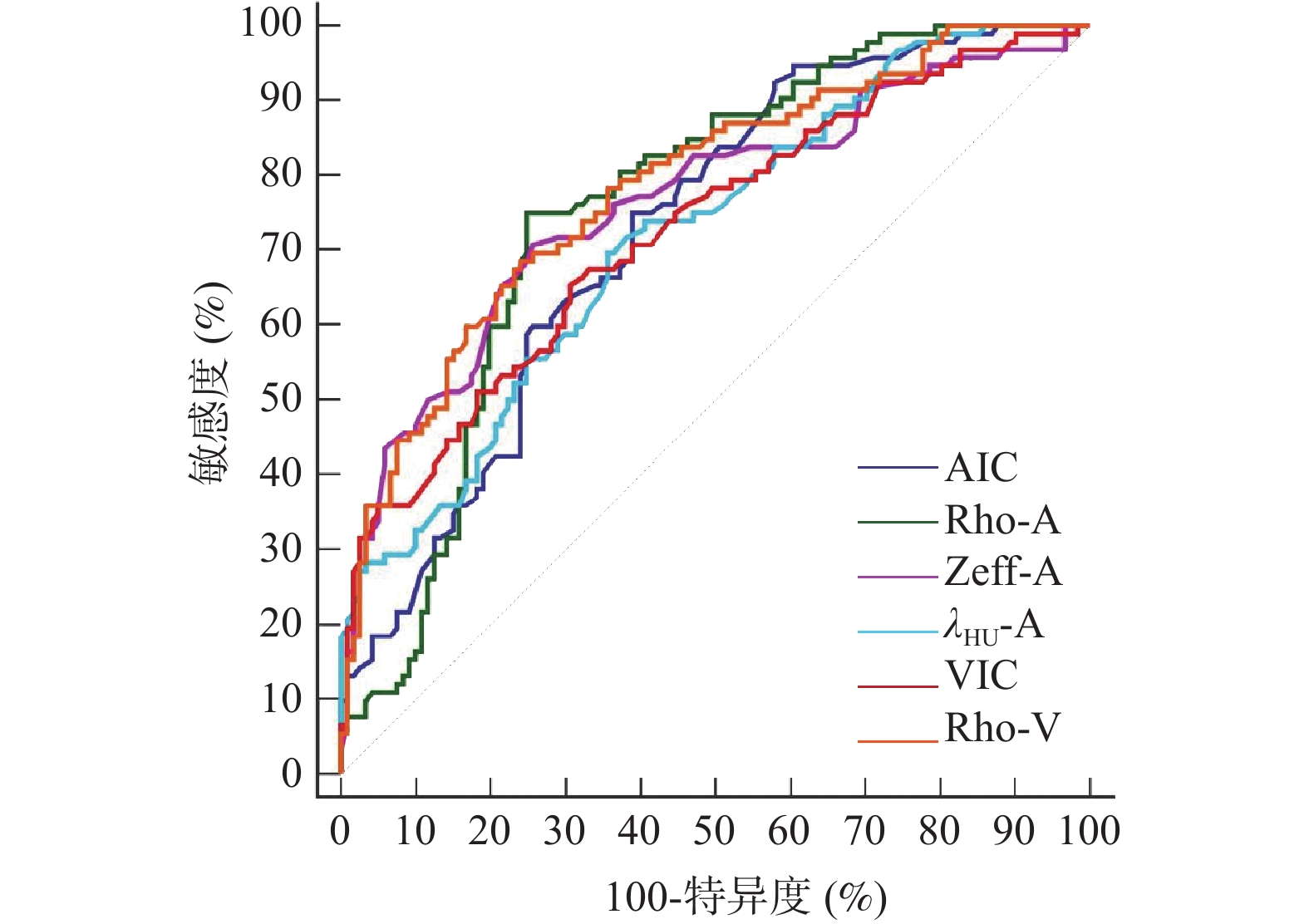
图 1 CT双能量成像参数预测结肠癌术前淋巴结转移的ROC曲线
Figure 1. ROC curves of dual-energy CT imaging parameters for predicting preoperative lymph node metastasis in colon cancer
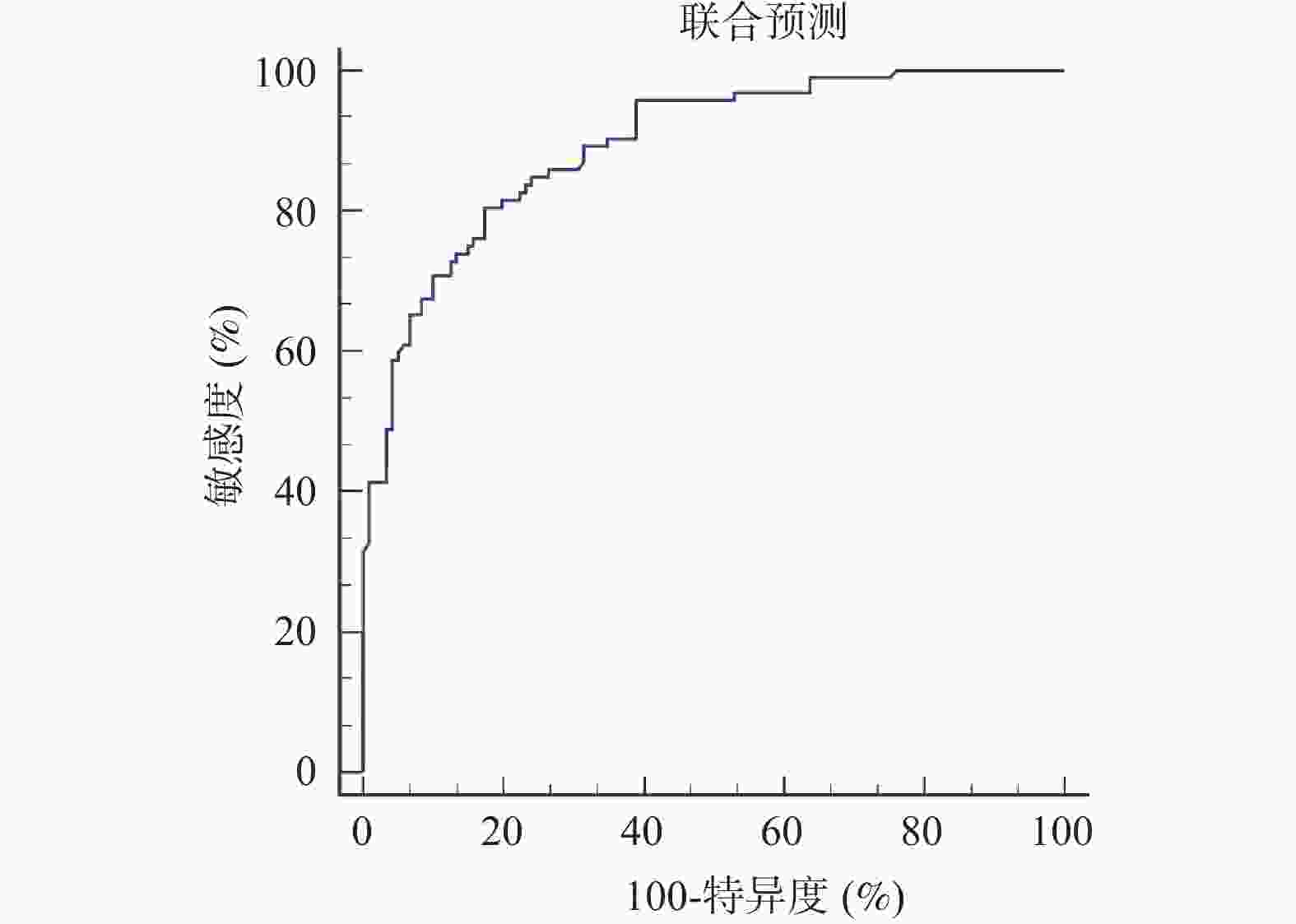
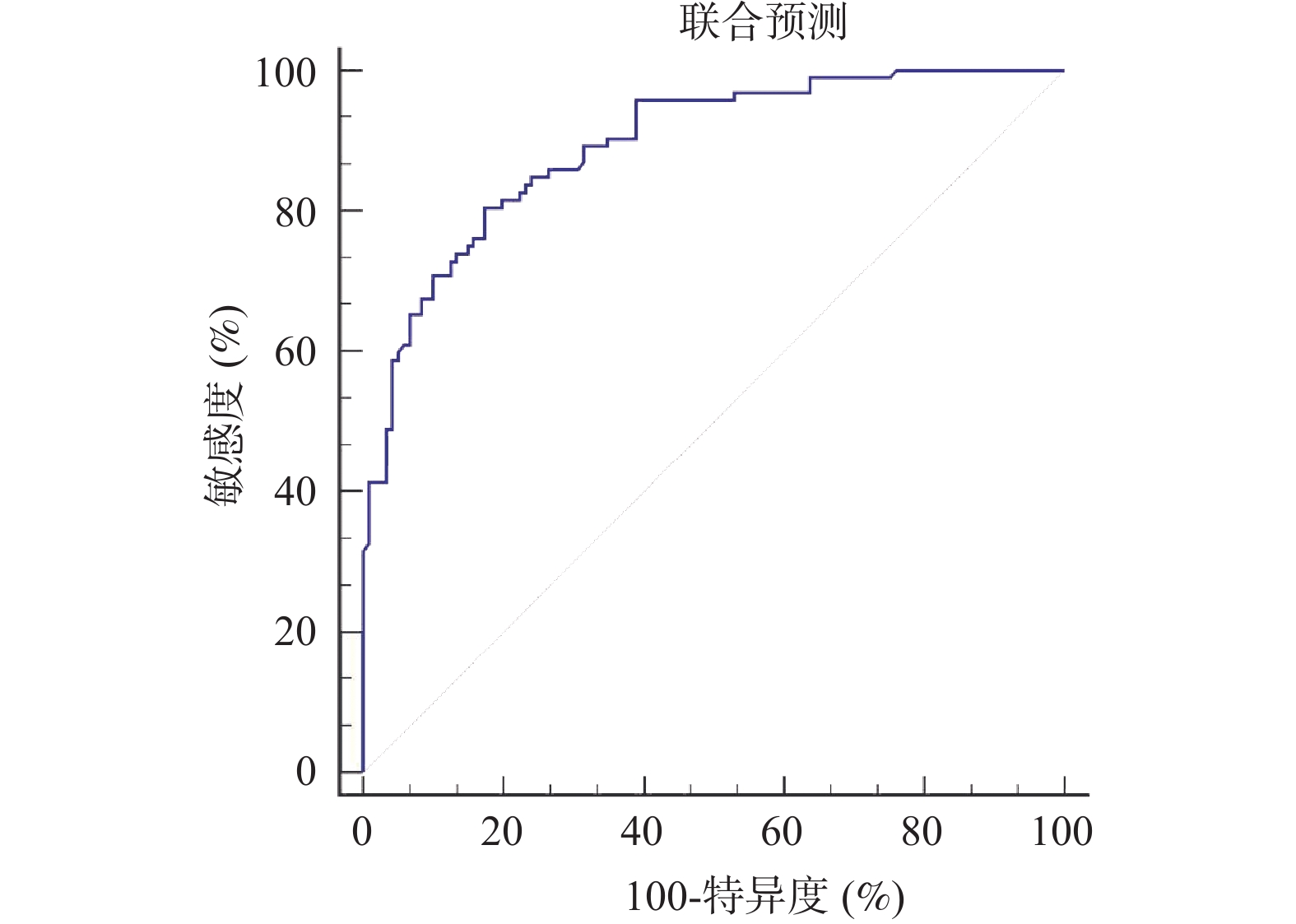
图 2 CT双能量成像参数与临床指标联合预测结肠癌术前淋巴结转移的价值
Figure 2. Value of combining dual-energy CT imaging parameters with clinical indicators for predicting preoperative lymph node metastasis in colon cancer
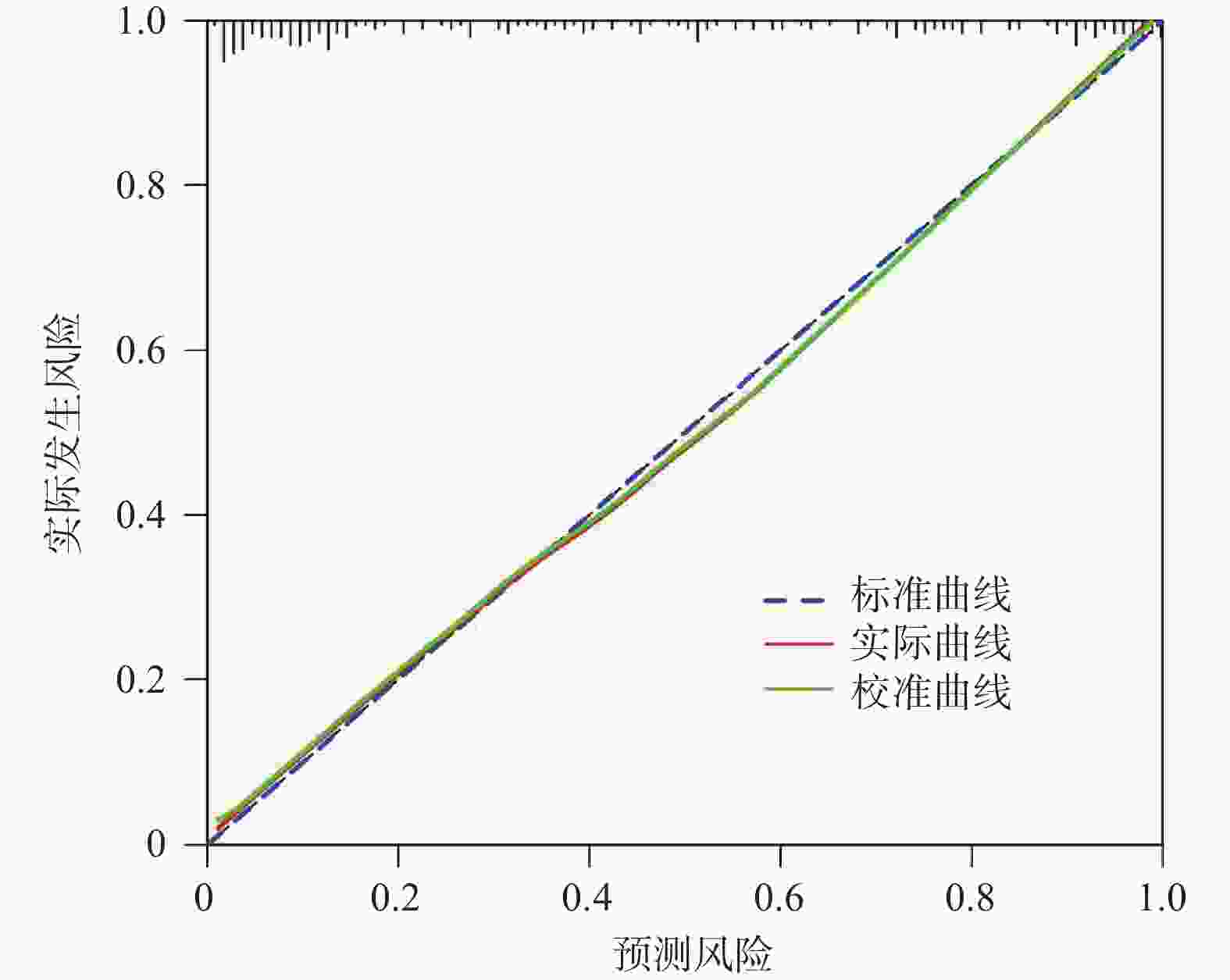
图 3 CT双能量成像参数与临床指标联合预测结肠癌术前淋巴结转移的校准曲线
Figure 3. Calibration curve of the combined prediction model (dual-energy CT parameters + clinical indicators) for preoperative lymph node metastasis in colon cancer
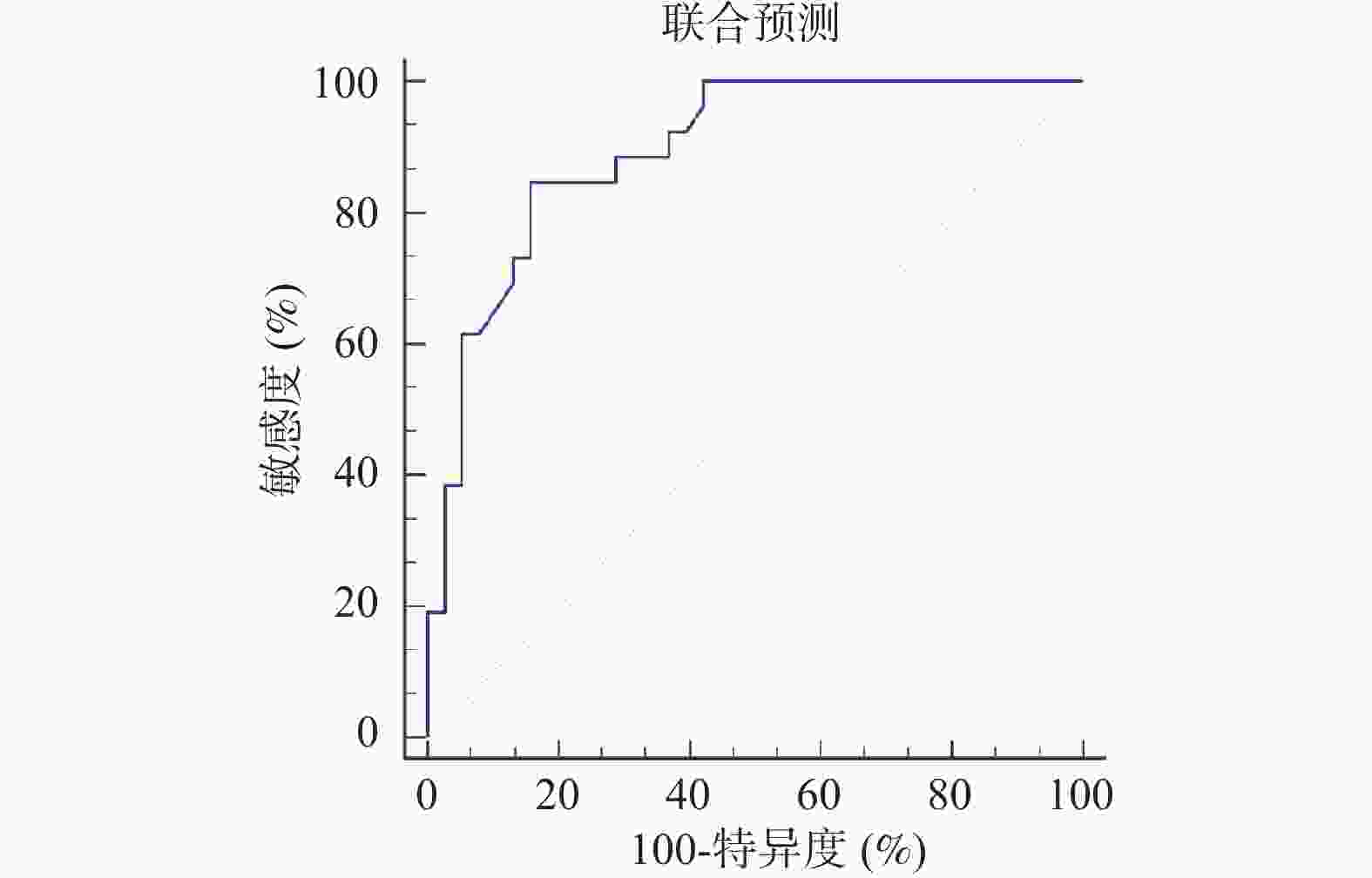
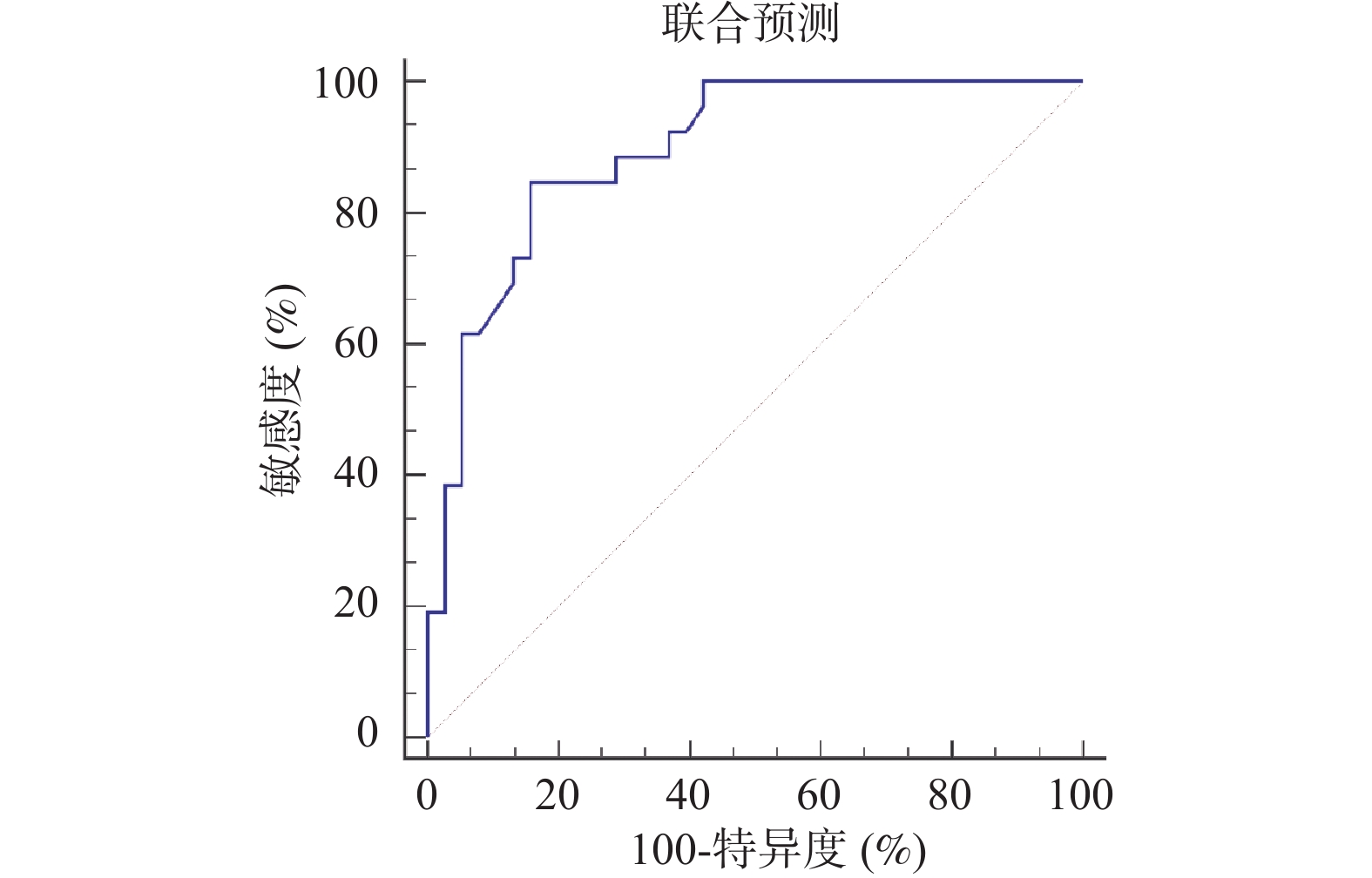
图 4 联合预测在外部验证集的ROC曲线
Figure 4. ROC curve of the combined prediction model in the external validation set
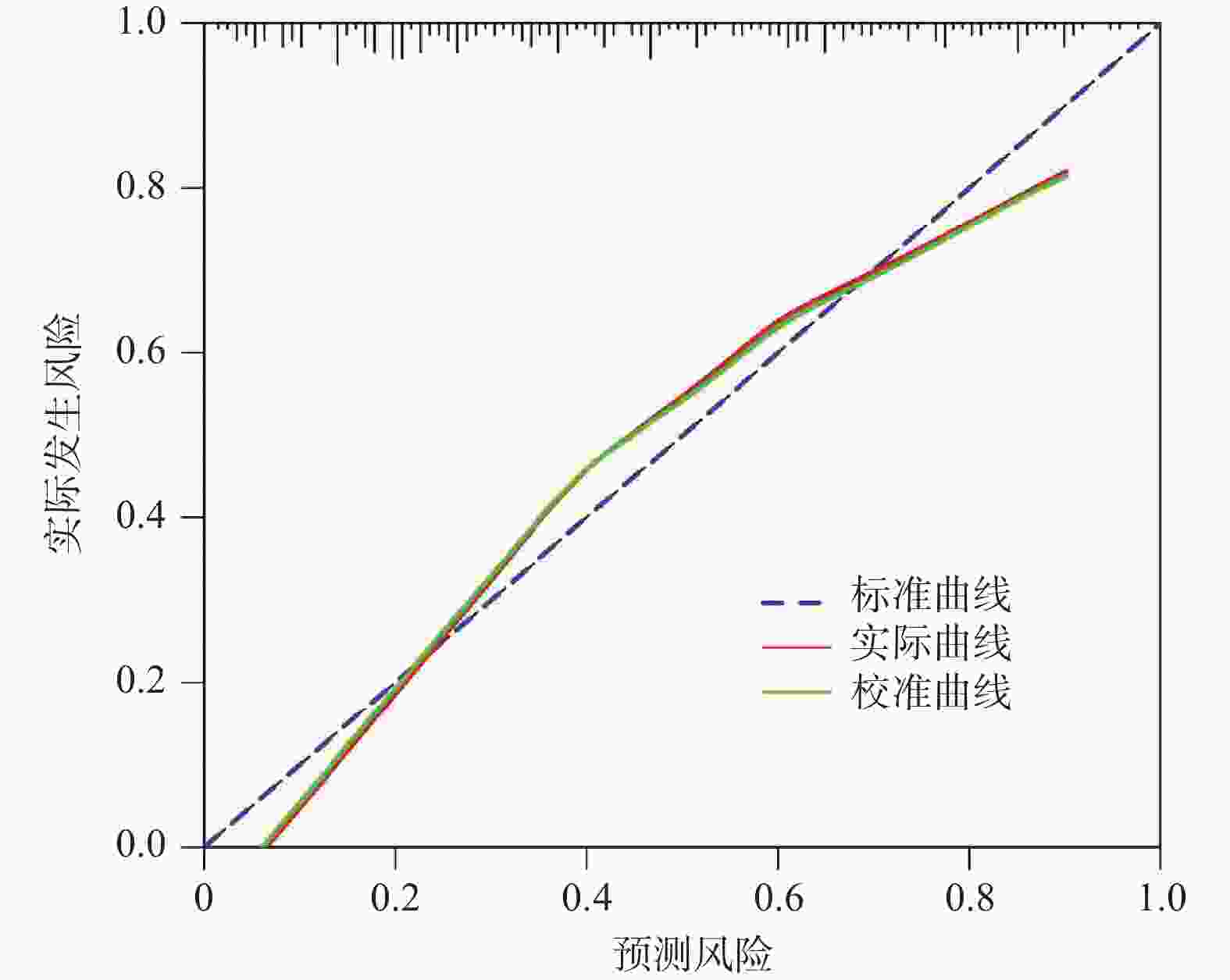
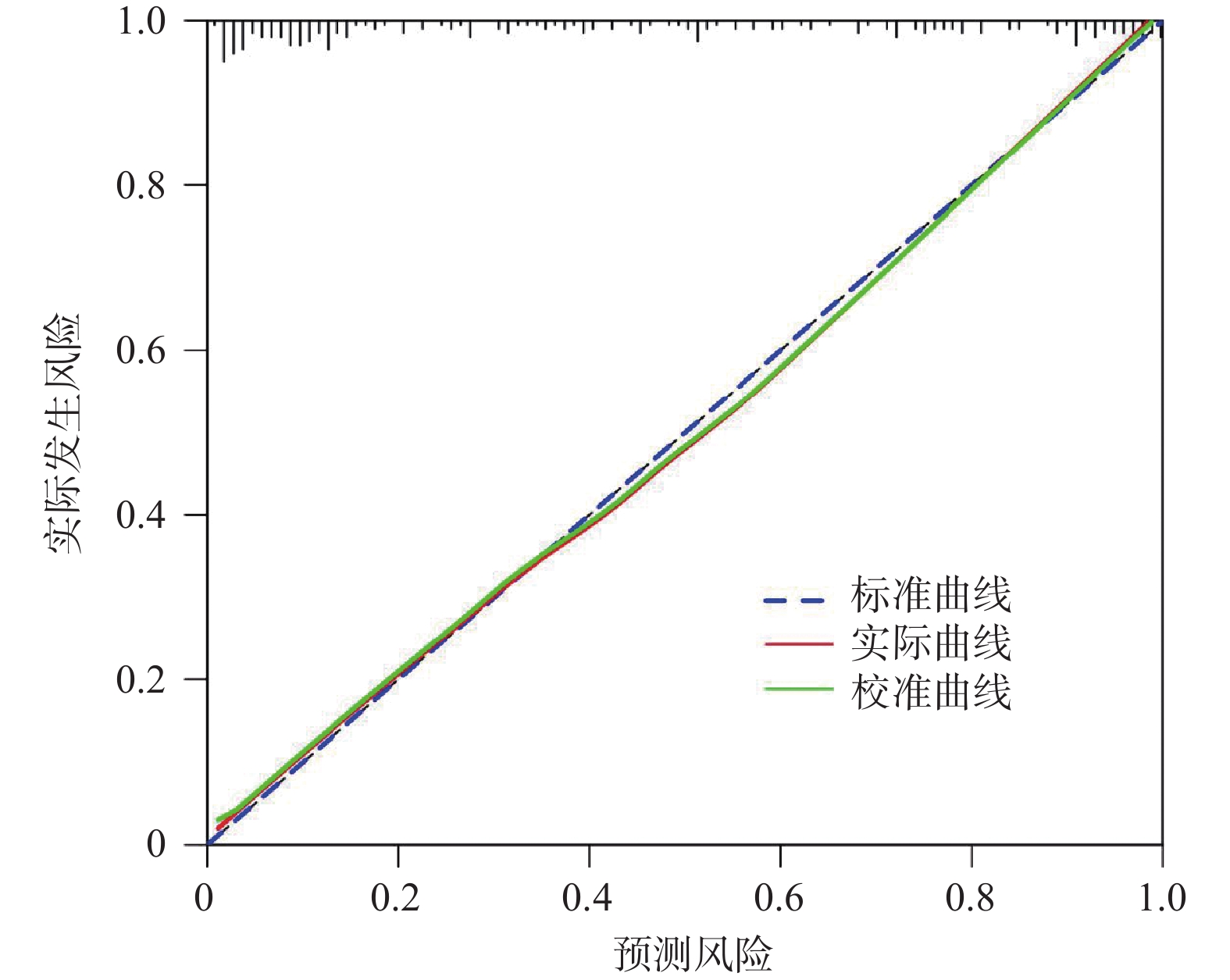
图 5 联合预测在外部验证集的校准曲线
Figure 5. Calibration curve of the combined prediction model in the external validation set
表 1 两组基线资料比较[n(%)/($ \bar x \pm s $)]
Table 1. Comparison of baseline characteristics between the two groups[n(%)/($ \bar x \pm s $)]
资料 淋巴结转移组(n = 92) 无淋巴结转移组(n = 121) t/χ2 P 性别 0.447 0.504 男 49(53.26) 70(57.85) 女 43(46.74) 51(42.15) 年龄(岁) 58.37 ± 6.29 56.94 ± 5.88 1.706 0.090* 体质量指数(kg/m2) 22.97 ± 1.13 23.15 ± 1.09 1.175 0.241 基础病 高血压 24(26.09) 26(21.49) 0.615 0.433 高脂血症 18(19.57) 29(23.97) 0.589 0.443 糖尿病 16(17.39) 31(25.62) 2.058 0.151 结肠癌家族史 0.757 0.384 有 10(10.87) 9(7.44) 无 82(89.13) 112(92.56) 肿瘤部位 0.166 0.684 左半结肠 40(43.48) 56(46.28) 右半结肠 52(56.52) 65(53.72) 肿瘤形态 7.158 0.028* 肿块型 22(23.91) 49(40.50) 溃疡型 38(41.30) 44(36.36) 浸润型 32(34.78) 28(23.14) 肿瘤直径(cm) 2.89 ± 0.52 2.21 ± 0.46 10.099 <0.001* 分化程度 7.739 0.005 中高分化 50(54.35) 88(72.73) 低分化 42(45.65) 33(27.27) 脉管癌栓 8.911 0.003* 有 21(22.83) 10(8.26) 无 71(77.17) 111(91.74) 肿瘤出芽分级 6.655 <0.001* BD1 18(19.57) 78(64.46) BD2 32(34.78) 31(25.62) BD3 42(45.65) 12(9.92) *P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 两组CT双能量成像参数比较($ \bar x \pm s $)
Table 2. Comparison of dual-energy CT imaging parameters between the two groups($ \bar x \pm s $)
CT双能量参数 淋巴结转移组(n = 92) 无淋巴结转移组(n = 121) t P 动脉期 AIC(mg/mL) 1.65 ± 0.54 1.46 ± 0.38 3.013 0.003* ANIC 0.17 ± 0.06 0.13 ± 0.04 5.827 <0.001* λHU-A 2.81 ± 0.92 2.24 ± 0.70 5.136 <0.001* Rho-A(HU) 37.82 ± 3.28 36.19 ± 3.02 3.759 <0.001* Zeff-A 8.31 ± 0.25 8.18 ± 0.21 4.120 <0.001* 静脉期 VIC(mg/mL) 2.52 ± 0.90 2.05 ± 0.64 3.462 0.001* VNIC 0.51 ± 0.18 0.43 ± 0.13 2.935 0.004* λHU-V 3.17 ± 0.87 2.88 ± 0.72 2.121 0.036* Rho-V(HU) 40.63 ± 3.52 38.55 ± 3.11 4.566 <0.001* Zeff-V 8.60 ± 0.31 8.41 ± 0.27 4.770 <0.001* *P < 0.05。
下载: 导出CSV
表 3 结肠癌术前淋巴结转移的Logistic回归分析
Table 3. Logistic regression analysis of preoperative lymph node metastasis in colon cancer
变量 β S.E. Waldχ2 P OR 95%CI 肿瘤直径 0.721 0.115 39.256 0.024* 2.056 1.641~2.575 分化程度 中高分化 1.000 低分化 1.160 0.108 115.428 <0.001* 3.191 2.582~3.943 脉管癌栓 1.187 0.146 66.137 0.010* 3.278 2.463~4.364 AIC 0.626 0.094 44.363 0.021* 1.870 1.556~2.249 Rho-A 0.791 0.103 58.936 0.015* 2.205 1.802~2.698 Zeff-A 0.836 0.126 44.048 0.021* 2.308 1.803~2.954 λHU-A 0.823 0.117 49.490 0.018* 2.278 1.725~3.007 VIC 0.685 0.098 48.884 0.019* 1.984 1.457~2.702 Rho-V 0.772 0.101 58.366 0.016* 2.163 1.663~2.814 常数项 −1.428 0.205 72.405 0.007* − − *P < 0.05。
下载: 导出CSV
表 4 CT双能量成像参数对结肠癌术前淋巴结转移的预测价值
Table 4. Predictive value of dual-energy CT imaging parameters for preoperative lymph node metastasis in colon cancer
指标 AUC 95%CI 截断 敏感度(%) 特异度(%) P AIC 0.726 0.661~0.785 1.52 75.00 61.16 <0.001* Rho-A 0.758 0.695~0.814 37.03 HU 75.00 75.21 <0.001* Zeff-A 0.763 0.700~0.818 8.25 70.65 74.38 <0.001* λHU-A 0.719 0.653~0.778 2.57 71.74 61.16 <0.001* VIC 0.727 0.662~0.785 2.38 65.22 69.42 <0.001* Rho-V 0.784 0.723~0.837 39.28 HU 68.48 76.03 <0.001* 联合预测 0.893 0.844~0.931 0.40 80.43 82.64 <0.001* *P < 0.05。
下载: 导出CSV
-
[1] 文家治, 向荣. 结肠癌术后吻合口瘘合并腹腔感染危险因素分析[J]. 临床误诊误治, 2024, 37(14): 59-63. [2] Abbaspour E, Karimzadhagh S, Monsef A, et al. Application of radiomics for preoperative prediction of lymph node metastasis in colorectal cancer: A systematic review and meta-analysis[J]. Int J Surg, 2024, 110(6): 3795-3813. doi: 10.1097/JS9.0000000000001239 [3] Kajiwara Y, Oka S, Tanaka S, et al. Nomogram as a novel predictive tool for lymph node metastasis in T1 colorectal cancer treated with endoscopic resection: A nationwide, multicenter study[J]. Gastrointest Endosc, 2023, 97(6): 1119-1128. e5. [4] Bian Y, Zheng Z, Fang X, et al. Artificial intelligence to predict lymph node metastasis at CT in pancreatic ductal adenocarcinoma[J]. Radiology, 2023, 306(1): 160-169. doi: 10.1148/radiol.220329 [5] Chu L C, Fishman E K. Artificial intelligence outperforms radiologists for pancreatic cancer lymph node metastasis prediction at CT[J]. Radiology, 2023, 306(1): 170-171. doi: 10.1148/radiol.222012 [6] 刘瑞华, 宗志恩. 双能量CT成像联合DCE-MRI在结肠癌术前评估中的应用[J]. 实用癌症杂志, 2023, 38(1): 122-125. doi: 10.3969/j.issn.1001-5930.2023.01.035 [7] Shao C, He C, Zheng P, et al. Preoperative prediction of tumor budding and lymphovascular invasion in colon cancer using dual-energy CT: a prospective study with internal model validation[J]. Abdom Radiol (NY), 2025, 50(8): 3406-3414. doi: 10.1007/s00261-025-04803-4 [8] 谭博文, 梁云, 陈环, 等. 术前外周血炎性指标联合肿瘤标记物对可切除结肠癌患者的预后价值[J]. 昆明医科大学学报, 2024, 45(12): 94-98. [9] 中华人民共和国国家卫生和计划生育委员会医政医管局, 中华医学会肿瘤学分会. 中国结直肠癌诊疗规范(2017年版)[J]. 中国实用外科杂志, 2018, 38(10): 1089-1103. doi: 10.19538/j.cjps.issn1005-2208.2025.12.01 [10] 吴晓凤, 许云华, 付广, 等. 新辅助化疗方案在可切除结肠癌中的应用进展[J]. 中国普通外科杂志, 2023, 32(4): 594-603. [11] Sugiura K, Seo Y, Tajima Y, et al. Prognostic impact of main lymph node metastasis in patients with colon cancer[J]. World J Surg, 2023, 47(5): 1292-1302. doi: 10.1007/s00268-023-06918-5 [12] Zeng P, Qu C, Liu J, et al. Comparison of MRI and CT-based radiomics for preoperative prediction of lymph node metastasis in pancreatic ductal adenocarcinoma[J]. Acta Radiol, 2023, 64(7): 2221-2228. doi: 10.1177/02841851221142552 [13] 郑穗敏, 翁志蓬, 欧建宏. 基于第三代双源CT force自动管电压的CCTA技术在冠心病诊断中的应用[J]. 海南医学, 2022, 33(22): 2940-2943. [14] Greffier J, Dabli D, Faby S, et al. Abdominal image quality and dose reduction with energy-integrating or photon-counting detectors dual-source CT: A phantom study[J]. Diagn Interv Imag, 2024, 105(10): 379-385. doi: 10.1016/j.diii.2024.05.002 [15] Jiang Y, Huang S, Tian Y, et al. Dual-time point 68Ga-FAPI-04 PET/CT improves tumor delineation and cervical lymph node metastasis identification in patients with head and neck squamous cell carcinoma[J]. Clin Nucl Med, 2025, 50(3): e130-e137. doi: 10.1097/RLU.0000000000005610 [16] Luo Y H, Mei X L, Liu Q R, et al. Diagnosing cervical lymph node metastasis in oral squamous cell carcinoma based on third-generation dual-source, dual-energy computed tomography[J]. Eur Radiol, 2023, 33(1): 162-171. doi: 10.1007/s00330-022-09033-6 [17] Zhou Y, Xu Y K, Geng D, et al. Added value of arterial enhancement fraction derived from dual-energy computed tomography for preoperative diagnosis of cervical lymph node metastasis in papillary thyroid cancer: Initial results[J]. Eur Radiol, 2024, 34(2): 1292-1301. [18] Geng D, Zhou Y, Shang T, et al. Effect of Hashimoto’s thyroiditis on the dual-energy CT quantitative parameters and performance in diagnosing metastatic cervical lymph nodes in patients with papillary thyroid cancer[J]. Cancer Imag, 2024, 24(1): 10-16. doi: 10.1186/s40644-024-00655-1 [19] Li M, Cui Y, Yan Y, et al. Dual energy CT-derived quantitative parameters and hematological characteristics predict pathological complete response in neoadjuvant chemoradiotherapy esophageal squamous cell carcinoma patients[J]. BMC Gastroenterol, 2025, 25(1): 357-366. doi: 10.1186/s12876-025-03964-2 [20] Li S, Wei X, Wang L, et al. Dual-source dual-energy CT and deep learning for equivocal lymph nodes on CT images for thyroid cancer[J]. Eur Radiol, 2024, 34(12): 7567-7579. doi: 10.1007/s00330-024-10854-w [21] Zhao W, Shen S, Ke T, et al. Clinical value of dual-energy CT for predicting occult metastasis in central neck lymph nodes of papillary thyroid carcinoma[J]. Eur Radiol, 2024, 34(1): 16-25. [22] Chen W, Lin G, Cheng F, et al. Development and validation of a dual-energy CT-based model for predicting the number of central lymph node metastases in clinically node-negative papillary thyroid carcinoma[J]. Acad Radiol, 2024, 31(1): 142-156. doi: 10.1016/j.acra.2023.04.038 [23] Liu K, Cao Y, Gao Y, et al. Utilizing spectral detector computed tomography quantitative parameters via multimodality tumor tracking to predict occult lymph node metastasis in clinical stage 1 pure solid lung adenocarcinoma[J]. J Thorac Dis, 2025, 17(5): 2912-2925. doi: 10.21037/jtd-24-1920 [24] 董晓蕾, 邵川洋, 刘杰克, 等. 双能量CT定量参数预测结肠癌高级别肿瘤出芽[J]. 临床放射学杂志, 2025, 44(7): 1270-1275. doi: 10.13437/j.cnki.jcr.2025.07.004 [25] Ren X F, Song Z H, Zhang D, et al. Differentiation of benign and malignant lesions in Bethesda III and IV thyroid nodules via dual-energy computed tomography quantitative parameters and morphologic features[J]. Quant Imaging Med Surg, 2024, 14(7): 4567-4578. doi: 10.21037/qims-23-1511 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 133
- HTML全文浏览量: 64
- PDF下载量: 18
- 被引次数: 0
